

Abstract
Objective:
To determine if there is an association between total lipid intake, saturated fatty acid (SFA), Poly- and Mono-Unsaturated Fatty Acid (PUFA and MUFA) and cholesterol intake and breast cancer risk.
Materials and Methods:
We conducted a systematic review of the literature and a meta-analysis following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We included all cohort and case-control studies published up to December 2020 with subgroup analysis according to menopausal status.
Results:
We included 44 articles for analysis. There was no association between total fat, SFA, MUFA, PUFA and cholesterol intake and breast cancer in the general population and in pre-menopausal women. In postmenopausal women, high SFA consumption was associated with increased breast cancer risk in case-control studies [relative risk (RR): 1.12; confidence interval (CI) 95%: 1.03–1.21; p = 0.006 but not in cohort studies (RR: 1.01; CI 95%: 0.85–1.19; p = 0.93).
Conclusion:
There was a weak association between high SFA consumption and breast cancer risk in post-menopausal women, however there was high heterogeneity for this analysis. As lipids can have different actions in the same family, studies should rather focus on specific lipid consumption.
Keywords: Breast cancer risk, cholesterol, dietary fat intake, mono-unsaturated fatty acid, saturated fatty acid,
Key Points
• There was no association between total fat, saturated fatty-acids, mono and poly-unsaturated fatty acids and cholesterol intake and breast cancer incidence in the general population and in pre-menopausal women.
• There was a weak association between high saturated fatty acids consumption and breast cancer risk in post-menopausal women, but the results were heterogeneous.
Introduction
Among women, breast cancer is the most commonly diagnosed cancer and the leading cause of cancer-related mortality worldwide. It was estimated that in 2020 it represented over 2.2 million new cases (24.5% of all cancers) and caused over 680,000 deaths (15.5% of cancer-related deaths) (1). To date, different risk factors have been identified, some of which are potentially modifiable. Breast cancer is more commonly associated with age, environmental, hormonal and lifestyle factors than genetic factors ones (2). As it represents a major public health issue and both incidence and mortality will increase in the next decades (1), prevention focuses on acting on modifiable risk factors. Among lifestyle-related breast cancer risk factors, some are commonly accepted, including lack of physical activity (3) and overweight and obesity (4), while others are still controversial. Of interest, diet is known to play a role in the development of various cancers, such as colon cancer (5). Yet, in breast cancer the role of diet remains uncertain (2). Assessing the role of diet on breast cancer risk is complex, as diet varies between individuals, cultures and territories. Moreover, different evaluation methods exist, such as consumption of a particular food, a particular nutrient, or a particular pattern. For instance, the Mediterranean diet, dairy product consumption and fruit and vegetables intake seem to have a positive impact on reducing breast cancer incidence, while red meat consumption and alcohol intake seem to increase breast cancer risk (6). Similarly, organic food diet (7) and coffee consumption (8) seem to decrease breast cancer risk in postmenopausal women.
Commonly called “fats”, lipids are, along with proteins and carbohydrates, one of the three major families of macronutrients. Natural dietary lipids, which are essential in the diet for normal nutrition, include cholesterols and fatty acids. A distinction is made between saturated (SFA), mono-unsaturated (MUFA) and poly-unsaturated (PUFA) fatty acids. However, industrial fatty acids, which are mainly unsaturated trans fatty acids (TFA), seem to increase the risk of breast cancer (9). The role of natural lipids in carcinogenesis, and in particular their carcinogenic impact on the breast, has been suggested (10). Several studies and meta-analyses investigated the impact of dietary lipid intake and breast cancer incidence but the results are contradictory and inconclusive (11,12,14).
Our goal was therefore to attempt to determine, through a meta-analysis based on an updated literature review including cohort and case-control studies, whether there is an association not only between total lipid intake and breast cancer, but also to determine the specific role of SFA, PUFA, MUFA, and dietary cholesterol on breast cancer risk. In addition, we performed a subgroup analysis on menopausal status.
Materials and Methods
Search Strategy
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (15). A search was conducted on the MEDLINE database for articles published up to December 2020 and written in English, French or Spanish. The query included the following keywords: “fat intake”, “fatty acid”, “cholesterol”, “breast cancer risk”, “breast carcinoma”, “breast neoplasm”. The full query was: (“breast neoplasms”[MeSH Terms] OR (“breast”[All Fields] AND “neoplasms”[All Fields]) OR “breast neoplasms”[All Fields] OR (“breast”[All Fields] AND “cancer”[All Fields]) OR “breast cancer”[All Fields] OR (“breast neoplasms”[MeSH Terms] OR (“breast”[All Fields] AND “neoplasms”[All Fields]) OR “breast neoplasms”[All Fields] OR (“breast”[All Fields] AND “neoplasm”[All Fields]) OR “breast neoplasm”[All Fields]) OR (“breast”[All Fields] AND (“cancer s”[All Fields] OR “cancerated”[All Fields] OR “canceration”[All Fields] OR “cancerization”[All Fields] OR “cancerized”[All Fields] OR “cancerous”[All Fields] OR “neoplasms”[MeSH Terms] OR “neoplasms”[All Fields] OR “cancer”[All Fields] OR “cancers”[All Fields]) AND (“risk”[MeSH Terms] OR “risk”[All Fields]))) AND (“fatty acids”[MeSH Terms] OR (“fatty”[All Fields] AND “acids”[All Fields]) OR “fatty acids”[All Fields] OR (“fatty”[All Fields] AND “acid”[All Fields]) OR “fatty acid”[All Fields] OR (“fat”[All Fields] AND (“intake”[All Fields] OR “intake s”[All Fields] OR “intakes”[All Fields])) OR (“cholesterol”[MeSH Terms] OR “cholesterol”[All Fields] OR “cholesterol s”[All Fields] OR “cholesterol”[All Fields] OR “cholesterols”[All Fields])).
Eligibility Criteria
Prospective cohort or case-control studies were included if they met the following eligibility criteria:
• Population: pre- or post-menopausal women
• Exposure: high dietary intake of total fat, SFA, MUFA, PUFA, or cholesterol
• Comparator: low dietary intake of total fat, SFA, MUFA, PUFA, or cholesterol
• Outcome: risk increase of breast cancer
In addition, we included only articles where the population of each group was provided or could be precisely calculated. If more than one study involved the same population, only the most recent study or the one with the highest number of cases was included in the analysis.
Bibliographic Selection
The initial query gave 7,088 results. These articles were analyzed by two independent reviewers (M.L. and A.K.). Based on the title and abstract, 6,761 articles were excluded because they were not directly related to the subject under study, because of an unassessed association between breast cancer and dietary lipid intake, or because they were meta-analyses, correspondence, literature reviews, basic research articles, animal or in vitro studies. We retained 323 articles that were selected for full-text review. Among those, a further 279 articles were excluded because they did not investigate dietary intake of total fat, SFA, MUFA, PUFA or cholesterol and breast cancer risk, because no data was available in the published paper or because it was related to the same cohort of another included article. The final selection included 44 articles for the meta-analysis. Discrepancies between the two reviewers were resolved by consensus. The bibliographic selection, with exclusion reasons, is reported in the flow chart (Figure 1).
Figure 1.
