

Abstract
Background
Quadriceps strength and mass deficits are common after anterior cruciate ligament (ACL) reconstruction. Postoperatively, heavy load resistance training can have detrimental effects on knee joint pain and ACL graft laxity. Therefore, low-load blood flow restriction (LL-BFR) training has been suggested as an alternative to traditional strength rehabilitation.
Purpose
The present systematic review aimed to investigate the effect of LL-BFR training on quadriceps strength, quadriceps mass, knee joint pain, and ACL graft laxity after ACL reconstruction compared to non-BFR training.
Study design
Systematic review
Methods
A systematic literature search of PubMed, EMBASE.com, Cochrane Library/Wiley, CINAHL/Ebsco and Web of Science/Clarivate Analytics was performed on 19 February 2021. Studies were included if they compared LL-BFR and non-BFR training after ACL reconstruction with pre- and post-intervention quadriceps strength, quadriceps mass, knee joint pain or ACL graft laxity measurement. Systematic reviews, editorials, case reports and studies not published in a scientific peer reviewed journal were excluded. The risk of bias of randomized studies was assessed with the use of the Cochrane Risk of Bias Tool.
Results
A total of six randomized controlled trials were included. Random sequence generation and allocation concealment was defined as high risk in two of the six studies. In all studies blinding of participants and personnel was unclear or could not be performed. The included studies used different LL-BFR and non-BFR protocols with heterogeneous outcome measurements. Therefore, a qualitative analysis was performed. Two of the six studies assessed quadriceps strength and demonstrated significant greater quadriceps strength after LL-BFR compared to non-BFR training. Quadriceps mass was evaluated in four studies. Two studies observed significant greater quadriceps mass after LL-BFR compared to non-BFR training, while two studies observed no significant difference in quadriceps mass. Knee joint pain was assessed in three studies with significantly less knee joint pain after LL-BFR compared to non-BFR training. Two studies evaluated ACL graft laxity and observed no significant difference in ACL graft laxity between LL-BFR and non-BFR training.
Conclusion
The results of this systematic review indicate that LL-BFR training after ACL reconstruction may be beneficial on quadriceps strength, quadriceps mass, and knee joint pain compared to non-BFR training with non-detrimental effects on ACL graft laxity. However, more randomized controlled trials with standardized intervention protocols and outcome measurements are needed to add evidence on the clinical value of LL-BFR training.
Level of evidence
2a
Keywords: resistance training, quadriceps strength, quadriceps mass, postoperative rehabilitation, knee pain, graft laxity
INTRODUCTION
Quadriceps strength and mass deficits are common after anterior cruciate ligament (ACL) reconstruction.1–6 Approximately 30% of patients have quadriceps strength deficits 12 months after ACL surgery.1,3 Quadriceps mass deficits can be as high as 30% and can persist for many years after ACL reconstruction.5 Furthermore, quadriceps mass deficits can negatively affect quadriceps strength.7–9 This is of importance as quadriceps strength after ACL reconstruction is associated with patient reported outcome measurements, functional performance, return to sport and ACL re-injury.1,10–16 Therefore, interventions to address quadriceps strength and mass deficits after ACL reconstruction are imperative.
Heavy load resistance (HLR) training using external loads >60% of one repetition maximum (1RM) is recommended to increase quadriceps strength and mass.17 However, after ACL reconstruction, training with external loads >60% 1RM can have detrimental effects on knee joint pain and ACL graft laxity.18–23 Therefore, low-load blood flow restriction (LL-BFR) training using external loads of 20-40% 1RM has been suggested as an alternative to traditional strength rehabilitation.24,25 During LL-BFR training, a pressurized cuff is applied to the proximal thigh that occludes venous outflow while maintaining arterial inflow.24,25 The combination of venous occlusion and resistance training is believed to induce muscle hypertrophy secondary to elevated systematic hormone production, cell swelling, production of reactive oxygen species, intramuscular anabolic signaling and fast-twitch fiber recruitment.25–27
A recent systematic review showed promising results of LL-BFR training on quadriceps mass after ACL reconstruction.28 As LL-BFR training is an increasingly popular method for the rehabilitation after an ACL reconstruction, it is important to evaluate the value of this treatment.24,25 Therefore, the present systematic review aimed to investigate the effect of LL-BFR training on quadriceps strength, quadriceps mass, knee joint pain and ACL graft laxity after ACL reconstruction compared to non-BFR training.
MATERIALS AND METHODS
The review protocol was registered on PROSPERO (CRD42020163467) and was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines.29
Search strategy and study selection
A systematic literature search in PubMed, EMBASE.com, Cochrane Library/Wiley, CINAHL/Ebsco and Web of Science/Clarivate Analytics was performed on 19 February 2021 (BK, MH). The following search terms, including all synonyms, were used to search in all databases as index term and as free-text words: blood flow restriction and anterior cruciate ligament (See Appendix 1 for the detailed search strategy). The results of the literature search were collected in the reference management program RefWorks and were de-duplicated.30 Studies were included if they compared LL-BFR and non-BFR training after ACL reconstruction with pre- and post-intervention quadriceps strength or quadriceps mass or knee joint pain or ACL graft laxity measurement. Non-BFR training was defined as strength training without vascular restriction. The exclusion criteria were: systematic reviews, editorials, case reports and studies not published in a scientific, peer reviewed journal. Two reviewers (BK and AT) separately and independently screened all titles and abstracts. The full text was reviewed if title and abstract suggested a study of interest. In case of disagreement, consensus was achieved by a third researcher (MS). In addition, trial reference lists of included studies were screened for relevant articles.
Data extraction
Data of included articles were extracted with the use of RevMan 5.4 (Review Manager 5.4, The Cochrane Centre Collaboration, Copenhagen, Denmark, 2020) including: year of publication, study design, number of patients, study arms, graft used for ACL reconstruction, patient characteristics, LL-BFR training protocol, non-BFR training protocol, and quadriceps strength, quadriceps mass, knee joint pain, and ACL graft laxity measurements.31 When raw data of outcome measurements were not available, the authors were contacted to provide raw data.
Study quality and reporting
The independent reviewers (BK and AT) assessed the risk of bias of the included studies with the use of the Cochrane Risk of Bias Tool. Non-randomized studies were assessed with the ROBINS-I checklist.32 The included studies were evaluated on: selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias.
Data synthesis
Outcome measurements were extracted with the use of RevMan 5.4.31 The difference in pre- and post-intervention mean and standard deviation (SD) was used to calculate the standardized mean difference (SMD). In case SD was not available, this was estimated in accordance with recommendations provided by Cochrane Handbook for Systematic Reviews.33 Data were pooled for a meta-analysis if the included studies were clinically, methodologically and statistically homogenous. In case of considerable heterogeneity (I2 >75%) of the study results, a qualitative analysis was performed.34 The level of statistical significance was set at p≤0.05.
