

Abstract
Purpose
Selective serotonin re-uptake inhibitors (SSRIs) are frequently used to treat premature ejaculation (PE) in men. We performed a Cochrane review to assess the efficacy of SSRI treatment for PE.
Materials and Methods
We extensively searched a range of databases up to May 2020 and only included randomized controlled trials.
Results
A total of 31 studies with 8,254 men were included in this analysis. We found that SSRI treatment probably improves self-perceived PE symptoms (defined as a rating of ‘better’ or ‘much better’; risk ratio [RR], 1.92; 95% confidence interval [CI], 1.66–2.23; moderate-certainty evidence) and satisfaction with intercourse (defined as a rating of ‘good’ or ‘very good’; RR, 1.63; 95% CI, 1.42–1.87; moderate-certainty evidence) compared to placebo. Furthermore, SSRI treatment likely improve participants’ self-perceived control over ejaculation (defined as rating of ‘good’ or ‘very good’; RR, 2.29; 95% CI, 1.72–3.05; moderate-certainty evidence) and probably lessens distress (defined as rating of ‘a little bit’ or ‘not at all’) about PE (RR, 1.54; 95% CI, 1.26–1.88; moderate-certainty evidence). SSRI treatment may increase IELT compared to placebo (mean difference, 3.09 minutes higher; 95% CI, 1.94 higher to 4.25 higher; low-certainty evidence). However, SSRIs may increase treatment cessations due to adverse events compared to placebo (RR, 3.80; 95% CI, 2.61–5.51; low-certainty evidence).
Conclusions
SSRI treatment for PE appears to substantially improve a number of outcomes of direct patient importance such as symptom improvement, satisfaction with intercourse and perceived control over ejaculation when compared to placebo.
Keywords: Meta-analysis, Premature ejaculation, Serotonin and noradrenaline reuptake inhibitors, Systematic review
INTRODUCTION
Premature ejaculation (PE) is reported to effect a significant proportion of men with an estimated prevalence of 5% to 30% [1,2,3] and can have a significant negative impact on quality of life. In a community-based observation study, Rowland et al [4] reported that men with PE and their partners reported lower levels of sexual functioning and satisfaction, and higher levels of personal distress and interpersonal difficulty. PE can foster feelings of inadequacy, disappointment and anxiety [5]. In addition to adverse impacts on sexual function and relationships, the consequences of PE can permeate to other domains and negatively affect overall quality of life [6].
There are a range of treatments that have been recommended as treatments for PE [7]. Selective serotonin re-uptake inhibitors (SSRIs), which is mainly used as a treatment for depression, have been prescribed off-label to men experiencing PE. There have been several reviews already conducted examining the effectiveness of SSRI medication for the treatment of PE but none have been performed in a rigorous manner and are relatively outdated [8,9,10].
Therefore, we aimed to conduct a systematic review and meta-analysis in accordance with Cochrane guidelines to assess the effects of SSRIs in the treatment of PE in adult men.
MATERIALS AND METHODS
The full protocol of this review was published a priori in the Cochrane Database of Systematic Reviews [11].
We extensively searched a number of databases including PUBMED Medline, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Latin American and Caribbean Health Sciences Literature (LILACS), Cumulative Index of Nursing and Allied Health Literature (CINAHL) and World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) up to May 2020. We also searched the grey literature and the abstracts of major urological meetings.
We included studies of men aged ≥18 years with lifelong PE only (from first sexual experience). We excluded men with PE secondary to other known conditions such as prostatitis or PE as a medication side effect (acquired PE). We only included RCTs in which participants were allocated to receive either SSRI or placebo/no treatment. We also included cross-over clinical trials. We did not include agents classified as serotonin-norepinephrine re-uptake inhibitors such as duloxetine.
The primary outcomes were:
· Participant perception of change with treatment: assessed using the Clinical Global Impression of Change (CGIC) questionnaire, we recorded the number of participants describing the change as ‘better’ or ‘much better’ after treatment in a dichotomous manner.
· Participant satisfaction with intercourse: we recorded the number of participants describing their satisfaction as ‘good’ or ‘very good’ before and after treatment (for satisfaction and control) using the CGIC.