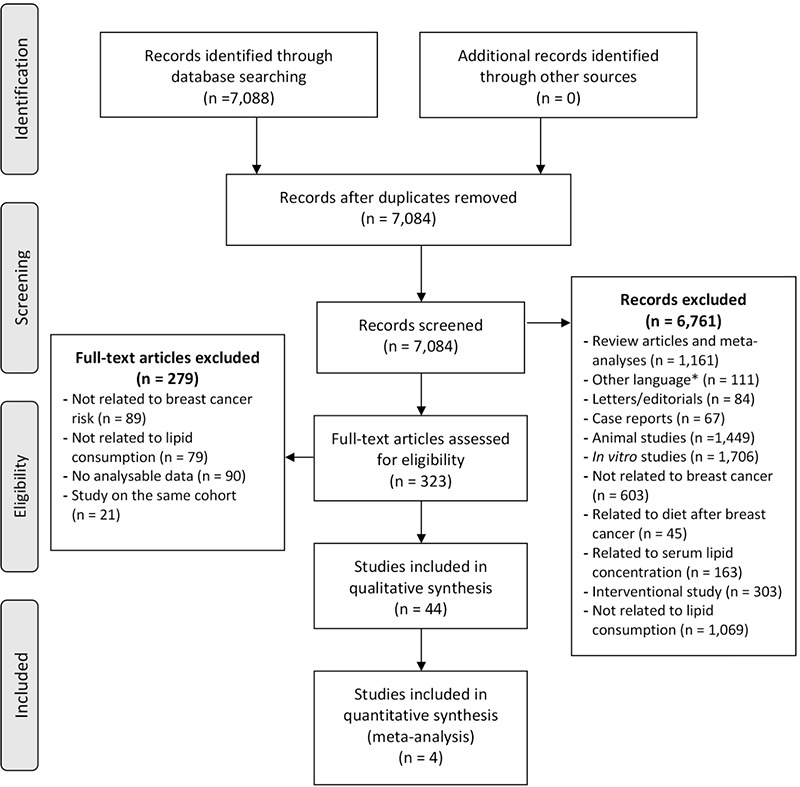
Flow chart diagram
n: number
Data Collection
For each article, one reviewer (AK) extracted the following information: first author name, year of publication, type of study (cohort or case-control), population studied (pre- or post-menopausal or both), the type of lipid (total fat, SFA, MUFA, PUFA, cholesterol) and the number of patients in each group (high versus low exposure, case and controls). In addition, country, years of inclusion, group constitution method (i.e., in two groups, in tertiles, quartiles, or quintiles), principal results and adjusting variables were retrieved. Verification of all these data was performed by the second reviewer (ML).
Statistical Analysis
For each article, we compared the group with the highest intake versus the group with the lowest. For instance, if patients were divided into five groups (quintiles), we compared the first with the fifth. The meta-analysis was performed using R (version: 3.6.1, 2019-07-05) (16) and with the metafor package (https://metafor-project.org/). Given the heterogeneity of the populations in the different studies, the random effect model was used in the meta-analysis. The articles were weighted on the standard error of each population, which in turn depended not only on the size of the cohort but also on its homogeneity. Summary relative risk (RR) was calculated with an estimated 95% confidence interval. Heterogeneity was quantified with a maximum-likelihood estimator for Tau2 and we calculated the Higgins’ I2 statistic. For the test of heterogeneity, the Cochran Q p-value was obtained with Wald-type test.
Results
Forty-four articles were included in the meta-analysis, consisting of 28 case-control studies (17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44) and 16 cohort studies (45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60). Results of each study are reported in Tables 1 and 2. In total, this meta-analysis involved 1,185,896 women, of whom 54,553 had breast cancer. Table 3 summarizes the pooled analysis results according to the studied population, lipids, and study type.
Table 1. Case-control studies.
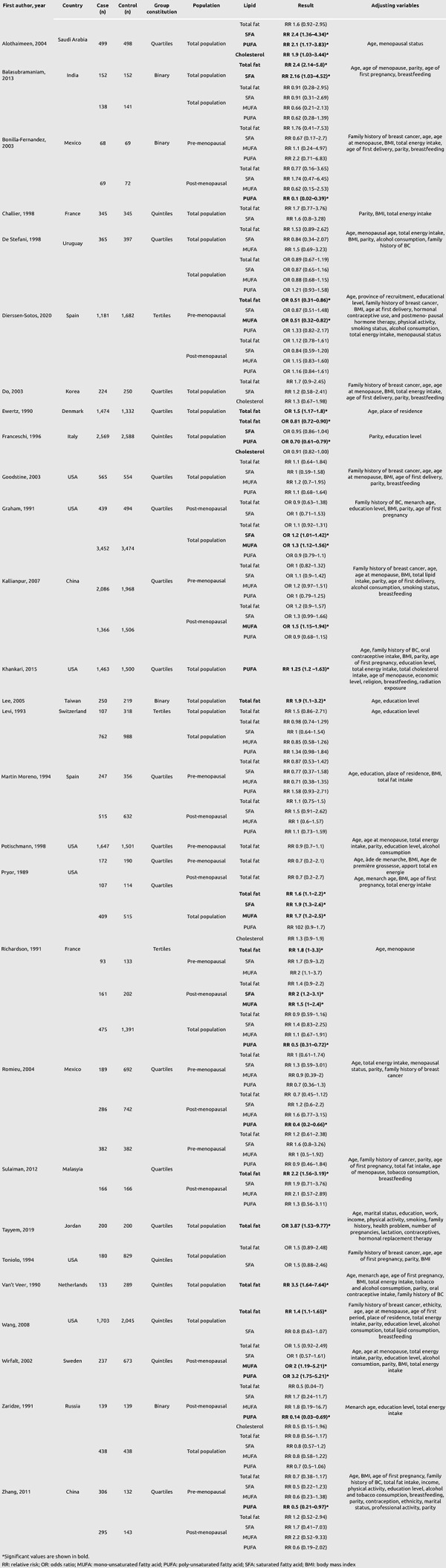
Table 2. Cohort studies.