RESULTS
Study selection and characteristics
The database search yielded 1474 articles. After initial title and abstract screening, 11 articles were assessed for eligibility. The remaining 11 articles were fully read and six articles met the inclusion criteria. The two independent reviewers agreed on selection of eligible studies and achieved consensus on which studies to include. No additional studies were identified through reference list screening. Therefore, six articles were included in the systematic review (Figure 1). Table 1 shows an overview of the study characteristics.
Figure 1. Flow chart of the literature search and selection procedure.
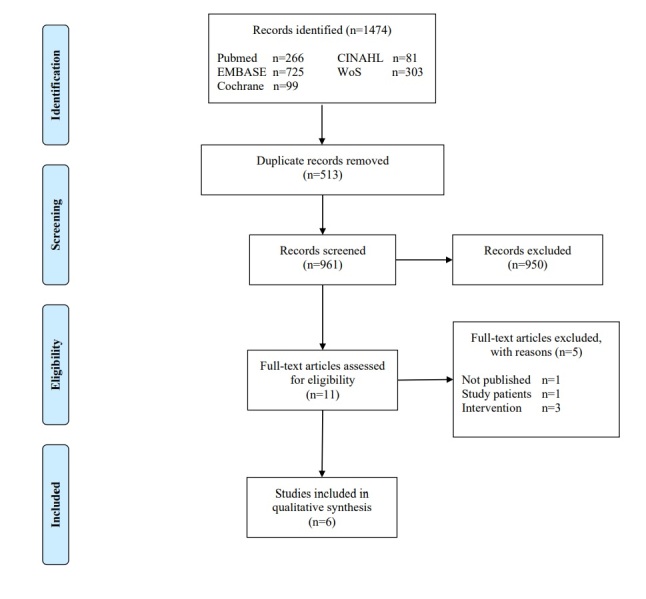
Table 1. Overview of study characteristics.
| Author (Year) | Study design | Total number of patients |
Study arms
(No.) |
Outcome |
|---|---|---|---|---|
| Hughes (2019a) |
Randomized controlled trial | 24 | LL-BFR group (n=12) Non-BFR group (n=12) |
Quadriceps strength Quadriceps mass Knee joint pain ACL graft laxity |
| Hughes (2019b) |
Randomized controlled trial | 24 | LL-BFR group (n=12) Non-BFR group (n=12) |
Knee joint pain |
| Hughes (2018) |
Randomized controlled trial | 20 | LL-BFR group (n=10) Non-BFR group (n=10) |
Knee joint pain |
| Iversen (2014) |
Randomized controlled trial | 24 | LL-BFR group (n=12) Non-BFR group (n=12) |
Quadriceps mass |
| Ohta (2003) |
Randomized controlled trial | 44 | LL-BFR group (n=22) Non-BFR group (n=22) |
Quadriceps strength Quadriceps mass ACL graft laxity |
| Takarada (2000) |
Controlled trial | 16 | LL-BFR group (n=8) Non-BFR group (n=8) |
Quadriceps mass |
LL-BFR: Low-load blood flow restriction.
Three studies were conducted in the United Kingdom, two in Japan and one in Norway.18,35–39 The studies conducted in the United Kingdom are three reports from the same study.18,35,36 However, the three reports from the same study described different outcome measurements, thus, were included in this review. The included studies involved a total of 152 patients who had been randomized into LL-BFR (n=76) or non-BFR (n=76) group.18,35–39 Sample sizes ranged between 16 and 44 patients.18,35–39 Five studies used hamstring graft for ACL reconstruction, whereas one study did not report type of graft.18,35–39 Patient characteristics were not statistically significant different between the LL-BFR and non-BFR group. Table 2 shows an overview of the patient characteristics.
Table 2. Overview of patient characteristics.
| Author (Year) | Graft for ACL reconstruction | Male in LL-BFR & non-BFR group | Age (years) in LL-BFR & non-BFR group | Weight (kg) in LL-BFR & non-BFR group | BMI in LL-BFR & non-BFR group |
|---|---|---|---|---|---|
| Hughes (2019a) |
Hamstring | 7 (58%) & 10 (83%) | 29 (7) & 29 (7) | 76 (15) & 79 (15) | 25.4 (3.9) & 26.4 (4.4) |
| Hughes (2019b) |
Hamstring | 7 (58%) & 10 (83%) | 29 (7) & 29 (7) | 76 (15) & 79 (15) | 25.4 (3.9) & 26.4 (4.4) |
| Hughes (2018) |
Hamstring | 6 (60%) & 7 (70%) | 29 (5) & 31 (7) | 77 (16) & 81 (12) | 25.7 (4.2) & 23.5 (3.4) |
| Iversen (2014) |
Hamstring | 7 (58%) & 7 (58%) | 25 (7) & 30 (9) | 77 (12) & 78 (10) | - |
| Ohta (2003) |
Hamstring | 13 (59%) & 12 (55%) | 28 (10) & 30 (10) | 65 (14) & 63 (9) | - |
| Takarada (2000) |
- | 4 (50%) & 4 (50%) | 22 (1) & 23 (1) | 59 (1) & 62 (2) | - |
Results are presented as numbers (percentage) or mean (SD). ACL: anterior cruciate ligament; BMI: body mass index; LL-BFR: low-load blood flow restriction.
LL-BFR and non-BFR protocols
The intervention protocols are shown in Table 3. The duration of the intervention varied from 11 days up to 14 weeks and training sessions varied from two sessions/week up to two sessions/day.18,35–39 LL-BFR training was used in combination with low-load leg press, leg extension or straight leg raise exercises.18,35–39 The external load varied from body weight up to 30% 1RM and was not specified in two studies.18,35–39 Automatic personalized tourniquet systems and pneumatic cuffs were used during LL-BFR training.18,35–39 The occlusion pressure ranged between 148 and 238 mmHg, while cuff width ranged from 9 to 14 cm.18,35–39 In three studies LL-BFR pressure was defined as 80% of the limb occlusion pressure (ranged from 140 to 160 mmHg), whereas the occlusion pressure was based on previous research in three studies (ranged from 180 to 240mmHg).18,35–39 LL-BFR was intermittently applied with reperfusion periods ranging from 30 to 180 seconds.18,35,36,38,39 In three studies, non-BFR training consisted of the same exercise protocol as LL-BFR training but without vascular restriction.37–39 Hughes et al. used different exercise protocols in the non-BFR and LL-BFR group.18,35,36 In the non-BFR group, the patients performed three sets of 10 repetitions using external loads of 70% 1RM. In the LL-BFR group, the patients performed four sets (30-15-15-15) using external loads of 30% 1RM.18,35,36
Table 3. Overview of intervention.