· Study withdrawal due to adverse events.
The secondary outcomes were:
· Perceived control over ejaculation: using the PEP questionnaire, the recorded the number of participants describing their satisfaction as ‘good’ or ‘very good’ before and after treatment (for satisfaction and control).
· Participant distress about PE: we recorded the number of participants describing their distress as ‘a little bit’ or ‘not at all’ using the PEP questionnaire.
· Relationship difficulties: we recorded the number of participants describing their difficulties as ‘a little bit’ or ‘not at all’ using the PEP questionnaire.
· Adverse events
· Intravaginal ejaculatory latency time (IELT)
· Depression
We expected the following characteristics to introduce clinical heterogeneity, and carried out the following subgroup analyses including investigation of interactions.
· Long-acting SSRIs (e.g., paroxetine, fluoxetine, sertraline, citalopram and fluvoxamine) versus short-acting (on-demand type) SSRIs (e.g., dapoxetine). We compared the long- versus short-acting SSRIs.
· Among the long-acting SSRIs, comparison of individual agents (e.g., paroxetine versus fluoxetine versus sertraline versus citalopram versus fluvoxamine).
· If applicable, different dose levels (e.g., dapoxetine 30 mg versus 60 mg).
Statistical analysis
Statistical analysis was conducted in accordance with the Cochrane Handbook for Systematic Reviews. Random effects models were used for all analyses.
RESULTS
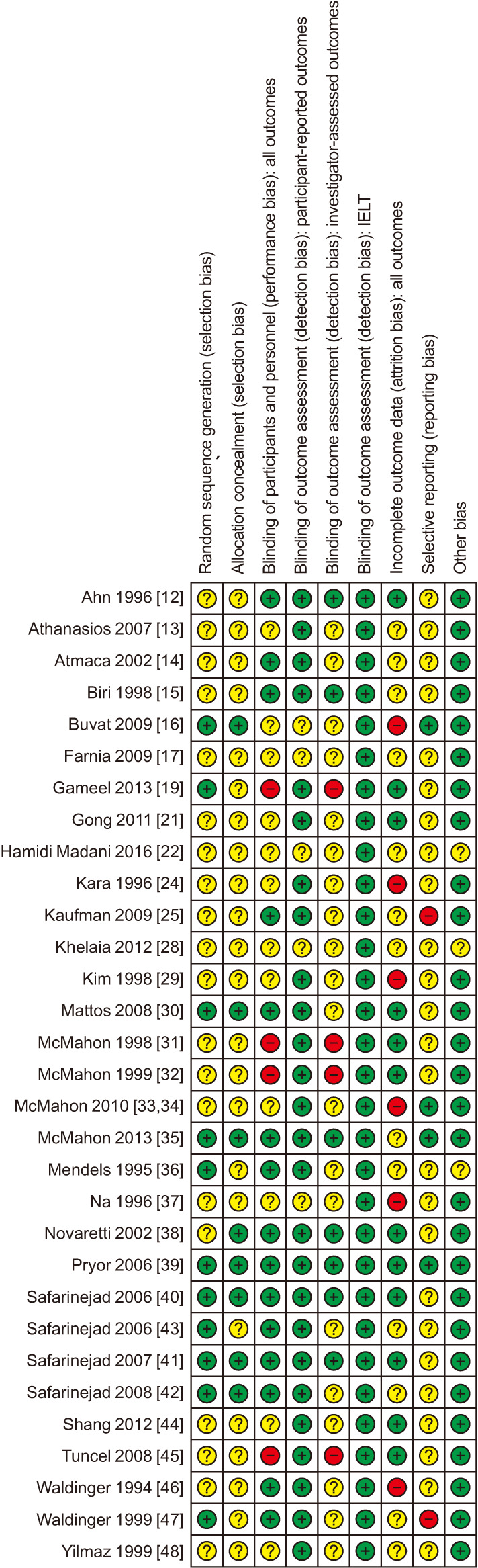
Our search retrieved 1,218 references from which 31 studies were included in this analysis after abstract screening and full-text review [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48] (Supplement Fig. 1). We included 8,049 randomized participants (SSRI 4,990, placebo 2,928, other drug 131). The included studies tested a range of SSRIs including fluoxetine, duloxetine, citalopram, sertraline, dapoxetine, paroxetine, escitalopram, and fluvoxamine. The characteristics of included studies can be found in Supplement Table 1. The risk of bias assessment is shown in Fig. 1.