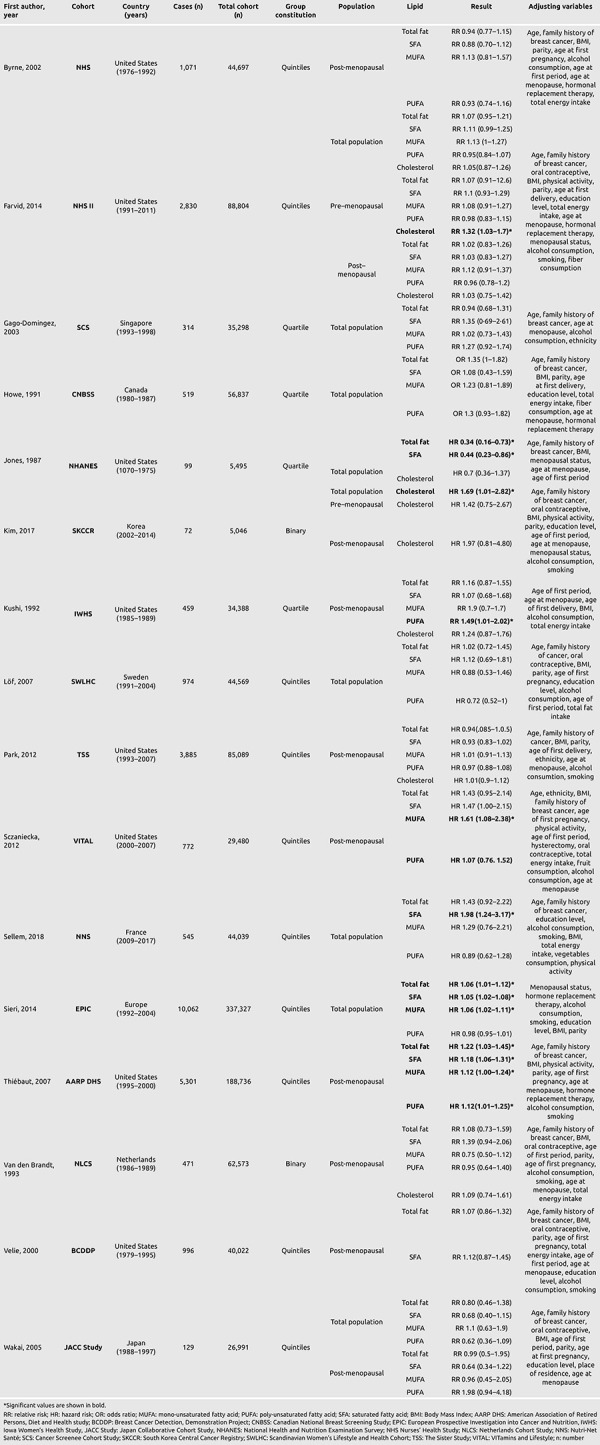
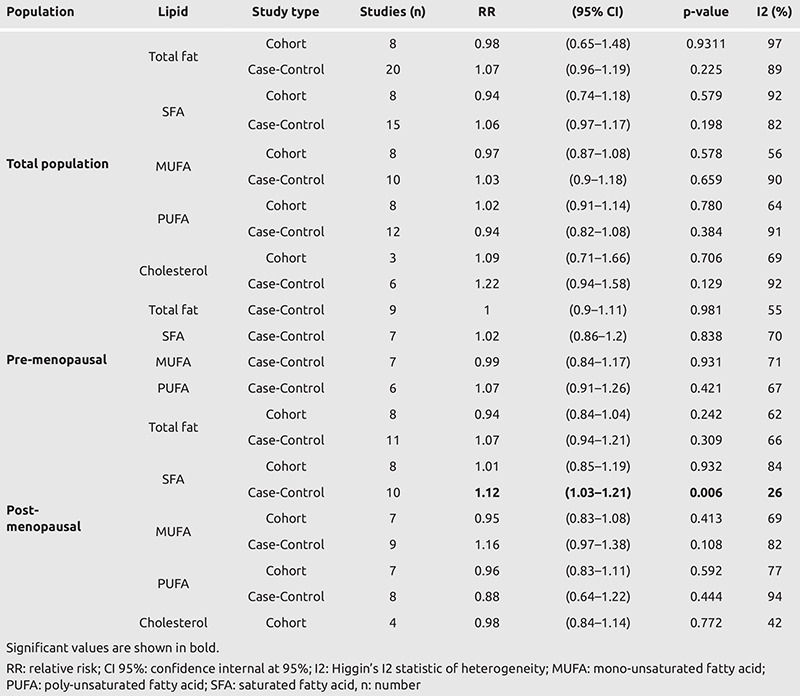
Table 3. Meta-analysis results.
Total Fat Intake
Total fat intake was evaluated in 27 case-control studies (96%) (17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 43, 44) and in 15 cohort studies (94%) (45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 59, 60). Ten studies (18, 19, 21, 36, 38, 39, 41, 43, 54, 57) found an increased risk of breast cancer with elevated total fat intake. Considering menopausal status, one study in pre-menopausal (21) and two in post-menopausal (39, 54) women found an increased risk of breast cancer. Conversely, two studies found a decreased risk with high fat intake diet (26, 44), and one of them among pre-menopausal women (44). The remaining studies did not find significant association between total fat intake and breast cancer.
In the pooled analysis, there was no significant risk increase in high total fat intake on breast cancer risk, neither for cohort [RR: 0.98; confidence interval (CI) 95%: 0.65–1.48; p = 0.93] nor case-control (RR: 1.07; CI 95% 0.96–1.19; p = 0.225) studies.
Considering menopausal status, no difference was found in pre-menopausal (RR: 1.0; CI 95%: 0.90–1.11; p = 0.98) women. In post-menopausal women both cohort and case-control pooled analysis were not significant giving relative risk results of RR: 0.94; CI 95%: 0.84 - 1.04; p = 0.24 and RR: 1.07; CI 95%: 0.94–1.21; p = 0.31, respectively.
Saturated Fatty Acids Consumption
SFA intake was evaluated in 20 case-control studies (71%) (20, 21, 22, 24, 25, 26, 27, 28, 30, 31, 32, 33, 34, 35, 37, 3839, 40, 41, 44) and in 15 cohort studies (94%) (45, 46, 47, 48, 49, 57, 59, 60). Seven studies (21, 34, 37, 41, 54, 57, 60) found an increased risk of breast cancer with elevated SFA consumption. Only one study found significant association in post-menopausal women (21). Conversely, one cohort study found a decreased risk with high SFA consumption, independently from menopausal status (45). The remaining studies did not find significant association between total fat intake and breast cancer.
In pooled analysis, there was no significant risk increase with high SFA consumption in breast cancer risk, whether it was for cohort (RR: 0.94; CI 95%: 0.74–1.18; p = 0.58) or case-control (RR: 1.06; CI 95%: 0.97: 1.17; p = 0.20) studies.
Concerning post-menopausal women (Figure 2), the pooled analysis case-control studies showed a significant increase in breast cancer risk (RR: 1.12; CI 95%: 1.03–1.21; p = 0.006) while it was not significant in cohort studies (RR: 1.01; CI 95%: 0.85–1.19; p = 0.93). No statistical difference was found in pre-menopausal women (RR: 1.02; CI 95%: 0.86–1.2; p = 0.84).
Figure 2.
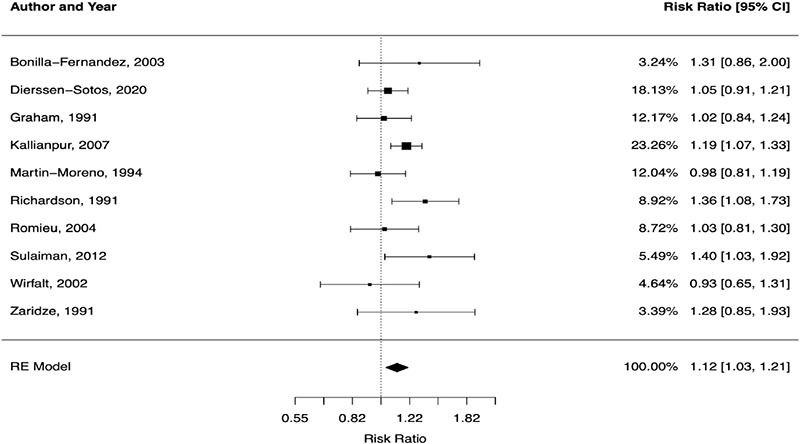
Forest plot of saturated fatty acids intake in case-control studies on post-menopausal women
CI: confidence interval
Unsaturated Fatty Acids Consumption
MUFA and PUFA consumption was evaluated in 15 case-control studies (54%) (21, 22, 24, 26, 28, 30, 31, 33, 34, 35, 37, 39, 40, 42, 44) and in 13 cohort studies (81%) (46, 47, 48, 50, 51,52, 53, 54, 55, 56, 57, 59, 60). Concerning PUFA, six articles found a decreased risk of breast cancer in women with elevated PUFA consumption (21, 22, 26, 31, 35, 40), among them one in pre-menopausal (40), and three in post-menopausal women (22, 31, 35). Conversely, five articles found an increased risk of breast cancer in women with elevated PUFA consumption (30, 34, 42, 47, 54), among them three in post-menopausal women (30, 47, 54). Concerning MUFA, six articles found an increased risk of breast cancer in women with elevated MUFA consumption (21, 30, 37, 54, 55, 57), among them four in post-menopausal women (30, 37, 54, 55). Conversely, one article found a decreased risk of breast cancer in pre-menopausal women with elevated MUFA consumption (44). The remaining studies did not find significant association between MUFA or PUFA consumption and breast cancer.
