
Figure 2.
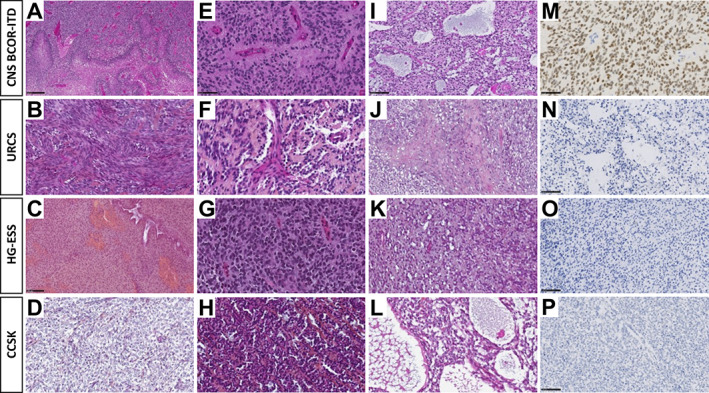
Histopathology of BCOR‐ITD tumours. Each line shows histopathological and immunohistochemical findings of one representative case of CNS BCOR‐ITD, URCS, ESS, and CCSK. A case of CNS BCOR‐ITD showing pseudo‐palisading necrosis (A, HPS, magnification, ×100), ependymal pseudorosettes (E, HPS, magnification, ×400), microcystic modifications (I, HPS, magnification, ×200), and diffuse Olig2 immunoexpression (M, magnification, ×400). A case of URCS showing a fascicular pattern composed of spindle cells (B, HPS, magnification, ×400), with some papillary structures and pseudorosettes (F, HPS, magnification, ×400), necrosis, and apoptotic bodies (J, HPS, magnification, ×200), without immunoexpression for Olig2 (N, magnification, ×200). A case of ESS showing spindle cells (C, HPS, magnification, ×200), some pseudorosettes (G, HPS, magnification, ×400), and microcysts (K, HPS, magnification, ×200), with no expression of Olig2 (O, magnification, ×200). A case of CCSK showing an alveolar pattern (D, HPS, magnification, ×400), with some pseudorosettes (H, HPS, magnification, ×400), and microcysts (L, HPS, magnification, ×400), but without immunostaining for Olig2 (P, magnification, ×200). HPS, haematoxylin phloxine saffron. Black scale bars represent 50 μm (E, M), 100 μm (I, N, C, O, P), and 250 μm (A).