Fig. 1. Risk of bias assessment.
The GRADE summary of findings is outlined in Table 1. A detailed description of the results of this review including the subgroup analyses is available in the original review [49].
Table 1. SSRI compared to placebo for premature ejaculation in adult men.
| Outcomes | No. of participants (studies) |
Certainty of the evidence (GRADEa) |
Relative effect (95% CI) |
Anticipated absolute effectsb (95% CI) | What happens | |
|---|---|---|---|---|---|---|
| Risk with placebo | Risk difference with SSRI | |||||
| Participant perception of change with treatment assessed with: Clinical Global Impression of Change questionnaire (event is good as it represents improvement in symptoms) | 3,260 (6 RCTs) |
⊕⊕⊕⊝ Moderatec |
RR 1.92 (1.66–2.23) |
Study population | SSRI probably results in perceived improvement compared to placebo. | |
| 220 per 1,000 | 202 more per 1,000 (145 more to 270 more) |
|||||
| Participant satisfaction with intercourse assessed with: Premature Ejaculation Profile questionnaire (event is good as it represents increased satisfaction) | 4,273 (3 RCTs) |
⊕⊕⊕⊝ Moderatec,d |
RR 1.63 (1.42–1.87) |
Study population | SSRI probably results in improved satisfaction with intercourse compared to placebo. | |
| 278 per 1,000 | 175 more per 1,000 (117 more to 242 more) |
|||||
| Study withdrawal due to adverse events | 7,367 (20 RCTs) |
⊕⊕⊝⊝ Lowc,e |
RR 3.80 (2.61–5.51) |
Study population | SSRI may result in more withdrawals due to adverse events compared to placebo. | |
| 11 per 1,000 | 30 more per 1,000 (17 more to 49 more) |
|||||
| Perceived control over ejaculation assessed with: Premature Ejaculation Profile questionnaire (event is good as it represents increased control over ejaculation) | 4,273 (3 RCTs) |
⊕⊕⊕⊝ Moderate |
RR 2.29 (1.72–3.05) |
Study population | SSRI probably results in improved perceived control over ejaculation compared to placebo. | |
| 132 per 1,000 | 170 more per 1,000 (95 more to 270 more) |
|||||
| Participant distress about PE assessed with: Premature Ejaculation Profile questionnaire (event is good as it represents less distress) | 652 (1 RCT) |
⊕⊕⊕⊝ Moderate |
RR 1.54 (1.26–1.88) |
Study population | SSRI probably results in increased numbers of men not distressed about PE compared to placebo. | |
| 353 per 1,000 | 191 more per 1,000 (92 more to 311 more) |
|||||
| Adverse events | 4,624 (17 RCTs) |
⊕⊕⊕⊝ Moderatec |
RR 1.71 (1.48–1.99) |
Study population | SSRI probably results in increased adverse events compared to placebo. | |
| 243 per 1,000 | 173 more per 1,000 (117 more to 241 more) |
|||||
| IELT | 5,872 (20 RCTs) |
⊕⊕⊝⊝ Lowc,f |
- | Study population | SSRI probably results in extended IELT compared to placebo. | |
| The mean IELT was 1.41 minutes | MD 3.09 minutes higher (1.94 higher to 4.25 higher) |
|||||
Patient or population: adult men with premature ejaculation. Setting: outpatient. Intervention: SSRI. Comparison: placebo.
