

Abstract
Background
Bone foreign bodies are commonly encountered in small animal practice. Esophageal bone foreign bodies (E‐bFBs) warrant removal, whereas gastric bone foreign bodies might not.
Objectives
Describe management and outcomes for dogs with esophageal or gastric bone foreign bodies.
Animals
One hundred twenty‐nine dogs with esophageal (n = 45) or gastric (n = 84) bone foreign bodies.
Methods
Retrospective review of medical records.
Results
Dogs with E‐bFBs were younger than dogs with gastric bone foreign bodies (median age esophageal, 4 years [IQR 2‐8]; median age gastric, 6 years [IQR 3‐10]; P = .03), and had a higher bone cross‐sectional area relative to body weight (median esophageal, 98.21 mm2/kg [IQR 48.25‐142.6]; median gastric, 28.6 mm2/kg [IQR 17.25‐64.28]; P < .001). Forty‐two of 45 esophageal foreign bodies were resolved non‐surgically and 3 by esophagotomy. Esophageal erosions were more likely with distal entrapment (OR 12.88, [95% CI 31.95‐129.29], P = .01) and longer duration (OR 18.82 [95% CI 2.22‐273.97], P = .01). Sixty‐two of 84 bone gastric foreign bodies were left in situ. Endoscopic removal was successful in 20 of 22 (91%; 95% CI 70‐99) attempts.
Conclusions and Clinical Importance
While all E‐bFBs were dislodged either by advancement into the stomach, endoscopic removal, or esophagotomy, the majority of gastric bone foreign bodies were left in situ for dissolution, with no reported complications. Gastric advancement of E‐bFBs should be considered when oral removal is not feasible, and dissolution can be considered even with large bones.
Keywords: endoscopy, erosion, esophagus, stomach
Abbreviations
- B : BWI
bone : body weight index
- CI
confidence interval
- E‐bFB
esophageal bone foreign body
- G‐bFB
gastric bone foreign body
- IQR
interquartile range
- OR
odds ratio
1. INTRODUCTION
Gastrointestinal foreign bodies in dogs are a common emergency in small animal practice. Dogs frequently ingest bony material, including chicken bones and mammalian ribs, and these can be encountered as both esophageal and gastric foreign bodies. Bone is the most commonly reported esophageal foreign body in dogs, accounting for 30% to 80% of reported cases. 1 , 2 , 3 , 4 , 5 , 6 , 7 Although esophageal foreign bodies warrant urgent or emergency intervention regardless of their composition, in some studies, esophageal bone foreign bodies (E‐bFBs) appear to be more likely to traumatize the esophageal mucosa and carry a worse prognosis compared to other substances. 1 , 3 In another study, however, there was no association between type of esophageal foreign body and complication rate. 5
Gastric bone foreign bodies (G‐bFBs) have been studied less than E‐bFBs. In a case series of gastric and esophageal foreign bodies in 102 dogs, only 2 G‐bFBs were evaluated, 1 and in a retrospective evaluation of gastrointestinal foreign body surgeries, only 5 bones were identified in 208 cases. 8 Although bones can cause gastric perforation, 1 their higher digestibility compared to non‐organic foreign bodies is unique, supporting the argument to leave them in situ. 9 , 10 Despite potential complications associated with foreign material in the stomach, in some cases E‐bFBs actively or passively advanced into the stomach are considered successfully resolved. 3 , 4 , 5 A comparative evaluation of removal of the bone per os versus gastric advancement of the bony material has not been performed, and little data exist regarding outcomes of gastric bone digestion in dogs.
The objectives of this retrospective study were to (a) describe dog characteristics, bone attributes (bone type and number, duration, location, and relative size), and outcome, for dogs with esophageal or gastric bone foreign bodies removed by endoscopy, surgery, or advancement into the stomach; (b) determine factors associated with presence of esophageal erosions in dogs with E‐bFBs; and (c) determine factors associated with the decision to remove G‐bFBs.
2. MATERIALS AND METHODS
2.1. Study design, setting, and participants
This was a retrospective observational descriptive study. Radiology reports from dogs presented to the North Carolina State University Veterinary Hospital (NC State‐VH) between January 2005 and February 2019 were searched retrospectively for the terms “bone” and “foreign.” An initial database was generated, and the medical record of each case was examined. Inclusion criteria were foreign gastric or esophageal material consistent with bone, as assessed from the radiology report and clinical history, and a complete medical record. Exclusion criteria included absence of bone foreign body on review of images or radiographic report, bone foreign body in location other than esophagus or stomach, foreign bodies consisting of artificial bone‐like substances or rawhides, or cases in which induction of emesis successfully resolved the foreign body.