| Author (Year) | BFR device | Cuff width | BFR pressure | LL-BFR training | Non-BFR training | Exercises | Duration | Total training sessions |
|---|---|---|---|---|---|---|---|---|
| Hughes (2019a) |
Automatic personalized tourniquet system | 11.5 cm | Mean 150 mmHg Based on 80% of LOP |
4 sets (30-15-15-15 reps) Interset rest periods: 30 seconds External load: 30% 1RM Session: 2x/week |
3 sets (10-10-10 reps) Interset rest periods: 30 seconds External load: 70% 1RM Session: 2x/week |
Unilateral leg press | 8 weeks Start: 2 weeks postop End: 10 weeks postop |
16 |
| Hughes (2019b) |
Automatic personalized tourniquet system | 11.5 cm | Mean 150 mmHg Based on 80% of LOP |
4 sets (30-15-15-15 reps) Interset rest periods: 30 seconds External load: 30% 1RM Session: 2x/week |
3 sets (10-10-10 reps) Interset rest periods: 30 seconds External load: 70% 1RM Session: 2x/week |
Unilateral leg press | 8 weeks Start: 2 weeks postop End: 10 weeks postop |
16 |
| Hughes (2018) |
Automatic personalized tourniquet system | 11.5 cm | Mean 148 mmHg Based on 80% of LOP |
4 sets (30-15-15-15 reps) Interset rest periods: 30 seconds External load: 30% 1RM Session: 2x/week |
3 sets (10-10-10 reps) Interset rest periods: 30 seconds External load: 70% 1RM Session: 2x/week |
Unilateral leg press | 8 weeks Start: 2 weeks postop End: 10 weeks postop |
16 |
| Iversen (2014) |
Contoured pneumatic occlusion cuff | 14 cm | Start:130 mmHg End: 180 mmHg Based on previous research |
5 sets of 20 reps Interset rest periods: 3 minutes External load: low Session: 2x/day |
5 sets of 20 reps Interset rest periods: 3 minutes External load: low Session: 2x/day |
Isometric quadriceps contraction progressing to leg extension over a knee-roll and straight leg raise | 12 days Start: 2 days postop End: 14 days postop |
24 |
| Ohta (2003) |
Hand-pumped air tourniquet | - | 180 mmHg Based on previous research |
1-3 sets (20 reps) Interset rest periods: unknown External load: 0-14 kg Session: 6x/week |
1-3 sets (20 reps) Interset rest periods: unknown External load: 0-14 kg Session: 6x/week |
Straight leg raise, hip joint abduction/ adduction, half squat, step up, elastic tube and knee-bending walking exercise | 14 weeks Start: 2 weeks postop End: 16 weeks postop |
84 |
| Takarada (2000) |
Pneumatic occlusion cuff | 9 cm | Start: 180 mmHg End: 238 mmHg Based on previous research |
5 sets Interset rest periods: 3 minutes External load: low Session: 2x/day |
5 sets Interset rest periods: 3 minutes External load: low Session: 2x/day |
Hospital rehabilitation protocol with knee brace immobilization | 11 days Start: 3 days postop End: 14 days postop |
22 |
LL-BFR: low-load blood flow restriction; LOP: limb occlusion pressure; 1RM: one repetition maximum; Postop: postoperatively; Reps: repetitions.
Risk of bias
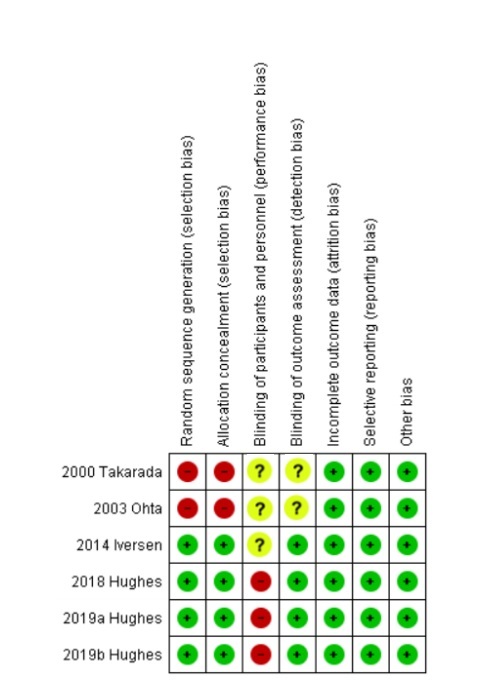
An overview of the quality assessment of the included studies is reported in Figure 2. Random sequence generation and allocation concealment was defined as high risk for bias in two of the six studies. In all studies blinding of participants and personnel was unclear or could not be performed.
Figure 2. Review authors’ judgements about each risk of bias domain with the use of the Cochrane Risk of Bias Tool.
Heterogeneity
Comorbidities and concomitant injuries of study participants were not defined in the included studies. Furthermore, different LL-BFR and non-BFR protocols with heterogeneous outcome measurements were used. Therefore, only a qualitative analysis was performed.