CI: confidence interval, RCT: randomized controlled trial, RR: risk ratio, SSRI: selective serotonin re-uptake inhibitor, PE: premature ejaculation, IELT: intravaginal ejaculatory latency time, MD: mean difference.
aGRADE Working Group grades of evidence: (1) High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. (2) Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. (3) Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. (4) Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
bThe risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
cDowngraded one level for study limitations: most studies had an unclear or high risk of selection, performance and detection bias.
dNot downgraded for high I2 statistic since observed inconsistency did not appear clinically relevant.
eDowngraded one level due to serious concerns regarding attrition bias.
fDowngraded one level for serious inconsistency.
1. Primary outcomes
SSRI treatment probably results in an improvement in PE-related symptoms defined as a rating of ‘better’ or ‘much better’ using the CGIC questionnaire compared to placebo (risk ratio [RR], 1.92; 95% confidence interval [CI], 1.66–2.23; I2=24%; studies=6, participants=3,260; moderate certainty of evidence).
SSRI treatment probably improves satisfaction with intercourse defined as a rating of ‘good’ or ‘very good’ using the CGIC questionnaire compared to placebo (RR, 1.63; 95% CI, 1.42–1.87; I2=53%; studies=3, participants=4,273; moderate certainty of evidence).
However, SSRI treatment may result in an increase in the number of treatment cessations due to adverse events compared to placebo (RR, 3.80; 95% CI, 2.61–5.51; I2=0%; studies=20, participants=7,367; low certainty of evidence).
2. Secondary outcomes
SSRI treatment probably improves participants’ control over ejaculation defined as a rating of ‘good’ or ‘very good’ based on the PEP questionnaire compared to placebo (RR, 2.29; 95% CI, 1.72–3.05; I2=75%; studies=3, participants=4,273; moderate certainty of evidence).
Furthermore, SSRI treatment probably decreases PE-related distress defined as ‘a little bit’ or ‘not at all’ distressing based on the PEP questionnaire compared to placebo (RR, 1.54; 95% CI, 1.26–1.88; studies=1, participants=652; moderate certainty of evidence).
Treatment with SSRIs may reduce relationship difficulties to only ‘a little bit’ or ‘not at all’ based on the PEP questionnaire compared to placebo (RR, 1.20; 95% CI, 1.07–1.34; studies=1, participants=652; low certainty of evidence).
Additionally, SSRI treatment may increase IELT compared to placebo (mean difference 3.09 minutes higher; 95% CI, 1.94 higher to 4.25 higher; I2=99%; studies=20, participants=5,872; low certainty of evidence).
SSRI treatment probably increases adverse events substantially compared to placebo (RR, 1.71; 95% CI, 1.48–1.99; I2=41%; studies=17, participants=4,624; moderate certainty of evidence).
We are very uncertain whether SSRI treatment compared to placebo increases depression (RR, 2.00; 95% CI, 0.23–17.34; studies=1, participants=14; vert low certainty of evidence).
DISCUSSION
This comprehensive systematic review and meta-analysis included 31 studies with 8,254 participants and found that compared to placebo, SSRI treatment for PE probably improves perception of change with treatment, satisfaction with intercourse, perceived control over ejaculation, participant distress about PE, relationship difficulties, and IELT. However, the administration of SSRIs may increase study withdrawals due to adverse events and probably increases adverse events. These findings are consistent with other published reviews on the topic [8,10,50].
We consistently downgraded the certainty of evidence by one or two steps to moderate or low. Our confidence in the estimates of effect were primarily limited by study limitations and heterogeneity. Most studies were classified at unclear or high risk of bias for multiple domains and, therefore, the potential biases in those studies introduced a degree of uncertainty in the calculated summary estimates.
CONCLUSIONS
Compared to placebo, the administration of SSRIs for PE may improve perception of change with treatment and satisfaction with intercourse. SSRIs may also improve perceived control over ejaculation and reduce both distress about PE and relationship difficulties. These potential benefits need to be weighed up against the possible increase in adverse events with SSRIs.
Acknowledgements
This article is based on a Cochrane Review published in the Cochrane Database of Systematic Reviews (CDSR) 2021, Issue 6, DOI: 10.1002/14651858.CD012799.pub2. (see cochranelibrary.com for information). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and the CDSR should be consulted for the most recent version of the review.
