
FIGURE 1.
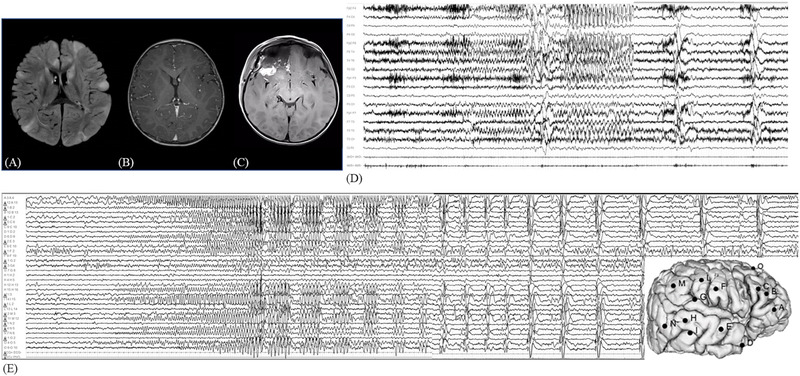
(A) Preoperative brain MRI showing multiple bilateral tubers with hyperintensity on FLAIR‐weighted sequences and subependymal nodules in T1‐sequence (B). (C) Postoperative brain MRI showing the resection area over the right fronto‐basal region. (D) Preoperative video‐EEG recording of right fronto‐temporal seizure with contralateral diffusion and followed by bilateral epileptic spasms. (E) SEEG recording of a focal seizure starting with a low‐voltage fast activity over electrodes B, C, and O, followed by rhythmic theta activity over the same electrodes and over electrode A. Then the ictal discharge involved temporal electrodes (D, E, H, M, and N). This discharge was followed by a cluster of clinically subtle epileptic spasms characterized by pseudorhythmic complexes of spikes, followed by a high‐voltage slow wave, mixed with fast activity evident at electrodes A3–4. EEG, electroencephalography; FLAIR, fluid attenuated inversion recovery; MRI, magnetic resonance imaging; SEEG, stereoelectroencephalography.