2.2. Variables and data sources
Using the electronic medical record, a database was constructed from the included cases. Age, breed, body weight, clinical signs, and the source of the ingested bone, if known, were recorded. The duration of time between a known ingestion and presentation was also recorded, and classified as peracute (<6 hours), acute (6‐48 hours), chronic (>48 hours), or incidental (dog was presented for a cause unrelated to the foreign body). Radiographs were examined and the location of the bone was recorded as proximal esophageal (from the oropharynx to the thoracic inlet), middle esophageal (from the thoracic inlet to the carina), distal esophageal (from the carina to the lower esophageal sphincter), or gastric (Figure 1). The bone cross‐sectional area was calculated with the aid of a digital linear measurement tool, by multiplying the longest identifiable length (mm) by the width (mm) in each available view and selecting the largest product. In some cases, because of differences in digital radiographic software between the primary care clinic and referral hospital, the linear measurement function was not available, and therefore bone cross‐sectional area was not calculated. Cross‐sectional areas were also not calculated for bone fragments measuring less than 5 mm in both dimensions. When more than 1 bone was present, the cross‐sectional areas of each were added together. A bone : body weight index (B : BWI) was calculated as total bone cross‐sectional area divided by body weight (kg). If body weight was not recorded or bone cross‐sectional area could not be calculated, the B : BWI was not calculated. The number of bones was recorded as 1 bone, 2 bones, >2 bones/bony fragments, or heterogeneous bony material.
FIGURE 1.
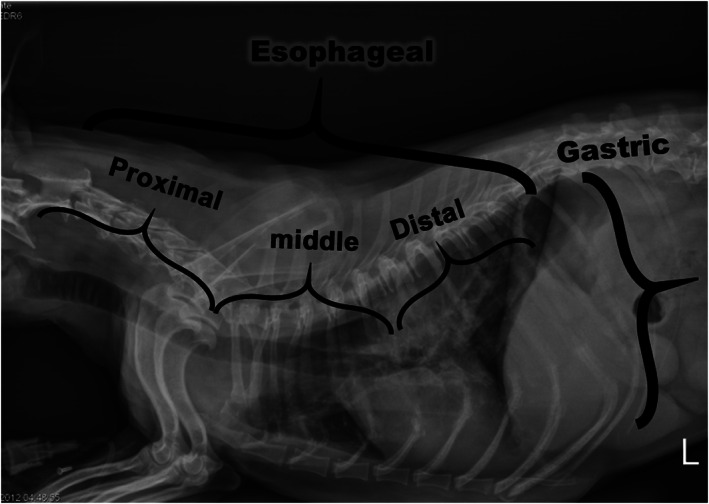
Bone foreign bodies were categorized by location as esophageal or gastric. Esophageal location was further subcategorized into proximal (oropharynx to the thoracic inlet), middle (between the thoracic inlet and the carina), and distal (between the carina and the lower esophageal sphincter)
The outcome of each bone foreign body was recorded as a decision to anesthetize for a procedure (yes/no), successful removal (orally via endoscopic retrieval or via surgery), or digestion (advancement aborad into the stomach via endoscopy or passive movement into the stomach under anesthesia without endoscopic assistance). The endoscopy reports were evaluated for the presence of mucosal erosions (a required field in these reports), whether the dog experienced complications, and whether surgery was indicated. If the dog was not anesthetized for a procedure, follow‐up radiographs, if available, were assessed for time to resolution of the foreign body, and medications dispensed were recorded. In all cases, communication logs and medical records were evaluated to determine clinical signs attributed to the foreign bodies at presentation, complications associated with foreign body management, and, if deceased, whether cause of death was related to the foreign body or not. Additional follow‐up information was retrieved by reviewing NC State‐VH electronic medical records and by telephone interviews with primary care veterinarians. Records from primary care veterinarians were classified as either complete (full record available), partial (incomplete record available, but with sufficient information to determine if the dog died or had adverse sequelae related to bone foreign body ingestion within 2 months after discharge from NC State‐VH), or absent.
2.3. Statistical methods
Body weight, age, and B : BWI were not normally distributed; therefore, groups (E‐bFB and G‐bFB) were compared with a Mann‐Whitney U‐test (GraphPad Prism, version 8.3.0, GraphPad Software Inc, San Diego, California). A P‐value <.05 was considered significant.