In pooled analysis there was no significant increased risk in high PUFA consumption on breast cancer risk, whether it was for cohort (RR: 1.02; CI 95%: 0.91–1.14; p = 0.78) or case-control (RR: 0.94; CI 95%: 0.82–1.08; p = 0.38) studies.
Considering menopausal status, no difference was found in pre-menopausal (RR: 1.07; CI 95%: 0.91–1.26; p = 0.42) women. In post-menopausal women both cohort and case-control pooled analysis were not significant (RR: 0.96; CI 95%. 0.83–1.11; p = 0.59 and RR: 0.88; CI 95%: 0.64–1.22; p = 0.44, respectively). Concerning MUFA, high consumption was not associated with increased breast cancer risk, whether it was for cohort (RR: 0.97; CI 95%: 0.87–1.08; p = 0.58) or case-control studies (RR: 1.03; CI 95%: 0.9–1.18; p = 0.66). No significant association was found in either pre-menopausal (RR: 0.99; CI 95%: 0.84–1.17; p = 0.93) or post-menopausal women, in either case-control studies (RR: 0.95; CI 95%: 0.83–1.08; p = 0.41) or cohort studies (RR: 1.16; CI 95%: 0.97–1.38; p = 0.11).
Cholesterol Consumption
Cholesterol consumption was evaluated in five case-control studies (18%) (21, 22, 26, 32, 34) and six cohort studies (43%) (45, 47, 48, 56, 58, 59). Three studies (34, 56, 58) found an increased risk of breast cancer with elevated cholesterol consumption, among them one found significant association in pre-menopausal women (56). None of the included studies found a decreased risk of breast cancer associated with high cholesterol consumption. The remaining studies did not find significant association between cholesterol consumption and breast cancer.
In pooled analysis there was no significant risk increase in high cholesterol consumption on breast cancer risk, whether it was for cohort (RR: 1.09; CI 95%: 0.71–1.61; p = 0.71) or case-control (RR: 1.22; CI 95%: 0.94–1.58; p = 0.13) studies.
Furthermore, no difference was found in post-menopausal women (RR: 0.98; CI 95%: 0.84–1.14; p = 0.772).
Discussion
The results of this meta-analysis does not demonstrate a statistically significant link between high consumption of total lipids, PUFA, MUFA and cholesterol and the occurrence of breast cancer. However, our results suggest that there is an association between SFA intake and breast cancer risk in postmenopausal women, although this was only found in case-controlled studies and not cohort studies. Nevertheless, it is necessary to underline the great heterogeneity in this meta-analysis. Lipid consumption may therefore play a role in breast health. Interestingly, another meta-analysis published in 2015 found a significant association between high SFA consumption and breast cancer risk among post-menopausal women, and the authors found this association only in case-control studies and not in cohort studies (61). These results are consistent with other previously published articles (62, 63). We investigated if high lipid consumption may act on breast tissue by the same mechanisms as obesity or if there were other underlying explanations.
Role of Obesity in Breast Carcinogenesis
Obesity, a documented breast cancer risk factor after menopause (4), is directly related to physical activity and diet (64). Mechanisms underlying the increased risk of breast cancer related to overweight and obesity are becoming better known and seem to rely largely on metabolic changes related to the endocrine action of excessive adipose tissue. These are mainly due to changes in steroid hormone metabolism as well as the action of inflammatory mediators (64). Mechanisms involving steroid hormones are the predominant hypothesis to explain the associations between obesity and breast cancer. The two main sites of estrogen synthesis are the ovaries before menopause, and adipose tissue through aromatization of adrenal androgen and ovarian androgens after menopause (65). Once released, estrogens act on breast epithelial cells and as a promoter of cell proliferation and this leads to an increased risk of mutation and malignant transformation of breast cells (65). This partly explains the increased risk of breast cancer after menopause in overweight or obese women. However, adipocytes, which are present in large numbers in breast tissue, secrete a range of adipokines/cytokines. Two of the cytokines are leptin and adiponectin. Leptin is a pro-inflammatory cytokine that causes post-prandial satiety and activation of cell proliferation. Adiponectin has an anti-inflammatory and antineoplastic action (66). These two cytokines balance each other in normal body weight, but in obese people there is a loss of this balance. and the production of pro-inflammatory cytokines is promoted. Clinical and experimental studies (67, 68), have found a deleterious link between adipocytes present at the tumor invasion front and the progression of breast cancer (69, 70). Breast adipocytes are involved in tumor initiation, proliferation, progression and metastasis (66). Adipocytes now appear to be important cellular contributors to tumor progression. Taken together, these biological mechanisms may explain how obesity increases breast cancer risk.
Lipid Consumption Is Not Directly Linked to Obesity
However, diet and obesity may not have an effect on the breast through the same mechanisms. Indeed, lipid consumption is not directly related to obesity and overweight. There is evidence that high total energy intake (71) and high carbohydrate intake (72) are directly related to weight gain. The link between obesity and higher fat consumption without an increase in total energy consumption is still debated. Surprisingly, epidemiological studies do not demonstrate the role of high lipid intake in the occurrence of obesity, beyond their contribution to making the energy balance positive. In the European Prospective Investigation into Cancer and Nutrition (EPIC) prospective study of over 89,000 subjects with mean lipid intakes of 31.5%–36.5% of total energy intake, dietary lipids were not associated with weight change (73). In addition, weight gain appears to be independent of the percentage of total fat consumed (74) and there is no evidence that overweight subjects ingest more lipids than others (75). Therefore, there must be other biological explanations for our findings.
Specificity and Action of Different Lipid Subtypes
The role of the different classes of fatty acids in breast carcinogenesis has been the subject of numerous studies, mainly based on animal models. In these models, high lipid intake (40% of ingested energy) stimulated mammary carcinogenesis with a dose-effect, independent from the nature of the lipids that made up the diet (76).
We found that high SFA consumption may increase breast cancer risk among post-menopausal women. However, biological mechanisms linking SFA and breast cancerogenesis are still unknown. In vitro studies on a breast cancer cell line (MDA-MB-231) found that SFA stimulated proliferation while unsaturated fatty acids inhibited proliferation and induced apoptosis (77). Still, a possible explanation would be that SFA intake increased insulin resistance and may therefore lead to an increased breast cancer risk (78). However, results of our meta-analysis do not show a significant impact of PUFA, MUFA and cholesterol consumption on breast cancer risk. Unlike SFA, MUFA derived from olive oil reduced insulin resistance and therefore had a benefit on breast cancer risk (79). However, this was not found for non-vegetable MUFA. Results from the E3N-EPIC study found that high plasma levels of natural MUFA were not associated with an increased breast cancer risk while there was an increased risk for trans-mono-saturated fatty acids (9).