Outcome measurements
Quadriceps strength
Quadriceps strength was evaluated in two studies by measuring RM, isokinetic contraction at 60°/seconds, isokinetic contraction at 150°/seconds, isokinetic contraction at 180°/seconds, isokinetic contraction at 300°/seconds or isometric contraction at 60° knee flexion.35,37 Quadriceps strength was measured pre-operatively and at nine up to 16 weeks postoperatively.35,37 Ohta et al. showed significantly less strength deficits in isokinetic knee extension at 60°/seconds (p<0.001), isokinetic knee extension at 180°/seconds (p=0.004) and isometric contraction at 60° knee flexion (p<0.001) after LL-BFR compared to non-BFR training.37 Hughes et al. reported significantly less strength deficits in isokinetic knee extension at 150° and 300°/seconds after LL-BFR compared to non-BFR training (p=0.010).35 However, no significant differences in RM (p=0.220) and isokinetic knee extension at 60°/seconds (p=0.200) were observed between LL-BFR and non-BFR training.35
Quadriceps mass
Three studies used MRI to measure changes in quadriceps cross-sectional area (CSA), while one study used ultrasound to measure changes in vastus lateralis muscle thickness.35,37–39 Quadriceps mass was measured pre-operatively and 14 days up to 16 weeks postoperatively.35,37–39 Takarada et al. showed significant less reduction in quadriceps CSA after LL-BFR compared to non-BFR training (p=0.046).38 Ohta et. al reported a significant increase in quadriceps CSA after 14 weeks LL-BFR compared to non-BFR training (p=0.040).37 Iversen et al. concluded that there was no significant difference in quadriceps CSA between LL-BFR and non-BFR training (p=0.626).39 Hughes et al. used ultrasound to assess changes in vastus lateralis muscle thickness and demonstrated no significant difference in quadriceps increase between LL-BFR and non-BFR training (p=0.230).35
Knee joint pain
Knee joint pain was assessed using a numerical rating scale in two studies, while one study used the Knee Injury and Osteoarthritis Outcome Score (KOOS) pain score.18,35,36 Knee joint pain was evaluated following each session, 24h post-exercise or 10 weeks postoperatively.18,35,36 Two studies observed significant lower knee joint pain scores in LL-BFR compared to non-BFR training.18,36 Furthermore, one study showed significant greater increase in KOOS pain score after LL-BFR compared to non-BFR training.35
ACL graft laxity
Two studies used a knee ligament arthrometer to measure changes in ACL graft laxity.35,37 ACL graft laxity was measured pre-operatively and at 10 up to 16 weeks postoperatively. No significant difference in ACL graft laxity was observed between LL-BFR and non-BFR.35,37
DISCUSSION
The most important finding of the present systematic review was that low-load blood flow restriction (LL-BFR) training after anterior cruciate ligament (ACL) reconstruction may be beneficial on quadriceps strength and quadriceps mass compared to non-BFR training. Furthermore, LL-BFR training may decrease knee joint pain compared to non-BFR training with similar effects on ACL graft laxity. Thus, the present systematic review suggests that LL-BFR training may be an effective alternative to non-BFR training after an ACL reconstruction.
Regarding quadriceps strength, Ohta et al. showed less quadriceps strength deficits after LL-BFR compared to non-BFR training.37 In addition, Hughes et al. demonstrated similar and greater effects on quadriceps strength after LL-BFR compared to non-BFR training.35 Ohta. at al used low-load resistance training (LLR) training as non-BFR training, while Hughes et al. used heavy-load resistance training (HLR) training as non-BFR training. Therefore, the findings of the present review are consistent with current literature comparing LL-BFR training to LLR and HLR training in healthy and postoperative patients.40–46
In regard to quadriceps mass, two studies demonstrated that LL-BFR training was more beneficial on quadriceps cross-sectional area (CSA) compared to non-BFR training.37,38 In contrast, Iversen et al. observed no difference in quadriceps CSA between LL-BFR and non-BFR training.39 The authors acknowledged that subtherapeutic training (e.g. training duration of 12 days) and LL-BFR application (e.g. no personalized BFR pressures) were possible reasons for this difference.39 Current evidence recommends training durations of 6-12 weeks and the use of personalized LL-BFR pressures (80% of limb occlusion pressure [LOP]) to achieve muscle strength and hypertrophy.23–25 In contrast to the previous studies, the non-BFR group of Hughes et al. did not consist of LLR but HLR training.35 In their study, ultrasound was used to examine vastus lateralis muscle thickness and no difference in muscle thickness was observed between LL-BFR and non-BFR training groups.35 Thus, the results of the present review are consistent with literature showing that LL-BFR training may be beneficial on quadriceps mass compared to LLR training and equally effective when compared to HLR training in healthy and postoperative patients.40–46
The application of LL-BFR has generally been indicated for the elderly or injured/postoperative patients who cannot tolerate high external loads.43,47–50 This review adds evidence on the application of LL-BFR as three studies assessing pain observed improved pain relief with LL-BFR compared to non-BFR training in patients following ACL surgery.18,35,36 This is in contrast with a recent systematic review that observed no significant difference in pain relief between LL-BFR and non-BFR training in individuals with knee joint pain.51 The study participants were heterogeneous and included individuals with patellofemoral pain, risk of symptomatic knee osteoarthritis, anterior knee pain and post knee arthroscopy.51 Furthermore, the heterogeneity in LL-BFR pressures and cuff width could explain the lack of effect on knee joint pain.51 Current evidence suggests that therapeutic restriction (defined as 80% of LOP) is achieved at lower LL-BFR pressures with wide compared to narrow cuffs.52–56 Furthermore, lower LL-BFR pressures are associated with less discomfort and greater safety.52–56 Thus, the use of non-personalized pressures without calculating the LOP may cause pain.52–56 In the present systematic review, all studies on knee joint pain used wide cuffs with an automatic personalized tourniquet system to calculate the LOP.18,35,36 Furthermore, all studies used HLR training as non-BFR training. Thus, pain relief may be the result of low external loads and hypoalgesia effects of LL-BFR training compared to HLR training.47,48,57,58
A major challenge in the rehabilitation after an ACL reconstruction is optimizing muscle strength while minimizing mechanical stress to the knee joint.59–61 The importance is represented by the remodeling process of the ACL graft. The remodeling process consists of three phases and the restructuring towards the properties of an intact (non-injured) ACL takes more than six months after reconstruction.21,62 Thereby, accelerated rehabilitation protocols and high load resistance training may compromise graft remodeling and may result in increased ACL graft laxity.19–21,63 BFR training in combination with low external loads has the advantage of minimizing mechanical stress to the knee joint compared to HLR training.47,48 However, in the present systematic review only two studies evaluated ACL graft laxity and showed no significant difference on ACL graft laxity with LL-BFR compared to non-BFR training.35,37 Therefore, more randomized controlled trials are needed to evaluate the effect of LL-BFR training on ACL graft laxity compared to HLR training.
The present systematic review has several limitations. First of all, due to the heterogeneity in intervention protocols and outcome measurements no meta-analysis could be performed. Secondly, differences in LL-BFR and non-BFR protocols affect the results of the present systematic review. Three studies compared LL-BFR training to HLR training, while three other studies compared LL-BFR training to LLR training.18,35–39 Furthermore, three of the six studies used LL-BFR protocols as recommended by current evidence.18,35,36 Thirdly, blinding of participants and personnel could not be performed or was unclear in the included studies.18,35–39 This could affect the results, as the patients may have experienced a nonspecific effect or a placebo effect due to the novel nature of LL-BFR training. Overall, the methodological quality of the included studies ranged from moderate to good. Lastly, no long-term effects of LL-BFR training after ACL reconstruction were reported.
CONCLUSION
The results of this systematic review indicate that LL-BFR training after ACL reconstruction may be beneficial on quadriceps strength, quadriceps mass, and knee joint pain compared to non-BFR training with non-detrimental effects on ACL graft laxity. However, more randomized controlled trials with operational definitions, standardized intervention protocols and outcome measurements are needed to add evidence on the clinical value of LL-BFR training.