A multivariable logistic regression model was constructed in R 3.5.1 11 to examine 2 outcomes: first, whether dogs with esophageal foreign bodies had esophageal mucosal erosions found on endoscopy, and second, whether dogs with gastric foreign bodies underwent endoscopy. We evaluated whether these outcomes were associated with selected explanatory variables. Explanatory variables for the esophageal erosion outcome included age (in years), duration of foreign body (peracute, acute, or chronic), B : BWI, location of the foreign body (proximal, middle, or distal esophageal), and whether the bone was chicken or not (chicken, other animal, or unknown). Explanatory variables for the gastric endoscopy outcome included age, duration of foreign body, B : BWI, presence of clinical signs, bone number (1 bone, 2 bones, >2 bones/bony fragments, or heterogeneous bony material), and whether the bone was chicken or not. All explanatory variables were included in the initial model for each outcome, and the final multivariable model was then selected based on a forward/backward stepwise approach based on Akaike Information Criterion (AIC) using the “MASS” package, 12 eliminating variables that did not contribute significantly to the model. The B : BWI variable was log transformed. Odds ratios (ORs) and 95% confidence intervals (CIs) for the ORs were estimated for each final model. Goodness of fit was assessed with McFadden's pseudo‐R, 2 using the “pscl” package, 13 and by examining graphics of actual outcome versus model predicted outcome. 14
3. RESULTS
3.1. Cases
Two hundred and fourteen potential cases of bone foreign bodies were identified, of which 129 met inclusion criteria. A total of 85 cases were excluded, including 46 in which the terms “bone” and “foreign” in the radiology report were subsequently found to describe 2 different objects. Twenty cases were excluded because of presence of intestinal bone foreign material, rather than gastric or esophageal. Fifteen cases were associated with artificial bone‐like substances and therefore excluded. Three cases were excluded because of resolution by induction of emesis, and 1 was excluded because of localization within the trachea. Medical records from primary care veterinarians were complete for 70 of the 129 included dogs (23 E‐bFBs, 47 G‐bFBs). Nineteen dogs (3 E‐bFBs, 16 G‐bFBs) had partial records with sufficient information to determine if the dog died or had adverse sequelae related to bone foreign body ingestion within the 2 months after presentation to NC State‐VH.
Forty‐five dogs with E‐bFBs were identified, with 20 breeds represented in this group, and weights ranging from 0.8 kg to 52.0 kg. The most common breeds were Shih Tzu (n = 5), West Highland White Terrier (n = 5), Chihuahua (n = 5), Jack Russell Terrier (n = 4), Yorkshire Terrier (n = 4), and Pomeranian (n = 3). Bone : body weight index could not be calculated for 6 of the 45 dogs with E‐bFBs. Eighty‐four dogs with G‐bFBs were identified, with 36 breeds represented in this group, and weights ranging from 1.9 kg to 60.9 kg. The most common breeds were mixed breed (n = 11), Labrador Retriever (n = 9), Dachshund (n = 6), Shih Tzu (n = 4), Beagle (n = 4), French Bulldog (n = 4), Maltese Terrier (n = 3), Bassett Hound (n = 3), and Corgi (n = 3). Bone : body weight index could not be calculated for 13 of the 84 dogs with G‐bFBs.
Dogs with E‐bFBs weighed significantly less than dogs with G‐bFBs (median weight E‐bFB, 7 kg [interquartile range (IQR), 3.48‐9.28]; median weight G‐bFB, 18.6 kg [IQR 9.25‐26.35]; P < .001) and were significantly younger (median age E‐bFB, 4 years [IQR 2‐8]; median age G‐bFB, 6 years [IQR 3‐10]; P = .03). There was no difference between the calculated cross‐sectional areas of gastric and esophageal foreign bodies (median cross‐sectional area E‐bFB, 471 mm2 [IQR 293‐913]; median cross‐sectional area G‐bFB, 557 mm2 [IQR 274‐1081]; P = .72); however, B : BWI was significantly higher in dogs with bone esophageal foreign bodies compared to dogs with bone gastric foreign bodies (median B : BWI E‐bFB, 98.21 mm2/kg [IQR 48.25‐142.6]; median B : BWI G‐bFB, 28.6 mm2/kg [IQR 17.25‐64.28]; P < .001). Dogs with bones entrapped in the middle or distal esophagus had a significantly higher B:BWI than those dogs with proximally‐entrapped bone foreign bodies (median B:BWI proximal, 30.49 mm2/kg [IQR 5.77‐121.3]; middle, 107.5 mm2/kg [IQR 60.55‐232.7]; distal, 105.6 mm2/kg [IQR 71.75‐139.9]; P = .03).
3.2. Esophageal bone foreign bodies
Of 45 dogs with E‐bFBs, 40 had clinical signs at presentation. The primary clinical signs reported were gagging (11), vomiting (8), regurgitation (5), inappetence (3), retching (3), respiratory distress (3), coughing (2), hard swallowing (2), ptyalism (2), and reverse sneezing (1). The remaining 5 dogs were presented after bone ingestion was witnessed, before the development of clinical signs. Eleven dogs were presented peracutely, 16 were presented acutely, and 18 were considered chronically affected. No dogs were found to have incidental esophageal foreign bodies. A single bone was present in all cases, and the location of the E‐bFB was proximal esophageal in 10 dogs, middle esophageal in 10 dogs, and distal esophageal in 25 dogs. Of ingested bones, 11 were of chicken origin, 26 were of non‐chicken origin (beef, turkey, etc.), and 8 were of unknown origin.
All 45 dogs with E‐bFBs (100%) were anesthetized for endoscopic removal. Forty‐two E‐bFBs were successfully addressed non‐surgically, and 3 were removed by surgical esophagotomy after failed endoscopic retrieval. All surgeries were performed at NC State‐VH by board‐certified surgeons and surgical residents, and no dogs underwent surgery without initial attempted endoscopic retrieval. In 33 cases, the bone was grasped under endoscopic guidance and removed from the esophagus per os. In 9 of 45 cases, the esophageal bone was advanced aborad into the stomach; 6 through active advancement and 3 by passive movement in which the bone moved spontaneously into the stomach after induction of anesthesia. Active advancement into the stomach under endoscopic guidance was accomplished by pushing the bone using grasping forceps that protruded a short distance from the tip of the endoscope.