PUFA may reduce the binding between estrogen and serum proteins, including sex-hormone binding globulin (SHBG) and albumin, thereby increasing the circulating level of biologically potent estrogens that can activate breast cell growth (76). Long-chain PUFA such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) can inhibit the production of arachidonic acid-derived eicosanoids in tumors (80). Lipid peroxidation can induce apoptosis (81, 82). The n-3 PUFA can therefore bind and activate the peroxisome proliferator-activated gamma receptor, leading to activation of the proteoglycan syndecan-1 in human breast cancer cells, thereby inducing apoptosis and inhibition of cell growth (80). Linoleic acid can generate 13-hydroxylinoleic acid, which enhances the growth-stimulating signal of peptide growth factors, such as epidermal growth factor (EGF) and insulin, which may stimulate the growth of cancer cells (83). A meta-analysis found that high plasma levels of n-3 PUFA were associated with a decreased risk of breast cancer (84). Conversely, high levels of MUFA and SFA (palmitic and oleic acids) were associated with increased breast cancer risk (84).
High blood cholesterol levels appear to increase the risk of breast cancer (85). Interventional studies in mice have highlighted the role of cholesterol in mammary tumor cells (86). Some derivatives such as 6-oxo-cholestan-3b,5a-diol (OCDO) and 27-hydroxycholesterol (27HC) are involved in the promotion, proliferation and migration of cancer cells (87, 88). To date, it is not confirmed that high dietary cholesterol intake is a risk factor for breast cancer, as shown in our meta-analysis and other articles (89, 90). This may be explained in part by the low proportion of cholesterol (about 30%) in the diet, while the rest comes from the degradation of lipids and carbohydrates by the liver (91).
Limitations of Our Study
It is important to consider certain elements that may have led to sources of bias in our results in view of the great heterogeneity of the selected studies. In fact, the studies included in our meta-analysis were carried out on populations from five continents with significant cultural and dietary diversity. The types of oils used in the diet also vary from one country to another, with a particular consumption of olive oil around the Mediterranean rim, as for example in Italy (26) or Spain (24), which is one of the main sources of MUFA. Conversely, in the United States and Canada, MUFA are largely provided by products of animal origin (46, 55). In Asian countries such as China, Korea, Japan and Singapore, women have a diet that is predominantly vegetarian or with low meat content (40, 51, 52). Moreover, each lipid family (SFA, MUFA, PUFA) contains a broad range of lipids. As previously described, effects may differ even among the same family. Consequently, it is possible that our results do not reflect the effect of a particular lipid, which may be specifically implicated in breast carcinogenesis.
In addition, methods of data collection, which differed across studies, must be considered when explaining the differences in outcomes between cohort and case-control studies. Case-control studies are subject to a recall bias, as dietary habits were collected with a questionnaire after the onset of the disease. Conversely, the results of cohort surveys are considered more conclusive because they are based on the collection of dietary habits in healthy subjects at the beginning of the studies and have a prospective setting. Moreover, cohort studies have a higher number of patients and a longer duration of follow-up (up to 20 years) and therefore higher statistical power.
Finally, our results were adjusted according to menopausal status but not with other variables, as data was not available for the meta-analysis. In the different studies, relative risks and odds ratio were adjusted with different variables such as body mass index, age, and parity. These variables are reported in Tables 1 and 2.
Conclusion
Despite the heterogeneity of the included articles, follow-up durations, populations and number of patients, most studies are consistent with respect to total lipids, MUFA, PUFA and cholesterol. Nevertheless, an association was found between high intake of SFA and the occurrence of breast cancer in post-menopausal women for case-controlled studies but not for cohort studies, requiring additional investigation. These studies should focus more on the type of SFA rather than the whole lipid family, as each lipid intake may have specific consequences.
At this stage, therefore, it is not possible to establish nutritional recommendations regarding the consumption of lipids to decrease breast cancer risk. However, even if lipid intake does not play a significant role in the etiology of breast cancer, its proven adverse effect on pathologies, such as cardiovascular disease, justifies the consolidation of nutritional education efforts.
Moreover, adipocytes have a role in promoting and regulating breast cancer. Current studies are of interest (87, 92) and contribute to an understanding of biochemical mechanisms. The discovery of new molecules with anti-tumor properties, such as dendrogenin A (DDA), a natural cholesterol derivative (87), opens doors to the development of new therapeutics.
Acknowledgments
The authors are thankful to the patient association Seins et Vie (SEVE) for the help and support.
Footnotes
Ethics Committee Approval: Not applicable.
Informed Consent: Not applicable.
Peer-review: Externally peer-reviewed.
Authorship Contributions
Concept: F.L.Q., C.M.; Design: M.L., C.M.; Data Collection and/or Processing: M.L., A.K., F.L.Q.; Analysis and/or Interpretation: M.L., V.G., C.T.; Literature Search: M.L., A.K., F.L.Q.; Writing: M.L., A.K., F.L.Q., V.G., C.T., C.M.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study received no financial support.
References
- 1.Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available at: accessed [24/01/2021]. 2020. [Internet] https://gco.iarc.fr/today.
- 2.Rojas K, Stuckey A. Breast Cancer Epidemiology and Risk Factors. Clin Obstet Gynecol. 2016;59:651–672. doi: 10.1097/GRF.0000000000000239. [DOI] [PubMed] [Google Scholar]
- 3.Thune I, Brenn T, Lund E, Gaard M. Physical activity and the risk of breast cancer. N Engl J Med. 1997;336:1269–1275. doi: 10.1056/NEJM199705013361801. [DOI] [PubMed] [Google Scholar]
- 4.Arnold M, Pandeya N, Byrnes G, Renehan PAG, Stevens GA, Ezzati PM, et al. Global burden of cancer attributable to high body-mass index in 2012: a population-based study. Lancet Oncol. 2015;16:36–46. doi: 10.1016/S1470-2045(14)71123-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Howe GR, Aronson KJ, Benito E, Castelleto R, Cornée J, Duffy S, et al. The relationship between dietary fat intake and risk of colorectal cancer: evidence from the combined analysis of 13 case-control studies. Cancer Causes Control. 1997;8:215–228. doi: 10.1023/a:1018476414781. [DOI] [PubMed] [Google Scholar]
- 6.De Cicco P, Catani MV, Gasperi V, Sibilano M, Quaglietta M, Savini I. Nutrition and Breast Cancer: A Literature Review on Prevention, Treatment and Recurrence. Nutrients. 2019;11:1514. doi: 10.3390/nu11071514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Baudry J, Assmann KE, Touvier M, Allès B, Seconda L, Latino-Martel P, et al. Association of Frequency of Organic Food Consumption With Cancer Risk: Findings From the NutriNet-Santé Prospective Cohort Study. JAMA Intern Med. 2018;178:1597–1606. doi: 10.1001/jamainternmed.2018.4357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nehlig A, Reix N, Arbogast P, Mathelin C. Coffee consumption and breast cancer risk: a narrative review in the general population and in different subtypes of breast cancer. Eur J Nutr. 2021;60:1197–1235. doi: 10.1007/s00394-020-02465-0. [DOI] [PubMed] [Google Scholar]
- 9.Chajès V, Thiébaut AC, Rotival M, Gauthier E, Maillard V, Boutron-Ruault MC, et al. Association between serum trans-monounsaturated fatty acids and breast cancer risk in the E3N-EPIC Study. Am J Epidemiol. 2008;167:1312–1320. doi: 10.1093/aje/kwn069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cowen S, McLaughlin SL, Hobbs G, Coad J, Martin KH, Olfert IM, et al. High-Fat, High-Calorie Diet Enhances Mammary Carcinogenesis and Local Inflammation in MMTV-PyMT Mouse Model of Breast Cancer. Cancers (Basel) 2015;7:1125–1142. doi: 10.3390/cancers7030828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cao Y, Hou L, Wang W. Dietary total fat and fatty acids intake, serum fatty acids and risk of breast cancer: A meta-analysis of prospective cohort studies. Int J Cancer. 2016;138:1894–1904. doi: 10.1002/ijc.29938. [DOI] [PubMed] [Google Scholar]
- 12.Hunter DJ, Spiegelman D, Adami HO, Beeson L, van den Brandt PA, Folsom AR, et al. Cohort studies of fat intake and the risk of breast cancer--a pooled analysis. N Engl J Med. 1996;334:356–361. doi: 10.1056/NEJM199602083340603. [DOI] [PubMed] [Google Scholar]
- 13.Boyd NF, Martin LJ, Noffel M, Lockwood GA, Trichler DL. A meta-analysis of studies of dietary fat and breast cancer risk. Br J Cancer. 1993;68:627–636. doi: 10.1038/bjc.1993.398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dandamudi A, Tommie J, Nommsen-Rivers L, Couch S. Dietary Patterns and Breast Cancer Risk: A Systematic Review. Anticancer Res. 2018;38:3209–3222. doi: 10.21873/anticanres.12586. [DOI] [PubMed] [Google Scholar]
- 15.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8:336–431. doi: 10.1016/j.ijsu.2010.02.007. [DOI] [PubMed] [Google Scholar]
- 16.R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; 2019. [Internet] http://lib.stat.cmu.edu/R/CRAN/doc/manuals/r-devel/fullrefman.pdf.