Conflicts of Interest
The authors declare no conflicts.
Supplementary Material
References
- Ithurburn Matthew P., Altenburger Alex R., Thomas Staci, Hewett Timothy E., Paterno Mark V., Schmitt Laura C. Knee Surgery, Sports Traumatology, Arthroscopy. 2. Vol. 26. Springer Science and Business Media LLC; Young athletes after ACL reconstruction with quadriceps strength asymmetry at the time of return-to-sport demonstrate decreased knee function 1 year later; pp. 426–433. [DOI] [PubMed] [Google Scholar]
- Factors predicting quadriceps femoris muscle atrophy during the first 12 weeks following anterior cruciate ligament reconstruction. Grapar Žargi T., Drobnič Matej, Vauhnik Renata, Koder Jadran, Kacin Alan. Mar;2017 The Knee. 24(2):319–328. doi: 10.1016/j.knee.2016.11.003. doi: 10.1016/j.knee.2016.11.003. [DOI] [PubMed] [Google Scholar]
- Piussi Ramana, Broman Daniel, Musslinder Erik, Beischer Susanne, Thomeé Roland, Hamrin Senorski Eric. BMC Sports Science, Medicine and Rehabilitation. 1. Vol. 12. Springer Science and Business Media LLC; Recovery of preoperative absolute knee extension and flexion strength after ACL reconstruction; pp. 77–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quadriceps and hamstring strength symmetry after anterior cruciate ligament reconstruction: a prospective study. Harput G., Tunay V.B., Ithurburn M. 2020J Sports Rehabil. 30:1–8. doi: 10.1123/jsr.2019-0271. [DOI] [PubMed] [Google Scholar]
- Quadriceps muscle size following ACL injury and reconstruction: a systematic review. Birchmeier Thomas, Lisee Caroline, Kane Kevin, Brazier Brett, Triplett Ashley, Kuenze Christopher. 2020Journal of Orthopaedic Research. 38(3):598–608. doi: 10.1002/jor.24489. doi: 10.1002/jor.24489. [DOI] [PubMed] [Google Scholar]
- Garcia Steven A., Curran Michael T., Palmieri-Smith Riann M. Sports Health: A Multidisciplinary Approach. 3. Vol. 12. SAGE Publications; Longitudinal assessment of quadriceps muscle morphology before and after anterior cruciate ligament reconstruction and its associations with patient-reported outcomes; pp. 271–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fukunaga Takumi, Johnson Christopher D., Nicholas Stephen J., McHugh Malachy P. Knee Surgery, Sports Traumatology, Arthroscopy. 2. Vol. 27. Springer Science and Business Media LLC; Muscle hypotrophy, not inhibition, is responsible for quadriceps weakness during rehabilitation after anterior cruciate ligament reconstruction; pp. 573–579. [DOI] [PubMed] [Google Scholar]
- Kuenze Christopher M., Blemker Silvia S., Hart Joseph M. Journal of Orthopaedic Research. 9. Vol. 34. Wiley; Quadriceps function relates to muscle size following ACL reconstruction; pp. 1656–1662. [DOI] [PubMed] [Google Scholar]
- Muscle atrophy contributes to quadriceps weakness after anterior cruciate ligament reconstruction. Thomas Abbey C., Wojtys Edward M., Brandon Catherine, Palmieri-Smith Riann M. Jan;2016 Journal of Science and Medicine in Sport. 19(1):7–11. doi: 10.1016/j.jsams.2014.12.009. doi: 10.1016/j.jsams.2014.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quadriceps function, knee pain, and self-reported outcomes in patients with anterior cruciate ligament reconstruction. Lepley Adam S., Pietrosimone Brian, Cormier Marc L. Apr 1;2018 Journal of Athletic Training. 53(4):337–346. doi: 10.4085/1062-6050-245-16. doi: 10.4085/1062-6050-245-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Low rates of patients meeting return to sport criteria 9 months after anterior cruciate ligament reconstruction: a prospective longitudinal study. Welling Wouter, Benjaminse Anne, Seil Romain, Lemmink Koen, Zaffagnini Stefano, Gokeler Alli. Mar 24;2018 Knee Surgery, Sports Traumatology, Arthroscopy. 26(12):3636–3644. doi: 10.1007/s00167-018-4916-4. doi: 10.1007/s00167-018-4916-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Associations among quadriceps strength and rate of torque development 6 weeks post anterior cruciate ligament reconstruction and future hop and vertical jump performance: a prospective cohort study. Pua Yong-Hao, Mentiplay Benjamin F., Clark Ross A., Ho Jia-Ying. Oct 13;2017 Journal of Orthopaedic & Sports Physical Therapy. 47:845–852. doi: 10.2519/jospt.2017.7133. doi: 10.2519/jospt.2017.7133. [DOI] [PubMed] [Google Scholar]
- Ithurburn Matthew P., Paterno Mark V., Ford Kevin R., Hewett Timothy E., Schmitt Laura C. The American Journal of Sports Medicine. 11. Vol. 43. SAGE Publications; Young athletes with quadriceps femoris strength asymmetry at return to sport after anterior cruciate ligament reconstruction demonstrate asymmetric single-leg drop-landing mechanics; pp. 2727–2737. [DOI] [PubMed] [Google Scholar]
- The relationship between quadriceps strength asymmetry and knee biomechanics asymmetry during walking in individuals with anterior cruciate ligament reconstruction. Shi Huijuan, Huang Hongshi, Ren Shuang, Yu Yuanyuan, Liang Zixuan, Wang Qi, Hu Xiaoqing, Ao Yingfang. Sep;2019 Gait & Posture. 73:74–79. doi: 10.1016/j.gaitpost.2019.07.151. doi: 10.1016/j.gaitpost.2019.07.151. [DOI] [PubMed] [Google Scholar]
- Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Kyritsis Polyvios, Bahr Roald, Landreau Philippe, Miladi Riadh, Witvrouw Erik. May 23;2016 British Journal of Sports Medicine. 50(15):946–951. doi: 10.1136/bjsports-2015-095908. doi: 10.1136/bjsports-2015-095908. [DOI] [PubMed] [Google Scholar]
- Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Grindem Hege, Snyder-Mackler Lynn, Moksnes Håvard, Engebretsen Lars, Risberg May Arna. May 9;2016 British Journal of Sports Medicine. 50(13):804–808. doi: 10.1136/bjsports-2016-096031. doi: 10.1136/bjsports-2016-096031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Progression models in resistance training for healthy adults. American College of Sports Medicine Mar;2009 Medicine & Science in Sports & Exercise. 41(3):687–708. doi: 10.1249/mss.0b013e3181915670. doi: 10.1249/mss.0b013e3181915670. [DOI] [PubMed] [Google Scholar]