We thank Cochrane Urology for its support. We are grateful to Dr Yu Xie for translating articles. We are also appreciative of the feedback provided by Dr Josip Vukina, MD, MPH (University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA) and Dr Ege Can Serefoglu, MD, FECSM (Professor of Urology, Biruni University School of Medicine, Istanbul, Turkey; Editor-in-Chief, International Journal of Impotence Research, London, UK) who served as peer referees.
Footnotes
Conflict of Interest: The authors have nothing to disclose.
Funding: None.
- Conceptualization: NJS, RM, ECH, JAB, SS, PD.
- Data curation: NJS, ECH, JAL, RM, AS.
- Formal analysis: NJS, ECH.
- Investigation: JAB, SS, PD.
- Methodology: NJS, JAL, ECH, RM, JAB, SS, PD.
- Supervision: JAB, PD.
- Writing—original draft: NJS, ECH, JAL, PD.
- Writing—review & editing: RM, JAB, AS, SS.
Supplementary Materials
Supplementary materials can be found via https://doi.org/10.5534/wjmh.210155.
PRISMA study flowchart.
Characteristics of included studies
References
- 1.McMahon CG, Lee G, Park JK, Adaikan PG. Premature ejaculation and erectile dysfunction prevalence and attitudes in the Asia-Pacific region. J Sex Med. 2012;9:454–465. doi: 10.1111/j.1743-6109.2011.02507.x. [DOI] [PubMed] [Google Scholar]
- 2.Gao J, Zhang X, Su P, Liu J, Xia L, Yang J, et al. Prevalence and factors associated with the complaint of premature ejaculation and the four premature ejaculation syndromes: a large observational study in China. J Sex Med. 2013;10:1874–1881. doi: 10.1111/jsm.12180. [DOI] [PubMed] [Google Scholar]
- 3.Lee SW, Lee JH, Sung HH, Park HJ, Park JK, Choi SK, et al. The prevalence of premature ejaculation and its clinical characteristics in Korean men according to different definitions. Int J Impot Res. 2013;25:12–17. doi: 10.1038/ijir.2012.27. [DOI] [PubMed] [Google Scholar]
- 4.Rowland DL, Patrick DL, Rothman M, Gagnon DD. The psychological burden of premature ejaculation. J Urol. 2007;177:1065–1070. doi: 10.1016/j.juro.2006.10.025. [DOI] [PubMed] [Google Scholar]
- 5.Revicki D, Howard K, Hanlon J, Mannix S, Greene A, Rothman M. Characterizing the burden of premature ejaculation from a patient and partner perspective: a multi-country qualitative analysis. Health Qual Life Outcomes. 2008;6:33. doi: 10.1186/1477-7525-6-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rosen RC, Althof S. Impact of premature ejaculation: the psychological, quality of life, and sexual relationship consequences. J Sex Med. 2008;5:1296–1307. doi: 10.1111/j.1743-6109.2008.00825.x. [DOI] [PubMed] [Google Scholar]
- 7.Althof SE, McMahon CG, Waldinger MD, Serefoglu EC, Shindel AW, Adaikan PG, et al. An update of the International Society of Sexual Medicine's guidelines for the diagnosis and treatment of premature ejaculation (PE) Sex Med. 2014;2:60–90. doi: 10.1002/sm2.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jian Z, Wei X, Ye D, Li H, Wang K. Pharmacotherapy of premature ejaculation: a systematic review and network meta-analysis. Int Urol Nephrol. 2018;50:1939–1948. doi: 10.1007/s11255-018-1984-9. [DOI] [PubMed] [Google Scholar]
- 9.Yi ZM, Chen SD, Tang QY, Tang HL, Zhai SD. Efficacy and safety of sertraline for the treatment of premature ejaculation: systematic review and meta-analysis. Medicine (Baltimore) 2019;98:e15989. doi: 10.1097/MD.0000000000015989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Castiglione F, Albersen M, Hedlund P, Gratzke C, Salonia A, Giuliano F. Current pharmacological management of premature ejaculation: a systematic review and meta-analysis. Eur Urol. 2016;69:904–916. doi: 10.1016/j.eururo.2015.12.028. [DOI] [PubMed] [Google Scholar]