- 17.Pryor M, Slattery ML, Robison LM, Egger M. Adolescent diet and breast cancer in Utah. Cancer Res. 1989;49:2161–2167. [PubMed] [Google Scholar]
- 18.Ewertz M, Gill C. Dietary factors and breast-cancer risk in Denmark. Int J Cancer. 1990;46:779–784. doi: 10.1002/ijc.2910460505. [DOI] [PubMed] [Google Scholar]
- 19.Van’t Veer P, Kok FJ, Brants HA, Ockhuizen T, Sturmans F, Hermus RJ. Dietary fat and the risk of breast cancer. Int J Epidemiol. 1990;19:12–18. doi: 10.1093/ije/19.1.12. [DOI] [PubMed] [Google Scholar]
- 20.Graham S, Hellmann R, Marshall J, Freudenheim J, Vena J, Swanson M, et al. Nutritional epidemiology of postmenopausal breast cancer in western New York. Am J Epidemiol. 1991;134:552–566. doi: 10.1093/oxfordjournals.aje.a116129. [DOI] [PubMed] [Google Scholar]
- 21.Richardson S, Gerber M, Cenee S. The role of fat, animal protein and some vitamin consumption in breast cancer: a case control study in southern France. Int J Cancer. 1991;48:1–9. doi: 10.1002/ijc.2910480102. [DOI] [PubMed] [Google Scholar]
- 22.Zaridze D, Lifanova Y, Maximovitch D, Day NE, Duffy SW. Diet, alcohol consumption and reproductive factors in a case-control study of breast cancer in Moscow. Int J Cancer. 1991;48:493–501. doi: 10.1002/ijc.2910480404. [DOI] [PubMed] [Google Scholar]
- 23.Levi F, La Vecchia C, Gulie C, Negri E. Dietary factors and breast cancer risk in Vaud, Switzerland. Nutr Cancer. 1993;19:327–335. doi: 10.1080/01635589309514263. [DOI] [PubMed] [Google Scholar]
- 24.Martin-Moreno JM, Willett WC, Gorgojo L, Banegas JR, Rodriguez-Artalejo F, Fernandez-Rodriguez JC, et al. Dietary fat, olive oil intake and breast cancer risk. Int J Cancer. 1994;58:774–780. doi: 10.1002/ijc.2910580604. [DOI] [PubMed] [Google Scholar]
- 25.Toniolo P, Riboli E, Shore RE, Pasternack BS. Consumption of meat, animal products, protein, and fat and risk of breast cancer: a prospective cohort study in New York. Epidemiology. 1994;5:391–397. doi: 10.1097/00001648-199407000-00003. [DOI] [PubMed] [Google Scholar]
- 26.Franceschi S, Favero A, Decarli A, Negri E, La Vecchia C, Ferraroni M, et al. Intake of macronutrients and risk of breast cancer. Lancet. 1996;347:1351–1356. doi: 10.1016/s0140-6736(96)91008-9. [DOI] [PubMed] [Google Scholar]
- 27.Challier B, Perarnau JM, Viel JF. Garlic, onion and cereal fibre as protective factors for breast cancer: a French case-control study. Eur J Epidemiol. 1998;14:737–747. doi: 10.1023/a:1007512825851. [DOI] [PubMed] [Google Scholar]
- 28.De Stefani E, Deneo-Pellegrini H, Mendilaharsu M, Ronco A. Essential fatty acids and breast cancer: a case-control study in Uruguay. Int J Cancer. 1998;76:491–494. doi: 10.1002/(sici)1097-0215(19980518)76:4<491::aid-ijc8>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 29.Potischman N, Weiss HA, Swanson CA, Coates RJ, Gammon MD, Malone KE, et al. Diet during adolescence and risk of breast cancer among young women. J Natl Cancer Inst. 1998;90:226–233. doi: 10.1093/jnci/90.3.226. [DOI] [PubMed] [Google Scholar]
- 30.Wirfält E, Mattisson I, Gullberg B, Johansson U, Olsson H, Berglund G. Postmenopausal breast cancer is associated with high intakes of omega6 fatty acids (Sweden) Cancer Causes Control. 2002;13:883–893. doi: 10.1023/a:1021922917489. [DOI] [PubMed] [Google Scholar]
- 31.Bonilla-Fernández P, López-Cervantes M, Torres-Sánchez LE, Tortolero-Luna G, López-Carrillo L. Nutritional factors and breast cancer in Mexico. Nutr Cancer. 2003;45:148–155. doi: 10.1207/S15327914NC4502_02. [DOI] [PubMed] [Google Scholar]
- 32.Do MH, Lee SS, Jung PJ, Lee MH. Intake of dietary fat and vitamin in relation to breast cancer risk in Korean women: a case-control study. J Korean Med Sci. 2003;18:534–540. doi: 10.3346/jkms.2003.18.4.534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Goodstine SL, Zheng T, Holford TR, Ward BA, Carter D, Owens PH, et al. Dietary (n-3)/(n-6) fatty acid ratio: possible relationship to premenopausal but not postmenopausal breast cancer risk in U.S. women. J Nutr. 2003;133:1409–1414. doi: 10.1093/jn/133.5.1409. [DOI] [PubMed] [Google Scholar]
- 34.Alothaimeen A, Ezzat A, Mohamed G, Muammar T, Al-Madouj A. Dietary fat and breast cancer in Saudi Arabia: a case-control study. East Mediterr Health J. 2004;10:879–886. [PubMed] [Google Scholar]
- 35.Romieu I, Lazcano-Ponce E, Sanchez-Zamorano LM, Willett W, Hernandez-Avila M. Carbohydrates and the risk of breast cancer among Mexican women. Cancer Epidemiol Biomarkers Prev. 2004;13:1283–1289. [PubMed] [Google Scholar]
- 36.Lee MM, Chang IY, Horng CF, Chang JS, Cheng SH, Huang A. Breast cancer and dietary factors in Taiwanese women. Cancer Causes Control. 2005;16:929–937. doi: 10.1007/s10552-005-4932-9. [DOI] [PubMed] [Google Scholar]
- 37.Kallianpur AR, Lee SA, Gao YT, Lu W, Zheng Y, Ruan ZX, et al. Dietary animal-derived iron and fat intake and breast cancer risk in the Shanghai Breast Cancer Study. Breast Cancer Res Treat. 2008;107:123–132. doi: 10.1007/s10549-007-9538-3. [DOI] [PubMed] [Google Scholar]
- 38.Wang J, John EM, Horn-Ross PL, Ingles SA. Dietary fat, cooking fat, and breast cancer risk in a multiethnic population. Nutr Cancer. 2008;60:492–504. doi: 10.1080/01635580801956485. [DOI] [PubMed] [Google Scholar]
- 39.Sulaiman S, Shahril MR, Shaharudin SH, Emran NA, Muhammad R, Ismail F, et al. Fat intake and its relationship with pre- and post-menopausal breast cancer risk: a case-control study in Malaysia. Asian Pac J Cancer Prev. 2011;12:2167–2178. [PubMed] [Google Scholar]
- 40.Zhang CX, Ho SC, Lin FY, Chen YM, Cheng SZ, Fu JH. Dietary fat intake and risk of breast cancer: a case-control study in China. Eur J Cancer Prev. 2011;20:199–206. doi: 10.1097/CEJ.0b013e32834572bb. [DOI] [PubMed] [Google Scholar]