- Examination of the comfort and pain experienced with blood flow restriction training during post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: a UK national health service trial. Hughes Luke, Patterson Stephen David, Haddad Fares, Rosenblatt Benjamin, Gissane Conor, McCarthy Daniel, Clarke Thomas, Ferris Graham, Dawes Joanna, Paton Bruce. Sep;2019 Physical Therapy in Sport. 39:90–98. doi: 10.1016/j.ptsp.2019.06.014. doi: 10.1016/j.ptsp.2019.06.014. [DOI] [PubMed] [Google Scholar]
- An early return to vigorous activity may destabilize anterior cruciate ligaments reconstructed with hamstring grafts. Fujimoto Eisaku, Sumen Yoshio, Urabe Yukio, Deie Masataka, Murakami Yuji, Adachi Nobuo, Ochi Mitsuo. Feb;2004 Archives of Physical Medicine and Rehabilitation. 85(2):298–302. doi: 10.1016/s0003-9993(03)00621-x. doi: 10.1016/s0003-9993(03)00621-x. [DOI] [PubMed] [Google Scholar]
- Ménétrey J., Duthon V. B., Laumonier T., Fritschy D. Knee Surgery, Sports Traumatology, Arthroscopy. 3. Vol. 16. Springer Science and Business Media LLC; “Biological failure” of the anterior cruciate ligament graft; pp. 224–231. [DOI] [PubMed] [Google Scholar]
- Janssen Rob P. A., Scheffler Sven U. Knee Surgery, Sports Traumatology, Arthroscopy. 9. Vol. 22. Springer Science and Business Media LLC; Intra-articular remodelling of hamstring tendon grafts after anterior cruciate ligament reconstruction; pp. 2102–2108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rehabilitation after anterior cruciate ligament reconstruction: a prospective, randomized, double-blind comparison of programs administered over 2 different time intervals. Beynnon Bruce D., Uh Benjamin S., Johnson Robert J., Abate Joseph A., Nichols Claude E., Fleming Braden C., Poole A. Robin, Roos Harald. Mar;2005 The American Journal of Sports Medicine. 33(3):347–359. doi: 10.1177/0363546504268406. doi: 10.1177/0363546504268406. [DOI] [PubMed] [Google Scholar]
- The role of blood flow restriction therapy following knee surgery: expert opinion. DePhillipo Nicholas N., Kennedy Mitchell I., Aman Zach S., Bernhardson Andrew S., O'Brien Luke T., LaPrade Robert F. Aug;2018 Arthroscopy: The Journal of Arthroscopic & Related Surgery. 34(8):2506–2510. doi: 10.1016/j.arthro.2018.05.038. doi: 10.1016/j.arthro.2018.05.038. [DOI] [PubMed] [Google Scholar]
- Blood flow restriction and its function in post-operative anterior cruciate ligament reconstruction therapy: expert opinion. Humes C., Aguero S., Chahla J., Foad A. 2020Arch Bone Jt Surg. 8:570–574. doi: 10.22038/abjs.2020.42068.2145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blood flow restriction therapy: where we are and where we are going. Vopat Bryan G., Vopat Lisa M., Bechtold Megan M., Hodge Kevin A. Jun 15;2020 Journal of the American Academy of Orthopaedic Surgeons. 28(12):e493–e500. doi: 10.5435/jaaos-d-19-00347. doi: 10.5435/jaaos-d-19-00347. [DOI] [PubMed] [Google Scholar]
- Pearson Stephen John, Hussain Syed Robiul. Sports Medicine. 2. Vol. 45. Springer Science and Business Media LLC; A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy; pp. 187–200. [DOI] [PubMed] [Google Scholar]
- Mechanisms behind blood flow-restricted training and its effect toward muscle growth. Hwang Paul S., Willoughby Darryn S. Jul;2019 Journal of Strength and Conditioning Research. 33(1):S167–S179. doi: 10.1519/jsc.0000000000002384. doi: 10.1519/jsc.0000000000002384. [DOI] [PubMed] [Google Scholar]
- A systematic review of the effects of blood flow restriction training on muscle atrophy and circumference post ACL reconstruction. Charles Derek, White Ryan, Reyes Caleb, Palmer Drew. Dec;2020 International Journal of Sports Physical Therapy. 15(6):882–891. doi: 10.26603/ijspt20200882. doi: 10.26603/ijspt20200882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. Shamseer L., Moher D., Clarke M., Ghersi D., Liberati A., Petticrew M., Shekelle P., Stewart L. A., the PRISMA-P Group Jan 2;2015 BMJ. 349:g7647. doi: 10.1136/bmj.g7647. doi: 10.1136/bmj.g7647. [DOI] [PubMed] [Google Scholar]
- RefWorks Ann Arbour. [2021-2]. https://www.refworks.com/refworks2/ URL:
- Review Manager (RevMan) 5.4. [2021-2]. https://training.cochrane.org/ URL:
- ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. Sterne Jonathan AC, Hernán Miguel A, Reeves Barnaby C, Savović Jelena, Berkman Nancy D, Viswanathan Meera, Henry David, Altman Douglas G, Ansari Mohammed T, Boutron Isabelle, Carpenter James R, Chan An-Wen, Churchill Rachel, Deeks Jonathan J, Hróbjartsson Asbjørn, Kirkham Jamie, Jüni Peter, Loke Yoon K, Pigott Theresa D, Ramsay Craig R, Regidor Deborah, Rothstein Hannah R, Sandhu Lakhbir, Santaguida Pasqualina L, Schünemann Holger J, Shea Beverly, Shrier Ian, Tugwell Peter, Turner Lucy, Valentine Jeffrey C, Waddington Hugh, Waters Elizabeth, Wells George A, Whiting Penny F, Higgins Julian PT. Oct 12;2016 BMJ. 355:i4919. doi: 10.1136/bmj.i4919. doi: 10.1136/bmj.i4919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins J. P. T., Altman D. G., Gotzsche P. C., Juni P., Moher D., Oxman A. D., Savovic J., Schulz K. F., Weeks L., Sterne J. A. C., Cochrane Bias Methods Group. Cochrane Statistical Methods Group . BMJ. oct18 2. Vol. 343. BMJ; The Cochrane Collaboration's tool for assessing risk of bias in randomised trials; pp. d5928–d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cumpston Miranda, Li Tianjing, Page Matthew J, Chandler Jacqueline, Welch Vivian A, Higgins Julian PT, Thomas James. Cochrane Editorial Unit, editor. Oct 3;2019 Cochrane Database of Systematic Reviews. 10:ed000142 doi: 10.1002/14651858.ed000142. doi: 10.1002/14651858.ed000142. [DOI] [PMC free article] [PubMed]