Adverse outcomes were reported in 8 of the 26 dogs with E‐bFBs for which follow‐up information was available, including 2 recorded euthanasias. Of E‐bFBs managed with esophagoscopy alone, 2 dogs developed esophageal strictures, 1 of which resulted in euthanasia. An additional 4 dogs developed clinical problems that could not be definitively associated with the E‐bFB or its endoscopic removal. These problems included an uncharacterized infection, “not doing well” 10 days after the procedure, a “sensitive stomach,” and presentation to an emergency hospital for coughing or gagging 3 months after the procedure. Of the 3 dogs with E‐bFBs that underwent surgical esophagotomy after failed attempts at endoscopic removal, 1 dog had no short‐term complications and was lost to follow‐up, 1 dog developed an esophageal stricture postoperatively and was subsequently managed with a gastrostomy tube, and 1 dog was euthanized after developing pyothorax. A gastrostomy tube was also placed in the latter dog. A gastrostomy tube was not placed in any dogs in which the bone was resolved non‐surgically. Of the 9 dogs in which the bone was advanced into the stomach, in 2 cases the bone was grasped and removed endoscopically from the gastric lumen during the initial endoscopy procedure, 1 dog underwent surgical gastrotomy and bone removal by the primary care veterinarian the day after the endoscopy procedure, and the remaining 6 had bones left for in situ digestion without reported complications. In an additional 2 dogs in which E‐bFBs were successfully resolved endoscopically, smaller fragments of bone were left in the stomach to digest, with no known complications.
Twenty‐eight of 45 dogs (62%; 95% CI 47‐76) with E‐bFBs had esophageal mucosal erosions noted during endoscopy. Erosions were present in 21 of the 33 cases (64%; 95% CI 45‐80) in which the bone was removed endoscopically per os, in 4 of the 6 (67%; 95% CI 22‐96) cases in which the bone was advanced into the stomach, and in none of the cases in which the bone moved passively into the stomach with induction of anesthesia. Erosions were present in all 3 dogs undergoing surgical removal of E‐bFBs and in both dogs that developed esophageal strictures after endoscopic E‐bFB removal.
There were more erosions associated with increased chronicity, with erosions present in 3 of 11 peracute cases, 9 of 16 acute cases, and 16 of 18 chronically affected cases (Figure 2A). More erosions were associated with more distal entrapment, with erosions present in 3 of 10 cases with proximal entrapment, 5 of 10 cases with middle entrapment, and 20 of 25 cases with distally entrapped E‐bFBs (Figure 2B). There was no significant difference in the B : BWI between dogs with and without mucosal erosions. Based on the multivariable logistic regression model, only chronicity and location of entrapment were independently associated with mucosal erosions. Dogs with chronic esophageal foreign bodies were significantly more likely to experience mucosal erosions (OR 18.82 [95% CI 2.22‐273.97], P = .01) compared to dogs with peracute entrapments. Distally entrapped bone foreign bodies were also significantly associated with erosions (OR 12.88, [95% CI 31.95‐129.29], P = .01). Age, B:BWI, and chicken origin were not associated with mucosal erosions.
FIGURE 2.
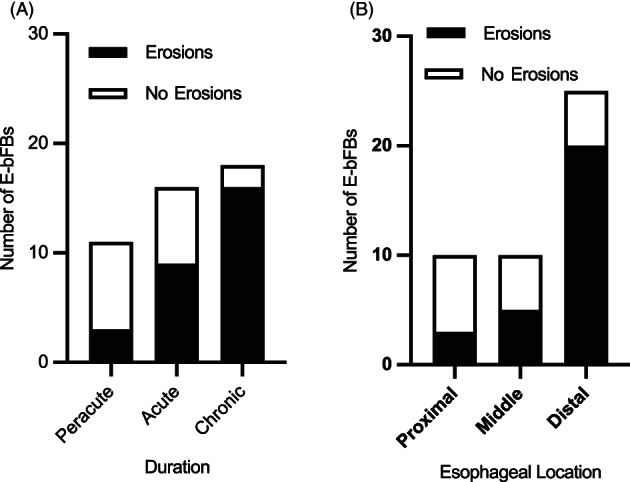
(A) Duration (time from ingestion to presentation) of esophageal bone foreign bodies in 45 dogs, with stacked bars representing number of dogs with and without esophageal erosions, for each duration. (B) Esophageal location of bone foreign bodies in 45 dogs, with stacked bars representing number of dogs with and without esophageal erosions, for each location. E‐bFB, esophageal bone foreign body
3.3. Gastric bone foreign bodies
Of 84 dogs with G‐bFBs, 24 had clinical signs at the time of presentation, with 20 of 24 (83%; 95% CI 62‐95) experiencing vomiting as their predominant clinical sign. Diarrhea, anorexia, hypersalivation, or abdominal distension was also reported. Twenty‐six dogs were presented peracutely, 14 were presented acutely, and 2 were considered chronic. Thirty‐eight dogs were found to have incidental gastric bone foreign bodies, and 4 had an unknown duration of ingestion. Twenty‐three dogs had ingested a single bone, and 8 dogs had ingested 2 bones or a single bone split into 2 fragments. Gastric contents of 40 dogs showed 3 or more bony fragments, and 13 dogs had gastric contents consistent with heterogenous bony material. Of ingested bones, 16 were of chicken origin, 22 were of known non‐chicken origin (beef, turkey, etc.), and 46 were of unknown origin.