- 41.Balasubramaniam SM, Rotti SB, Vivekanandam S. Risk factors of female breast carcinoma: a case control study at Puducherry. Indian J Cancer. 2013;50:65–70. doi: 10.4103/0019-509X.112307. [DOI] [PubMed] [Google Scholar]
- 42.Khankari NK, Bradshaw PT, Steck SE, He K, Olshan AF, Shen J, et al. Polyunsaturated fatty acid interactions and breast cancer incidence: a population-based case-control study on Long Island, New York. Ann Epidemiol. 2015;25:929–935. doi: 10.1016/j.annepidem.2015.09.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tayyem RF, Mahmoud RI, Shareef MH, Marei LS. Nutrient intake patterns and breast cancer risk among Jordanian women: a case-control study. Epidemiol Health. 2019;41:e2019010. doi: 10.4178/epih.e2019010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Dierssen-Sotos T, Gómez-Acebo I, Palazuelos C, Gracia-Lavedan E, Pérez-Gómez B, Oribe M, et al. Fatty acid intake and breast cancer in the Spanish multicase-control study on cancer (MCC-Spain) Eur J Nutr. 2020;59:1171–1179. doi: 10.1007/s00394-019-01977-8. [DOI] [PubMed] [Google Scholar]
- 45.Jones DY, Schatzkin A, Green SB, Block G, Brinton LA, Ziegler RG, et al. Dietary fat and breast cancer in the National Health and Nutrition Examination Survey I Epidemiologic Follow-up Study. J Natl Cancer Inst. 1987;79:465–471. [PubMed] [Google Scholar]
- 46.Howe GR, Friedenreich CM, Jain M, Miller AB. A cohort study of fat intake and risk of breast cancer. J Natl Cancer Inst. 1991;83:336–340. doi: 10.1093/jnci/83.5.336. [DOI] [PubMed] [Google Scholar]
- 47.Kushi LH, Sellers TA, Potter JD, Nelson CL, Munger RG, Kaye SA, et al. Dietary fat and postmenopausal breast cancer. J Natl Cancer Inst. 1992;84:1092–1099. doi: 10.1093/jnci/84.14.1092. [DOI] [PubMed] [Google Scholar]
- 48.van den Brandt PA, van’t Veer P, Goldbohm RA, Dorant E, Volovics A, Hermus RJ, et al. A prospective cohort study on dietary fat and the risk of postmenopausal breast cancer. Cancer Res. 1993;53:75–82. [PubMed] [Google Scholar]
- 49.Velie E, Kulldorff M, Schairer C, Block G, Albanes D, Schatzkin A. Dietary fat, fat subtypes, and breast cancer in postmenopausal women: a prospective cohort study. J Natl Cancer Inst. 2000;92:833–839. doi: 10.1093/jnci/92.10.833. [DOI] [PubMed] [Google Scholar]
- 50.Byrne C, Rockett H, Holmes MD. Dietary fat, fat subtypes, and breast cancer risk: lack of an association among postmenopausal women with no history of benign breast disease. Cancer Epidemiol Biomarkers Prev. 2002;11:261–265. [PubMed] [Google Scholar]
- 51.Gago-Dominguez M, Yuan JM, Sun CL, Lee HP, Yu MC. Opposing effects of dietary n-3 and n-6 fatty acids on mammary carcinogenesis: The Singapore Chinese Health Study. Br J Cancer. 2003;89:1686–1692. doi: 10.1038/sj.bjc.6601340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Wakai K, Tamakoshi K, Date C, Fukui M, Suzuki S, Lin Y, et al. Dietary intakes of fat and fatty acids and risk of breast cancer: a prospective study in Japan. Cancer Sci. 2005;96:590–599. doi: 10.1111/j.1349-7006.2005.00084.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Löf M, Sandin S, Lagiou P, Hilakivi-Clarke L, Trichopoulos D, Adami HO, et al. Dietary fat and breast cancer risk in the Swedish women’s lifestyle and health cohort. Br J Cancer. 2007;97:1570–1576. doi: 10.1038/sj.bjc.6604033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Thiébaut AC, Chajès V, Gerber M, Boutron-Ruault MC, Joulin V, Lenoir G, et al. Dietary intakes of omega-6 and omega-3 polyunsaturated fatty acids and the risk of breast cancer. Int J Cancer. 2009;124:924–931. doi: 10.1002/ijc.23980. [DOI] [PubMed] [Google Scholar]
- 55.Sczaniecka AK, Brasky TM, Lampe JW, Patterson RE, White E. Dietary intake of specific fatty acids and breast cancer risk among postmenopausal women in the VITAL cohort. Nutr Cancer. 2012;64:1131–1142. doi: 10.1080/01635581.2012.718033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Farvid MS, Cho E, Chen WY, Eliassen AH, Willett WC. Premenopausal dietary fat in relation to pre- and post-menopausal breast cancer. Breast Cancer Res Treat. 2014;145:255–265. doi: 10.1007/s10549-014-2895-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Sieri S, Chiodini P, Agnoli C, Pala V, Berrino F, Trichopoulou A, et al. Dietary fat intake and development of specific breast cancer subtypes. J Natl Cancer Inst. 2014;106:dju068. doi: 10.1093/jnci/dju068. [DOI] [PubMed] [Google Scholar]
- 58.Kim JH, Lee J, Jung SY, Kim J. Dietary Factors and Female Breast Cancer Risk: A Prospective Cohort Study. Nutrients. 2017;9:1331. doi: 10.3390/nu9121331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Park YM, White AJ, Nichols HB, O’Brien KM, Weinberg CR, Sandler DP. The association between metabolic health, obesity phenotype and the risk of breast cancer. Int J Cancer. 2017;140:2657–2666. doi: 10.1002/ijc.30684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Sellem L, Srour B, Guéraud F, Pierre F, Kesse-Guyot E, Fiolet T, et al. Saturated, mono- and polyunsaturated fatty acid intake and cancer risk: results from the French prospective cohort NutriNet-Santé. Eur J Nutr. 2019;58:1515–1527. doi: 10.1007/s00394-018-1682-5. [DOI] [PubMed] [Google Scholar]
- 61.Xia H, Ma S, Wang S, Sun G. Meta-Analysis of Saturated Fatty Acid Intake and Breast Cancer Risk. Medicine (Baltimore) 2015;94:e2391. doi: 10.1097/MD.0000000000002391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Smith-Warner SA, Spiegelman D, Adami HO, Beeson WL, van den Brandt PA, Folsom AR, et al. Types of dietary fat and breast cancer: a pooled analysis of cohort studies. Int J Cancer. 2001;92:767–774. doi: 10.1002/1097-0215(20010601)92:5<767::aid-ijc1247>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 63.Boyd NF, Stone J, Vogt KN, Connelly BS, Martin LJ, Minkin S. Dietary fat and breast cancer risk revisited: a meta-analysis of the published literature. Br J Cancer. 2003;89:1672–1685. doi: 10.1038/sj.bjc.6601314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 2008;371:569–578. doi: 10.1016/S0140-6736(08)60269-X. [DOI] [PubMed] [Google Scholar]