- Comparing the effectiveness of blood flow restriction and traditional heavy load resistance training in the post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: a UK national health service randomised controlled trial. Hughes Luke, Rosenblatt Benjamin, Haddad Fares, Gissane Conor, McCarthy Daniel, Clarke Thomas, Ferris Graham, Dawes Joanna, Paton Bruce, Patterson Stephen David. Jul 12;2019 Sports Medicine. 49(11):1787–1805. doi: 10.1007/s40279-019-01137-2. doi: 10.1007/s40279-019-01137-2. [DOI] [PubMed] [Google Scholar]
- Comparison of the acute perceptual and blood pressure response to heavy load and light load blood flow restriction resistance exercise in anterior cruciate ligament reconstruction patients and non-injured populations. Hughes Luke, Paton Bruce, Haddad Fares, Rosenblatt Benjamin, Gissane Conor, Patterson Stephen David. Sep;2018 Physical Therapy in Sport. 33:54–61. doi: 10.1016/j.ptsp.2018.07.002. doi: 10.1016/j.ptsp.2018.07.002. [DOI] [PubMed] [Google Scholar]
- Low-load resistance muscular training with moderate restriction of blood flow after anterior cruciate ligament reconstruction. Ohta Haruyasu, Kurosawa Hisashi, Ikeda Hiroshi, Iwase Yoshiyuki, Satou Naohiro, Nakamura Shinji. Jan;2003 Acta Orthopaedica Scandinavica. 74(1):62–68. doi: 10.1080/00016470310013680. doi: 10.1080/00016470310013680. [DOI] [PubMed] [Google Scholar]
- Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles. Takarada YUDAI, Takazawa HARUO, Ishii NAOKATA. Dec;2000 Medicine and Science in Sports and Exercise. 32(12):2035–2039. doi: 10.1097/00005768-200012000-00011. doi: 10.1097/00005768-200012000-00011. [DOI] [PubMed] [Google Scholar]
- Intermittent blood flow restriction does not reduce atrophy following anterior cruciate ligament reconstruction. Iversen Erik, Røstad Vibeke, Larmo Arne. Mar;2016 Journal of Sport and Health Science. 5(1):115–118. doi: 10.1016/j.jshs.2014.12.005. doi: 10.1016/j.jshs.2014.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quadriceps strengthening with blood flow restriction for the rehabilitation of patients with knee conditions: a systematic review with meta-analysis. Van Cant Joachim, Dawe-Coz Alexander, Aoun Elie, Esculier Jean-François. Jul 20;2020 Journal of Back and Musculoskeletal Rehabilitation. 33(4):529–544. doi: 10.3233/bmr-191684. doi: 10.3233/bmr-191684. [DOI] [PubMed] [Google Scholar]
- The blood flow restriction training effect in knee osteoarthritis people: a systematic review and meta-analysis. Ferlito João Vitor, Pecce Samantha Angelica Pasa, Oselame Lucas, De Marchi Thiago. Aug 10;2020 Clinical Rehabilitation. 34(11):1378–1390. doi: 10.1177/0269215520943650. doi: 10.1177/0269215520943650. [DOI] [PubMed] [Google Scholar]
- Effect of blood‐flow restricted vs heavy‐load strength training on muscle strength: systematic review and meta‐analysis. Grønfeldt Birk Mygind, Lindberg Nielsen Jakob, Mieritz Rune Mygind, Lund Hans, Aagaard Per. May;2020 Scandinavian Journal of Medicine & Science in Sports. 30(5):837–848. doi: 10.1111/sms.13632. doi: 10.1111/sms.13632. [DOI] [PubMed] [Google Scholar]
- Blood flow-restricted training for lower extremity muscle weakness due to knee pathology: a systematic review. Barber-Westin Sue, Noyes Frank R. 2019Sports Health: A Multidisciplinary Approach. 11(1):69–83. doi: 10.1177/1941738118811337. doi: 10.1177/1941738118811337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Effects of blood flow restriction training on muscular strength and hypertrophy in older individuals: a systematic review and meta-Analysis. Centner Christoph, Wiegel Patrick, Gollhofer Albert, König Daniel. 2019Sports Medicine. 49(1):95–108. doi: 10.1007/s40279-018-0994-1. doi: 10.1007/s40279-018-0994-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. Hughes Luke, Paton Bruce, Rosenblatt Ben, Gissane Conor, Patterson Stephen David. Mar 4;2017 British Journal of Sports Medicine. 51(13):1003–1011. doi: 10.1136/bjsports-2016-097071. doi: 10.1136/bjsports-2016-097071. [DOI] [PubMed] [Google Scholar]
- Magnitude of muscle strength and mass adaptations between high-load resistance training versus low-load resistance training associate with blood-flow restriction: a systematic review and meta-analysis. Lixandrão Manoel E., Ugrinowitsch Carlos, Berton Ricardo, Vechin Felipe C., Conceição Miguel S., Damas Felipe, Libardi Cleiton A., Roschel Hamilton. 2018Sports Medicine. 48(2):361–378. doi: 10.1007/s40279-017-0795-y. doi: 10.1007/s40279-017-0795-y. [DOI] [PubMed] [Google Scholar]
- Benefits of resistance training with blood flow restriction in knee osteoarthritis. Ferraz RODRIGO BRANCO, Gualano BRUNO, Rodrigues REYNALDO, KURIMORI CECI OBARA, FULLER RICARDO, LIMA FERNANDA RODRIGUES, DE SÁ-PINTO ANA LÚCIA, ROSCHEL HAMILTON. May;2018 Medicine & Science in Sports & Exercise. 50(5):897–905. doi: 10.1249/mss.0000000000001530. doi: 10.1249/mss.0000000000001530. [DOI] [PubMed] [Google Scholar]
- Exercises with partial vascular occlusion in patients with knee osteoarthritis: a randomized clinical trial. Bryk Flavio Fernandes, dos Reis Amir Curcio, Fingerhut Deborah, Araujo Thomas, Schutzer Marcela, Cury Ricardo de Paula Leite, Duarte Aires Jr., Fukuda Thiago Yukio. Mar 12;2016 Knee Surgery, Sports Traumatology, Arthroscopy. 24(5):1580–1586. doi: 10.1007/s00167-016-4064-7. doi: 10.1007/s00167-016-4064-7. [DOI] [PubMed] [Google Scholar]