Sixty‐two of the 84 dogs with G‐bFBs (74%) did not undergo interventional (surgical or endoscopic) procedures, and the bones were left in situ to undergo gastric digestion. The median age of these dogs was 8 years (IQR 5.0‐11.0), and 9 of these dogs had clinical signs at the time of presentation. Three of the 62 dogs were euthanized at or around the time of diagnosis because of unrelated illness, and 1 died during anesthesia for an unrelated procedure. Of the 62 dogs that did not undergo interventional procedures, specific medications were prescribed in 13 dogs, some of which received multiple medications: omeprazole (5), famotidine (5), sucralfate (4), maropitant citrate (3), ondansetron (1), and metronidazole (1). In addition, short‐term dietary management, including a high fiber prescription diet, a highly digestible diet, or addition of white bread, was recommended in 4 dogs. Follow‐up abdominal imaging was recommended for 10 dogs and performed in 7. In 2 dogs, the G‐bFB resolved within 1 day; in 2 dogs, the bones were resolved by the time of subsequent imaging at 14 or 18 days, and in 3 dogs, the bones were reduced in size within 1 day, with no further imaging reported.
Endoscopic removal of the G‐bFB was attempted in 22 dogs (26%) and was successful in 20 of the 22 (91%; 95% CI 70‐99) dogs. The median age of these 22 dogs was 3 years (IQR 1.0‐5.25), and 15 of these dogs had clinical signs at the time of presentation. No complications of removal were reported. Of the 2 G‐bFBs for which endoscopic removal was unsuccessful, 1 was left to undergo gastric digestion with no reported complications (the dog died 6 years later from cardiac disease), and 1 was referred to the primary care veterinarian for surgical removal, and subsequently lost to follow‐up. There was no difference in B:BWI index between dogs that did and did not show clinical signs associated with the G‐bFB (B:BWI not clinical, 27.15 [IQR 16.41‐77.45]; B : BWI clinical, 31.97 [IQR 18.14‐46.10]; P = .78; Figure 3A), but B : BWI was significantly higher in dogs that underwent endoscopy compared to dogs in which bone removal was not attempted (B:BWI no endoscopy, 24.46 [IQR 14.82‐44.49]; B : BWI endoscopy, 50.65 [IQR 32.73‐95.73]; P < .001; Figure 3B).
FIGURE 3.
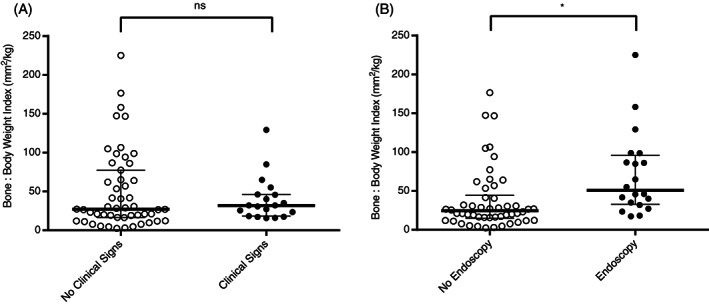
(A) Dot plots of bone : body weight index (B : BWI) in dogs that did or did not have clinical signs associated with G‐bFBs. ns, no significant difference. (B) Dot plots of B : BWI in dogs that did or did not undergo endoscopy for G‐bFB retrieval. *P < .001. The wider and thicker bars represent the median, and smaller bars above and below the median represent the interquartile range
In the multivariable model, 3 variables remained in the reduced model (clinical signs, B : BWI, and age), indicating that these factors significantly independently affected the odds of endoscopy being attempted. The number of bones or bone fragments was also included in the reduced model because of the potential for this variable being confounding, but this variable was not significantly associated with the decision to attempt endoscopic removal. Endoscopic removal was more likely to be attempted in dogs with clinical signs (OR 92.1 [95% CI 9.84‐2724], P = .001) and dogs with bones that had larger B:BWI (OR 9.4 [95% CI 2.05‐78.0], P = .01). Endoscopy was less likely in older dogs, with each year of age associated with 0.76 lower odds of endoscopy (OR 0.77 [95% CI 0.569‐0.96], P = .04). Duration of foreign body, bone number or fragmentation, or source of the bony material (chicken or other) was not associated with the decision to pursue endoscopy.