- 11.Mian R, Bodie JA, Soubra A, Lyon JA, Sultan S, Dahm P. Selective serotonin re-uptake inhibitors for premature ejaculation. Cochrane Database of Systematic Reviews. 2017 doi: 10.1002/14651858.CD012799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ahn TY, Park H, Choi EH, Choo MS, Park T. Fluoxetine as a treatment for premature ejaculation: a double-blind, randomized, placebo-controlled study. Korean J Urol. 1996;37:926–931. [Google Scholar]
- 13.Athanasios Z, Polyanthi P, George K. The efficacy of duloxetine in the treatment of premature ejaculation. Int Urol Nephrol. 2007;39:115–118. doi: 10.1007/s11255-006-6659-2. [DOI] [PubMed] [Google Scholar]
- 14.Atmaca M, Kuloglu M, Tezcan E, Semercioz A. The efficacy of citalopram in the treatment of premature ejaculation: a placebo-controlled study. Int J Impot Res. 2002;14:502–505. doi: 10.1038/sj.ijir.3900918. [DOI] [PubMed] [Google Scholar]
- 15.Biri H, Isen K, Sinik Z, Onaran M, Küpeli B, Bozkirli I. Sertraline in the treatment of premature ejaculation: a double-blind placebo controlled study. Int Urol Nephrol. 1998;30:611–615. doi: 10.1007/BF02550555. [DOI] [PubMed] [Google Scholar]
- 16.Buvat J, Tesfaye F, Rothman M, Rivas DA, Giuliano F. Dapoxetine for the treatment of premature ejaculation: results from a randomized, double-blind, placebo-controlled phase 3 trial in 22 countries. Eur Urol. 2009;55:957–967. doi: 10.1016/j.eururo.2009.01.025. [DOI] [PubMed] [Google Scholar]
- 17.Farnia V, Raisi F, Mohseni MG, Atharikia D, Ghafuri Z. On-demand treatment of premature ejaculation with citalopram: a randomized double-blind study. Acta Med Iran. 2009;47:353–355. [Google Scholar]
- 18.Gameel T, Tawfik A, Abou Farha M, Bastawisy M, Bendary M, Gamasy A. On-demand use of tramadol, sildenafil, paroxetine and local anaesthetics for the management of premature ejaculation: a randomized placebo-controlled clinical trial. J Sex Med. 2018;15(2 Suppl 1):S57. doi: 10.1016/j.aju.2013.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gameel TA, Tawfik AM, Abou-Farha MO, Bastawisy MG, El-Bendary MA, El-Gamasy Ael-N. On-demand use of tramadol, sildenafil, paroxetine and local anaesthetics for the management of premature ejaculation: a randomised placebo-controlled clinical trial. Arab J Urol. 2013;11:392–397. doi: 10.1016/j.aju.2013.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gameel TA, Tawfik AM, Soliman MG, El-Bendary MA, Abo-Elenen M, Tawfik TI, et al. On demand use of tramadol, sildenafil, paroxetine or local anesthetics for management of premature ejaculation, a randomized placebo-controlled clinical trial. Eur Urol Suppl. 2013;12:e214. doi: 10.1016/j.aju.2013.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gong ZY, Tang TL, Cui S, Wang JZ, Deng XZ. [Oral paroxetine for premature ejaculation: a randomized controlled study] Zhonghua Nan Ke Xue. 2011;17:923–925. Chinese. [PubMed] [Google Scholar]
- 22.Hamidi Madani A, Motiee R, Mokhtari G, Nasseh H, Esmaeili S, Kazemnezhad E. The efficiency and safety of tramadol, paroxetine and placebo in treatment of life long premature ejaculation. Eur Urol Suppl. 2016;15:e1001. [PMC free article] [PubMed] [Google Scholar]
