
Fig. 1. Hypertrophic pyloric stenosis.
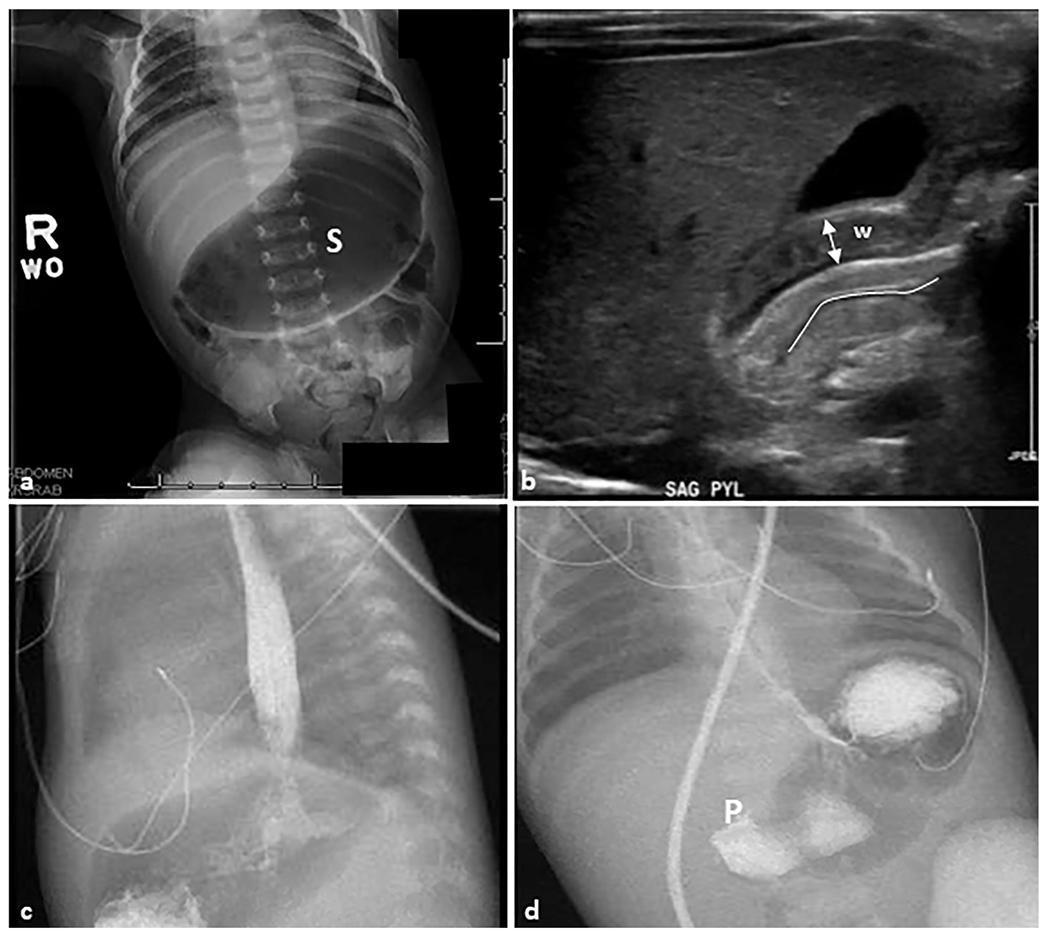
A 28-day-old female patient presented with non-bilious emesis and abdominal distension. (a) Anteroposterior abdominal radiograph demonstrating a markedly distended gas-filled stomach (S) without signs of perforation. (b) Sagittal grayscale ultrasound image reveals a thickening of the pyloric muscle wall (W) that measures 4 mm (double-headed arrow). The pyloric channel is elongated and measures 19 mm (line) and the pylorus does not open on dynamic imaging. (c, d) Sagittal and anteroposterior view contrast upper GI series show contrast crosses the lower esophageal sphincter into the air-distended stomach. There is no contrast passage across the pylorus (P), which is consistent with the previous findings.