- Low-load resistance training with blood flow restriction improves clinical outcomes in musculoskeletal rehabilitation: a single-blind randomized controlled Trial. Ladlow Peter, Coppack Russell J., Dharm-Datta Shreshth, Conway Dean, Sellon Edward, Patterson Stephen D., Bennett Alexander N. Sep 10;2018 Frontiers in Physiology. 9:1269. doi: 10.3389/fphys.2018.01269. doi: 10.3389/fphys.2018.01269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blood flow restriction training after knee arthroscopy: a randomized controlled pilot study. Tennent David J., Hylden Christina M., Johnson Anthony E., Burns Travis C., Wilken Jason M., Owens Johnny G. May;2017 Clinical Journal of Sport Medicine. 27(3):245–252. doi: 10.1097/jsm.0000000000000377. doi: 10.1097/jsm.0000000000000377. [DOI] [PubMed] [Google Scholar]
- The addition of blood flow restriction to resistance exercise in individuals with knee pain: a systematic review and meta-analysis. Cuyul-Vásquez Iván, Leiva-Sepúlveda Alejandro, Catalán-Medalla Oscar, Araya-Quintanilla Felipe, Gutiérrez-Espinoza Hector. Nov;2020 Brazilian Journal of Physical Therapy. 24(6):465–478. doi: 10.1016/j.bjpt.2020.03.001. doi: 10.1016/j.bjpt.2020.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blood flow restriction exercise: effects of sex, cuff width, and cuff pressure on perceived lower body discomfort. Spitz Robert W., Chatakondi Raksha N., Bell Zachary W., Wong Vickie, Viana Ricardo B., Dankel Scott J., Abe Takashi, Yamada Yujiro, Loenneke Jeremy P. 2021Perceptual and Motor Skills. 128(1):353–374. doi: 10.1177/0031512520948295. doi: 10.1177/0031512520948295. [DOI] [PubMed] [Google Scholar]
- The effect of cuff width for determining limb occlusion pressure: a comparison of blood flow restriction devices. Weatherholt A.M., Vanwye W.R., Lohmann J., Owens J.G. 2019J Exerc Sci. 12:136–143. doi: 10.70252/RWVU7100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Influence of cuff width, sex, and race on arterial occlusion: implications for blood flow restriction research. Jessee Matthew B., Buckner Samuel L., Dankel Scott J., Counts Brittany R., Abe Takashi, Loenneke Jeremy P. Jan 28;2016 Sports Medicine. 46(6):913–921. doi: 10.1007/s40279-016-0473-5. doi: 10.1007/s40279-016-0473-5. [DOI] [PubMed] [Google Scholar]
- Effects of cuff width on arterial occlusion: implications for blood flow restricted exercise. Loenneke Jeremy P., Fahs Christopher A., Rossow Lindy M., Sherk Vanessa D., Thiebaud Robert S., Abe Takashi, Bemben Debra A., Bemben Michael G. 2012European Journal of Applied Physiology. 112(8):2903–2912. doi: 10.1007/s00421-011-2266-8. doi: 10.1007/s00421-011-2266-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blood flow restricted exercise and discomfort: a review. Spitz Robert W., Wong Vickie, Bell Zachary W., Viana Ricardo B., Chatakondi Raksha N., Abe Takashi, Loenneke Jeremy P. 2022Journal of Strength and Conditioning Research. 36(3):871–879. doi: 10.1519/jsc.0000000000003525. doi: 10.1519/jsc.0000000000003525. [DOI] [PubMed] [Google Scholar]
- Blood flow restriction induces hypoalgesia in recreationally active adult male anterior knee pain patients allowing therapeutic exercise loading. Korakakis Vasileios, Whiteley Rodney, Epameinontidis Konstantinos. Jul;2018 Physical Therapy in Sport. 32:235–243. doi: 10.1016/j.ptsp.2018.05.021. doi: 10.1016/j.ptsp.2018.05.021. [DOI] [PubMed] [Google Scholar]
- Low load resistance training with blood flow restriction decreases anterior knee pain more than resistance training alone. a pilot randomised controlled trial. Korakakis Vasileios, Whiteley Rodney, Giakas Giannis. Nov;2018 Physical Therapy in Sport. 34:121–128. doi: 10.1016/j.ptsp.2018.09.007. doi: 10.1016/j.ptsp.2018.09.007. [DOI] [PubMed] [Google Scholar]
- ACL reconstruction with hamstring tendon autograft and accelerated brace-free rehabilitation: a systematic review of clinical outcomes. Janssen Rob P A, van Melick Nicky, van Mourik Jan B A, Reijman Max, van Rhijn Lodewijk W. Apr;2018 BMJ Open Sport & Exercise Medicine. 4(1):2017–20000301. doi: 10.1136/bmjsem-2017-000301. doi: 10.1136/bmjsem-2017-000301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rehabilitation after anterior cruciate ligament reconstruction: a systematic review. Kruse L.M., Gray B., Wright R.W. Oct 3;2012 Journal of Bone and Joint Surgery. 94(19):1737–1748. doi: 10.2106/jbjs.k.01246. doi: 10.2106/jbjs.k.01246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Athletes with bone-patellar tendon bone autograft for anterior cruciate ligament reconstruction were slower to meet rehabilitation milestones and return-to-sport criteria than athletes with hamstring tendon autograft or soft tissue allograft: secondary analysis from the ACL-SPORTS trial. Smith Angela Hutchinson, Capin Jacob J., Zarzycki Ryan, Snyder-Mackler Lynn. May;2020 Journal of Orthopaedic & Sports Physical Therapy. 50(5):259–266. doi: 10.2519/jospt.2020.9111. doi: 10.2519/jospt.2020.9111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Assessment of graft maturity after anterior cruciate ligament reconstruction using autografts: a systematic review of biopsy and magnetic resonance imaging studies. van Groningen Bart, van der Steen M.C., Janssen Daan M., van Rhijn Lodewijk W., van der Linden Antoine N., Janssen Rob P.A. Aug;2020 Arthroscopy, Sports Medicine, and Rehabilitation. 2(4):377–388. doi: 10.1016/j.asmr.2020.02.008. doi: 10.1016/j.asmr.2020.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Accelerated versus nonaccelerated rehabilitation after anterior cruciate ligament reconstruction: a prospective, randomized, double-blind investigation evaluating knee joint laxity using roentgen stereophotogrammetric analysis. Beynnon Bruce D., Johnson Robert J., Naud Shelly, Fleming Braden C., Abate Joseph A., Brattbakk Bjarne, Nichols Claude E. Sep 27;2011 The American Journal of Sports Medicine. 39(12):2536–2548. doi: 10.1177/0363546511422349. doi: 10.1177/0363546511422349. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.