- 23.Hamidi-Madani A, Motiee R, Mokhtari G, Nasseh H, Esmaeili S, Kazemnezhad E. The efficacy and safety of on-demand tramadol and paroxetine use in treatment of life long premature ejaculation: a randomized double-blind placebo-controlled clinical trial. J Reprod Infertil. 2018;19:10–15. [PMC free article] [PubMed] [Google Scholar]
- 24.Kara H, Aydin S, Yücel M, Agargün MY, Odabaş O, Yilmaz Y. The efficacy of fluoxetine in the treatment of premature ejaculation: a double-blind placebo controlled study. J Urol. 1996;156:1631–1632. [PubMed] [Google Scholar]
- 25.Kaufman JM, Rosen RC, Mudumbi RV, Tesfaye F, Hashmonay R, Rivas D. Treatment benefit of dapoxetine for premature ejaculation: results from a placebo-controlled phase III trial. BJU Int. 2009;103:651–658. doi: 10.1111/j.1464-410X.2008.08165.x. [DOI] [PubMed] [Google Scholar]
- 26.Khelaia A. Does still is a place for paroxetine in the era of dapoxetine. J Sex Med. 2015;12:214 [Google Scholar]
- 27.Khelaia A, Managadze L. Does still is a place for paroxetine in the era of dapoxetine. Andrology. 2014;2:100 [Google Scholar]
- 28.Khelaia AV, Bochorishvili GG, Managadze LG. Assessment of paroxetine in the treatment of premature ejaculation and dosage optimization. Eur Urol Suppl. 2012;11:e697–e697a. [Google Scholar]
- 29.Kim SC, Seo KK. Efficacy and safety of fluoxetine, sertraline and clomipramine in patients with premature ejaculation: a double-blind, placebo controlled study. J Urol. 1998;159:425–427. doi: 10.1016/s0022-5347(01)63940-5. [DOI] [PubMed] [Google Scholar]
- 30.Mattos RM, Marmo Lucon A, Srougi M. Tadalafil and fluoxetine in premature ejaculation: prospective, randomized, double-blind, placebo-controlled study. Urol Int. 2008;80:162–165. doi: 10.1159/000112607. [DOI] [PubMed] [Google Scholar]
- 31.McMahon CG. Treatment of premature ejaculation with sertraline hydrochloride: a single-blind placebo controlled crossover study. J Urol. 1998;159:1935–1938. doi: 10.1016/S0022-5347(01)63201-4. [DOI] [PubMed] [Google Scholar]
- 32.McMahon CG, Touma K. Treatment of premature ejaculation with paroxetine hydrochloride as needed: 2 single-blind placebo controlled crossover studies. J Urol. 1999;161:1826–1830. [PubMed] [Google Scholar]
- 33.McMahon C, Kim SW, Park NC, Chang CP, Rivas D, Tesfaye F, et al. Dapoxetine 3003 Study Investigators. Treatment of premature ejaculation in the Asia-Pacific region: results from a phase III double-blind, parallel-group study of dapoxetine. J Sex Med. 2010;7(1 Pt 1):256–268. doi: 10.1111/j.1743-6109.2009.01560.x. [DOI] [PubMed] [Google Scholar]
- 34.McMahon C, Park NC, Zhao Y, Rivas D, Rothman M. Treatment of premature ejaculation (PE) in the Asia-Pacific region: results from a phase III double-blind, parallel-group study of dapoxetine. Int J Urol. 2010;17 Suppl 1:A195. doi: 10.1111/j.1743-6109.2009.01560.x. [DOI] [PubMed] [Google Scholar]
- 35.McMahon CG, Giuliano F, Dean J, Hellstrom WJ, Bull S, Tesfaye F, et al. Efficacy and safety of dapoxetine in men with premature ejaculation and concomitant erectile dysfunction treated with a phosphodiesterase type 5 inhibitor: randomized, placebo-controlled, phase III study. J Sex Med. 2013;10:2312–2325. doi: 10.1111/jsm.12236. [DOI] [PubMed] [Google Scholar]
- 36.Mendels J, Camera A, Sikes C. Sertraline treatment for premature ejaculation. J Clin Psychopharmacol. 1995;15:341–346. doi: 10.1097/00004714-199510000-00006. [DOI] [PubMed] [Google Scholar]
