
Figure 2.
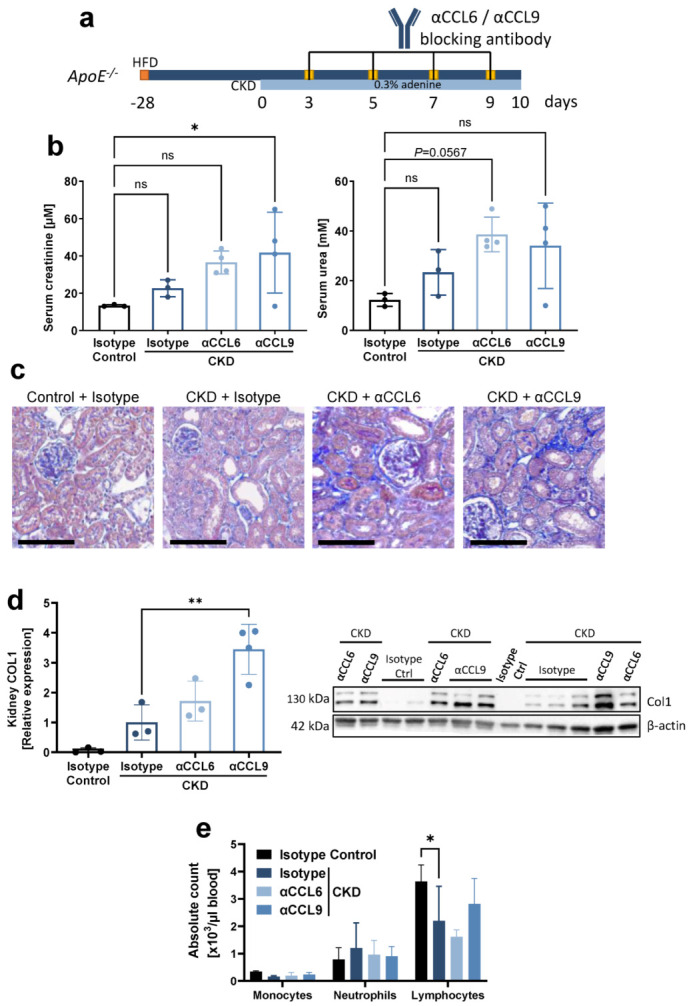
Systemic antibody-mediated blocking of CCL9 increases CKD-induced kidney fibrosis without effect on systemic inflammatory cells. Hyperlipidemic ApoE−/− mice with adenine-induced CKD were treated with blocking antibodies against CCL6 (αCCL6 CKD) or CCL9 (αCCL9 CKD), or with isotype-matched antibody controls (Isotype CKD), as indicated (n = 3–4). Hyperlipidemic ApoE−/− mice without adenine but with isotype-matched antibody treatment served as non-CKD controls (Isotype Control). (a) Experimental timeline. CKD = chronic kidney disease; HFD = high-fat diet. (b) Serum creatinine and urea at the end point. (c) Representative images of AFOG staining of kidney sections revealing kidney damage in all CKD conditions. Scale bar = 100 µm. (d) Quantification of collagen 1 (COL1) in kidney lysates by Western blot, normalized to β-actin and displayed relative to non-CKD controls. One value for ‘αCCL6 CKD’ excluded due to incomplete blotting (full Western blot images available online). (e) Leukocyte cell counts in peripheral blood. (b,d,e) Data represent means ± SD. Kruskal–Wallis test with Dunn’s post-test, one-way ANOVA with Dunnett’s post-test, or two-way ANOVA with Dunnett’s post-test for multiple comparisons, as appropriate. * p < 0.05; ** p < 0.01; ns = not significant.