Complete medical records were available for 47 of 84 dogs with G‐bFBs, with partial records available for an additional 16 dogs. In total, follow‐up information was available for 63 (75%) of 84 dogs, including 14 dogs that underwent endoscopy, and 49 dogs in which G‐bFBs were left in situ to undergo digestion. One dog had equivocal signs reported by the primary care veterinarian (“tense abdomen”), but the remaining 62 had no reported clinical signs. No dogs for which follow‐up was available were determined to have died from short‐term complications or chronic disease related to a gastric bone foreign body (G‐bFB).
4. DISCUSSION
In this retrospective study of esophageal and gastric bone foreign bodies in dogs, we found that endoscopic removal of E‐bFBs was attempted in all cases, with a high success rate overall. In contrast, the majority of dogs with gastric bone foreign bodies did not undergo interventional procedures, and when the bones were left in situ to digest, there was no evidence of short‐term or long‐term adverse effects in those dogs for which follow‐up information was available.
Bones are a commonly encountered gastrointestinal foreign body in dogs, but present a clinical conundrum, with conflicting arguments regarding the necessity of their removal: they have the potential to digest in the stomach with no harm to the dog, or could cause perforation with significant morbidity and risk of mortality. The urgency of bone foreign body removal is dependent on their location within the gastrointestinal tract. Esophageal foreign bodies warrant urgent or emergency removal, whereas guidelines for management of G‐bFBs in dogs are less clear.
Esophageal bone foreign bodies were resolved non‐surgically in 42 of 45 dogs in this study, and endoscopy was always attempted before surgery was performed. In 6 dogs, the bone was pushed into the stomach, after unsuccessful attempts to remove per os. This was accomplished by pushing the E‐bFB with grasping forceps that protruded a short distance from the end of the endoscope biopsy channel. There did not appear to be any correlation between presence of erosions and ability to remove the E‐bFB per os, as erosions were present in a similar proportion of dogs that either had the E‐bFB removed per os, or advanced into the stomach. In 3 dogs with E‐bFBs in this study, when endoscopy was performed, the bone had already moved into the stomach. It is presumed that this happened with the muscle relaxation that occurred at the time of anesthetic induction, as esophageal location of the bones was confirmed radiographically before endoscopy was performed. None of these dogs had esophageal erosions present, suggesting that the bones were not firmly lodged in the esophagus, and therefore were more likely to move spontaneously. When E‐bFBs were advanced into the stomach, either actively or spontaneously, in 2 dogs they were removed per os during the endoscopic procedure, and in 1 dog the bone was removed by gastrotomy after discharge from the referral hospital. The reasons for these decisions cannot be determined in this retrospective study, but the most important finding is that for those dogs in which the E‐bFB was left in the stomach for digestion, no adverse effects were reported. Advancement of an esophageal foreign body into the stomach has been reported in other studies, 5 , 6 but it is difficult to compare our findings with those studies as they included other types of foreign bodies in addition to bones, and outcomes were not consistently reported.
When dogs with E‐bFBs were compared to dogs with G‐bFB in our study, dogs with E‐bFBs were younger, of smaller body weight, and had a higher B : BWI compared to dogs with G‐bFBs. Five of 45 dogs with E‐bFBs were West Highland White Terriers. A breed predilection for esophageal foreign bodies in West Highland White Terriers has been previously reported, but no explanation has been provided. 1 , 4 , 7 , 15 Other small breeds represented in higher numbers included 5 each of Shih Tzu and Chihuahua; however, it is not possible to state that any of these breeds are truly overrepresented among dogs with E‐bFBs as their prevalence in our hospital population was not assessed.
Our findings in dogs with E‐bFBs align with other large studies of esophageal foreign bodies in dogs, 1 , 4 , 5 , 6 , 16 with endoscopic removal being successful in most cases. Previously described risk factors for complications associated with esophageal foreign bodies include smaller body size, 1 older age, 3 and entrapment or clinical signs for multiple days 2 , 3 , 7 ; although in a different study, procedural complications, but not prolonged esophageal entrapment, were associated with increased risk of death. 4 The degree of esophagitis, as characterized by the amount of mucosal hyperemia and erosions, has been associated with duration and severity of clinical signs at presentation, longer length of hospitalization, and increased risk of complications, 6 although the severity of esophagitis does not negatively predict successful endoscopic retrieval. 15 Using a multivariable model, we found that duration and site of entrapment were the only significant predictors of erosion formation, with entrapment >2 days and location within the distal esophagus carrying the highest risk. Dog age, B : BWI, and type of bone were not associated with development of erosions.