- 37.Na KI, Kim JJ. Sertraline treatment in premature ejaculation: a double blind, randomized, placebo-controlled study. J Korean Androl Soc. 1996;14:101–104. [Google Scholar]
- 38.Novaretti JPT, Pompeo ACL, Arap S. Selective serotonin uptake inhibitor in the treatment of premature ejaculation. Braz J Urol. 2002;28:116–122. [Google Scholar]
- 39.Pryor JL, Althof SE, Steidle C, Rosen RC, Hellstrom WJ, Shabsigh R, et al. Dapoxetine Study Group. Efficacy and tolerability of dapoxetine in treatment of premature ejaculation: an integrated analysis of two double-blind, randomised controlled trials. Lancet. 2006;368:929–937. doi: 10.1016/S0140-6736(06)69373-2. [DOI] [PubMed] [Google Scholar]
- 40.Safarinejad MR. Comparison of dapoxetine versus paroxetine in patients with premature ejaculation: a double-blind, placebo-controlled, fixed-dose, randomized study. Clin Neuropharmacol. 2006;29:243–252. doi: 10.1097/01.WNF.0000228210.12194.46. [DOI] [PubMed] [Google Scholar]
- 41.Safarinejad MR. Safety and efficacy of escitalopram in the treatment of premature ejaculation: a double-blind, placebo-controlled, fixed-dose, randomized study. J Clin Psychopharmacol. 2007;27:444–450. doi: 10.1097/jcp.0b013e31814b98d4. [DOI] [PubMed] [Google Scholar]
- 42.Safarinejad MR. Safety and efficacy of dapoxetine in the treatment of premature ejaculation: a double-blind, placebo-controlled, fixed-dose, randomized study. Neuropsychopharmacology. 2008;33:1259–1265. doi: 10.1038/sj.npp.1301500. [DOI] [PubMed] [Google Scholar]
- 43.Safarinejad MR, Hosseini SY. Safety and efficacy of citalopram in the treatment of premature ejaculation: a double-blind placebo-controlled, fixed dose, randomized study. IJIR. 2006;18:164–169. doi: 10.1038/sj.ijir.3901384. [DOI] [PubMed] [Google Scholar]
- 44.Shang XJ, Geng Q, Zhang K, Xia XY, Shao Y, Huang YF. [Efficacy of citalopram on premature ejaculation: a clinical observation] Zhonghua Nan Ke Xue. 2012;18:1097–1100. Chinese. [PubMed] [Google Scholar]
- 45.Tuncel A, Aslan Y, Başar MM, Atan A. Efficacy of clomipramine, sertraline and terazosin treatments in premature ejaculation. Turk J Med Sci. 2008;38:59–64. [Google Scholar]
- 46.Waldinger MD, Hengeveld MW, Zwinderman AH. Paroxetine treatment of premature ejaculation: a double-blind, randomized, placebo-controlled study. Am J Psychiatry. 1994;151:1377–1379. doi: 10.1176/ajp.151.9.1377. [DOI] [PubMed] [Google Scholar]
- 47.Waldinger MD, Hengeveld MW, Zwinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol. 1998;18:274–281. doi: 10.1097/00004714-199808000-00004. [DOI] [PubMed] [Google Scholar]
- 48.Yilmaz U, Tatlişen A, Turan H, Arman F, Ekmekçioğlu O. The effects of fluoxetine on several neurophysiological variables in patients with premature ejaculation. J Urol. 1999;161:107–111. [PubMed] [Google Scholar]
- 49.Sathianathen NJ, Hwang EC, Mian R, Bodie JA, Soubra A, Lyon JA, et al. Selective serotonin re-uptake inhibitors for premature ejaculation in adult men. Cochrane Database Syst Rev. 2021;3:CD012799. doi: 10.1002/14651858.CD012799.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Sun Y, Yang L, Bao Y, Liu Z, Liu L, Wei Q. Efficacy of PDE5Is and SSRIs in men with premature ejaculation: a new systematic review and five meta-analyses. World J Urol. 2017;35:1817–1831. doi: 10.1007/s00345-017-2086-5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
PRISMA study flowchart.
Characteristics of included studies