
Figure 2.
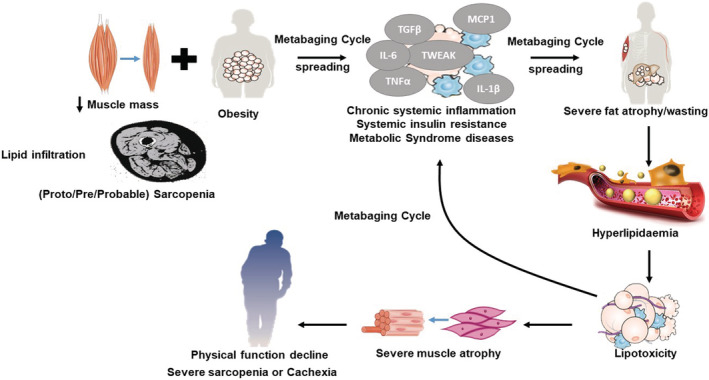
Resolving the obesity paradox. During ageing, adipose inflammation leads to the redistribution of fat to the intra‐abdominal area (visceral fat) and fatty infiltration into muscle. Intramuscular fat infiltration increases the chances of progression to obesity, which reduced muscular renewal, progressing to pre‐sarcopenia. This synergy between muscle loss (pre‐sarcopenia) and fatty infiltration (myosteatosis) might trigger and aggravate the pathogenesis of sarcopenic obesity (SO), low‐grade inflammation (inflammaging) and systemic insulin resistance. SO patients may appear as ‘normal’ subjects due to the mutual masking effect of sarcopenia and obesity. The vicious cycle of local myosteatosis and muscle insulin resistance can complete a larger vicious cycle leading to increasing lipolysis and local free fatty acid concentrations (the metabaging cycle), thereby worsening and spreading the local hyperlipidaemia. But after a long period of systemic inflammaging, chronic inflammation would exhaust both extant and newly formed adipose depots, leading to the systemic atrophy and wasting observed in cachexia and full‐blown sarcopenia. This suggests that SO may progress to full‐blown sarcopenia in the same way that cachexia develops: systemic inflammation‐induced adipose atrophy, which unmasks and exacerbates the muscle atrophy.