Gastric feeding tubes were placed in only 2 dogs with E‐bFBs in our study, both of which underwent esophagotomy. Gastrostomy tubes were not placed in any dogs in which E‐bFBs were managed non‐surgically. This is in contrast to 1 study in which gastric feeding tubes were placed in 21 of 60 dogs with esophageal foreign bodies, the majority of which were resolved non‐surgically, 6 and another study in which feeding tubes were placed in 16 of 114 dogs with esophageal foreign bodies, the majority of which were also managed non‐surgically. 16 In the former study, feeding tubes were only placed in dogs with moderate‐to‐severe esophagitis, but the reasons for this decision were not discussed. 6 In the latter study, severity of esophagitis and duration of foreign body were both statistically significantly associated with feeding tube placement, and the decision was attributed to clinician discretion. 16 No studies have compared the risks and benefits of feeding tube placement after resolution of esophageal foreign bodies, but it is not a standard procedure in our hospital, in which oral feeding is recommended after full recovery from anesthesia. This reflects institutional preference and a lack of evidence that “resting” the esophagus is beneficial. There are currently little data upon which to base either recommendation.
When gastric foreign body removal is indicated, this can be attempted through induction of emesis, 17 endoscopy, or surgery. Bone foreign bodies resolved by emesis were not included in this study, and while induction of emesis, for example with apomorphine, might be a valuable approach for soft materials such as socks or tampons, it is less appropriate for resolution of sharp objects, 17 and is not a common approach with bone foreign bodies. 18 Considerations regarding management of G‐bFBs also differ from other foreign bodies because bones are potentially digestible, compared to other materials ingested by dogs, such as fabric, plastic, and rocks. 17 Although members of the order Carnivora, dogs are omnivorous; their wild relatives consume both prey and carrion, 19 and would be expected to ingest and digest bones. Therefore, another approach to the management of G‐bFBs is to leave them in situ for digestion. 20 We found no clear adverse outcomes associated with gastric digestion of bones, or with gastric advancement and digestion of bones initially entrapped in the esophagus. In this tertiary referral center, where both endoscopic and surgical management are available, no gastrotomies for bone foreign body removal were performed, but esophagotomy was performed in 3 cases in which endoscopic removal of esophageal foreign bodies failed. Although 74% of gastric bones were left in situ for digestion, endoscopic removal was attempted for 26% of identified gastric bones. The presence of clinical signs was the most significant factor in the decision to attempt removal of a gastric bone, with an OR greater than 90. However, younger age and a larger bone to body size ratio (B:BWI) were also independently associated with the decision to remove the bone. Potential explanations for the association with young age could include owner reluctance to consent to anesthesia in an older dog, owner prior experience with bone ingestion that resolved without attempted removal, or the presence of comorbidities in an older dog. The association between B : BWI and decision to remove the bone could reflect clinician concern that larger amounts of bony material might not safely resolve without intervention. However, the relative roles of owner and clinician factors in decisions regarding G‐bFB management cannot be determined from this study.
Our study has limitations, most notably the retrospective nature, relatively low frequency of complete information from primary care veterinarians for follow‐up, and the small number of cases with reported complications. The influence of other characteristics of the bone, such as sharpness or whether the bone had been cooked, was not investigated. Future studies could investigate the potential for gastric dissolution of bones in study animals, and more specifically characterize the effects of bone density, bone sharpness, and gastric pH modulation on gastric dissolution of bone foreign bodies. Although study numbers were too small to compare outcomes, it may be worth noting that even dogs with G‐bFBs that were prescribed antacids had no chronic signs or complications. Lastly, this study was performed at a tertiary referral clinic. It is possible that in primary care practices, surgical (rather than endoscopic) management of gastric foreign bodies would be elected, and the proportion of cases of gastric bones left to digest might differ from the referral population.
In summary, while all E‐bFBs were dislodged either by advancement into the stomach, endoscopic removal, or esophagotomy, the majority of G‐bFBs were left in situ for dissolution with no reported complications. When removal of G‐bFBs was attempted, endoscopy was performed in all cases, and the presence of clinical signs was strongly associated with the decision to attempt removal. Younger age and larger relative total bone size were also associated with the decision to remove a G‐bFB. Although upper gastrointestinal bone foreign bodies have been associated with increased complications compared to non‐bone foreign bodies, 1 we found a relatively low complication rate (8/45 esophageal, and 0/84 gastric). Gastric advancement of E‐bFBs should be considered in cases where oral removal is not feasible, and gastric dissolution can be considered even with large bones.
CONFLICT OF INTEREST DECLARATION
Authors declare no conflict of interest.
OFF‐LABEL ANTIMICROBIAL DECLARATION
Authors declare no off‐label use of antimicrobials.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC) OR OTHER APPROVAL DECLARATION
Authors declare no IACUC or other approval was needed.
HUMAN ETHICS APPROVAL DECLARATION
Authors declare human ethics approval was not needed for this study.
ACKNOWLEDGMENT
No funding was received for this study.
Barash NR, Lashnits E, Kern ZT, Tolbert MK, Lunn KF. Outcomes of esophageal and gastric bone foreign bodies in dogs. J Vet Intern Med. 2022;36(2):500‐507. doi: 10.1111/jvim.16383
REFERENCES
- 1. Gianella P, Pfammatter NS, Burgener IA. Oesophageal and gastric endoscopic foreign body removal: complications and follow‐up of 102 dogs. J Small Anim Pract. 2009;50:649‐654. [DOI] [PubMed] [Google Scholar]
- 2. Thompson HC, Cortes Y, Gannon K, Bailey D, Freer S. Esophageal foreign bodies in dogs: 34 cases (2004‐2009). J Vet Emerg Crit Care. 2012;22:253‐261. [DOI] [PubMed] [Google Scholar]
- 3. Brisson BA, Wainberg SH, Malek S, Reabel S, Defarges A, Sears WC. Risk factors and prognostic indicators for surgical outcome of dogs with esophageal foreign body obstructions. J Am Vet Med Assoc. 2018;252:301‐308. [DOI] [PubMed] [Google Scholar]
- 4. Burton AG, Talbot CT, Kent MS. Risk factors for death in dogs treated for esophageal foreign body obstruction: a retrospective cohort study of 222 cases (1998‐2017). J Vet Intern Med. 2017;31:1686‐1690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Wyatt SR, Barron PM. Complications following removal of oesophageal foreign bodies: a retrospective review of 349 cases. Aust Vet J. 2019;97:116‐121. [DOI] [PubMed] [Google Scholar]
- 6. Rousseau A, Prittie J, Broussard JD, Fox PR, Hoskinson J. Incidence and characterization of esophagitis following esophageal foreign body removal in dogs: 60 cases (1999‐2003). J Vet Emerg Crit Care. 2007;17:159‐163. [Google Scholar]
- 7. Sterman AA, Mankin KMT, Ham KM, Cook AK. Likelihood and outcome of esophageal perforation secondary to esophageal foreign body in dogs. J Am Vet Med Assoc. 2018;253:1053‐1056. [DOI] [PubMed] [Google Scholar]
- 8. Hayes G. Gastrointestinal foreign bodies in dogs and cats: a retrospective study of 208 cases. J Small Anim Pract. 2009;50:576‐583. [DOI] [PubMed] [Google Scholar]
- 9. Tams TR. Diseases of the esophagus. In: Tams TR, ed. Handbook of Small Animal Gastroenterology. 2nd ed. St. Louis, MO: Saunders; 2003:118‐158. [Google Scholar]
- 10. Aronson LR, Brockman DJ, Brown DC. Gastrointestinal emergencies. Vet Clin North Am Small Anim Pract. 2000;30:555‐579. [DOI] [PubMed] [Google Scholar]
- 11. R Core Team . R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2018. https://www.R-project.org/ [Google Scholar]
- 12. Venables WN, Ripley BD, Venables WN. Modern Applied Statistics with S. 4th ed. New York: Springer; 2002. https://www.stats.ox.ac.uk/pub/MASS4/ [Google Scholar]
- 13. Jackman S. pscl: Classes and Methods for R Developed in the Political Science Computational Laboratory. Sydney, Australia: United States Studies Centre, University of Sydney; 2017. R package version 1.5.2 https://github.com/atahk/pscl/ [Google Scholar]
- 14. McFadden D. Quantitative methods for Analysing travel behaviour of individuals: some recent developments. In: Hensher DA, Stopher PR, eds. Behavioural Travel Modelling. London, England: Croom Helm; 1979:279‐318. [Google Scholar]
- 15. Juvet F, Pinilla M, Shiel RE, Mooney CT. Oesophageal foreign bodies in dogs: factors affecting success of endoscopic retrieval. Ir Vet J. 2010;63:163‐168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bongard AB, Furrow E, Granick JL. Retrospective evaluation of factors associated with degree of esophagitis, treatment, and outcomes in dogs presenting with esophageal foreign bodies (2004‐2014): 114 cases. J Vet Emerg Crit Care. 2019;29:528‐534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Zersen KM, Peterson N, Bergman PJ. Retrospective evaluation of the induction of emesis with apomorphine as treatment for gastric foreign bodies in dogs (2010‐2014): 61 cases. J Vet Emerg Crit Care. 2020;30:209‐212. [DOI] [PubMed] [Google Scholar]
- 18. Kirchofer KS, Block G, Johnson JA. Efficacy of intravenous administration of apomorphine for removal of gastric foreign material in dogs: 495 cases (2010‐2015). J Am Vet Med Assoc. 2019;255:459‐465. [DOI] [PubMed] [Google Scholar]
- 19. Debraekeleer J, Gross KL, Zicker SC. Normal dogs. In: Hand MS, Thatcher CD, Remillard RL, eds. Roudebush P: Small Animal Clinical Nutrition. 4th ed. Topeka, KS: Mark Morris Institute; 2000:213‐260. [Google Scholar]
- 20. Guilford WG. Gastrointestinal endoscopy. In: Guilford WG, Center SA, Strombeck DR, Williams DA, Meyer DJ, eds. Strombeck's Small Animal Gastroenterology. 3rd ed. Philadelphia, PA: WB Saunders; 1996:114‐129. [Google Scholar]