- 65.Travis RC, Key TJ. Oestrogen exposure and breast cancer risk. Breast Cancer Res. 2003;5:239–247. doi: 10.1186/bcr628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Renehan AG, Zwahlen M, Egger M. Adiposity and cancer risk: new mechanistic insights from epidemiology. Nat Rev Cancer. 2015;15:484–498. doi: 10.1038/nrc3967. [DOI] [PubMed] [Google Scholar]
- 67.Andarawewa KL, Boulay A, Masson R, Mathelin C, Stoll I, Tomasetto C, et al. Dual stromelysin-3 function during natural mouse mammary tumor virus-ras tumor progression. Cancer Res. 2003;63:5844–5849. [PubMed] [Google Scholar]
- 68.Dirat B, Bochet L, Dabek M, Daviaud D, Dauvillier S, Majed B, et al. Cancer-associated adipocytes exhibit an activated phenotype and contribute to breast cancer invasion. Cancer Res. 2011;71:2455–2465. doi: 10.1158/0008-5472.CAN-10-3323. [DOI] [PubMed] [Google Scholar]
- 69.Wang YY, Lehuédé C, Laurent V, Dirat B, Dauvillier S, Bochet L, et al. Adipose tissue and breast epithelial cells: a dangerous dynamic duo in breast cancer. Cancer Lett. 2012;324:142–151. doi: 10.1016/j.canlet.2012.05.019. [DOI] [PubMed] [Google Scholar]
- 70.Rio MC, Dali-Youcef N, Tomasetto C. Local adipocyte cancer cell paracrine loop: can «sick fat» be more detrimental? Horm Mol Biol Clin Investig. 2015;21:43–56. doi: 10.1515/hmbci-2014-0044. [DOI] [PubMed] [Google Scholar]
- 71.Vandevijvere S, Chow CC, Hall KD, Umali E, Swinburn BA. Increased food energy supply as a major driver of the obesity epidemic: a global analysis. Bull World Health Organ. 2015;93:446–456. doi: 10.2471/BLT.14.150565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Te Morenga LA, Howatson AJ, Jones RM, Mann J. Dietary sugars and cardiometabolic risk: systematic review and meta-analyses of randomized controlled trials of the effects on blood pressure and lipids. Am J Clin Nutr. 2014;100:65–79. doi: 10.3945/ajcn.113.081521. [DOI] [PubMed] [Google Scholar]
- 73.Forouhi NG, Sharp SJ, Du H, van der A DL, Halkjaer J, Schulze MB, et al. Dietary fat intake and subsequent weight change in adults: results from the European Prospective Investigation into Cancer and Nutrition cohorts. Am J Clin Nutr. 2009;90:1632–1641. doi: 10.3945/ajcn.2009.27828. [DOI] [PubMed] [Google Scholar]
- 74.Chaput JP, Tremblay A, Rimm EB, Bouchard C, Ludwig DS. A novel interaction between dietary composition and insulin secretion: effects on weight gain in the Quebec Family Study. Am J Clin Nutr. 2008;87:303–309. doi: 10.1093/ajcn/87.2.303. [DOI] [PubMed] [Google Scholar]
- 75.Suji M, Tamai Y, Wada K, Nakamura K, Hayashi M, Takeda N, et al. Associations of intakes of fat, dietary fiber, soy isoflavones, and alcohol with levels of sex hormones and prolactin in premenopausal Japanese women. Cancer Causes Control. 2012;23:683–689. doi: 10.1007/s10552-012-9935-8. [DOI] [PubMed] [Google Scholar]
- 76.Rose DP. Effects of dietary fatty acids on breast and prostate cancers: evidence from in vitro experiments and animal studies. Am J Clin Nutr. 1997;66(6 Suppl):1513–1522. doi: 10.1093/ajcn/66.6.1513S. [DOI] [PubMed] [Google Scholar]
- 77.Hardy S, El-Assaad W, Przybytkowski E, Joly E, Prentki M, Langelier Y. Saturated fatty acid-induced apoptosis in MDA-MB-231 breast cancer cells A role for cardiolipin. J Biol Chem. 2003;278:31861–31870. doi: 10.1074/jbc.M300190200. [DOI] [PubMed] [Google Scholar]
- 78.Riccardi G, Giacco R, Rivellese AA. Dietary fat, insulin sensitivity and the metabolic syndrome. Clin Nutr. 2004;23:447–456. doi: 10.1016/j.clnu.2004.02.006. [DOI] [PubMed] [Google Scholar]
- 79.Farnetti S, Malandrino N, Luciani D, Gasbarrini G, Capristo E. Food fried in extra-virgin olive oil improves postprandial insulin response in obese, insulin-resistant women. J Med Food. 2011;14:316–321. doi: 10.1089/jmf.2009.0264. [DOI] [PubMed] [Google Scholar]
- 80.Rose DP, Connolly JM, Coleman M. Effect of omega-3 fatty acids on the progression of metastases after the surgical excision of human breast cancer cell solid tumors growing in nude mice. Clin Cancer Res. 1996;2:1751–1756. [PubMed] [Google Scholar]
- 81.Welsch CW. Review of the effects of dietary fat on experimental mammary gland tumorigenesis: role of lipid peroxidation. Free Radic Biol Med. 1995;18:757–773. doi: 10.1016/0891-5849(94)00187-o. [DOI] [PubMed] [Google Scholar]
- 82.Hardman WE, Munoz J Jr, Cameron IL. Role of lipid peroxidation and antioxidant enzymes in omega 3 fatty acids induced suppression of breast cancer xenograft growth in mice. Cancer Cell Int. 2002;2:10. doi: 10.1186/1475-2867-2-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Sun H, Berquin IM, Edwards IJ. Omega-3 polyunsaturated fatty acids regulate syndecan-1 expression in human breast cancer cells. Cancer Res. 2005;65:4442–4447. doi: 10.1158/0008-5472.CAN-04-4200. [DOI] [PubMed] [Google Scholar]
- 84.Saadatian-Elahi M, Norat T, Goudable J, Riboli E. Biomarkers of dietary fatty acid intake and the risk of breast cancer: a meta-analysis. Int J Cancer. 2004;111:584–591. doi: 10.1002/ijc.20284. [DOI] [PubMed] [Google Scholar]
- 85.Kitahara CM, Berrington de González A, Freedman ND, Huxley R, Mok Y, Jee SH, et al. Total cholesterol and cancer risk in a large prospective study in Korea. J Clin Oncol. 2011;29:1592–1598. doi: 10.1200/JCO.2010.31.5200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Danilo C, Frank PG. Cholesterol and breast cancer development. Curr Opin Pharmacol. 2012;12:677–682. doi: 10.1016/j.coph.2012.07.009. [DOI] [PubMed] [Google Scholar]
- 87.Voisin M, de Medina P, Mallinger A, Dalenc F, Huc-Claustre E, Leignadier J, et al. Identification of a tumor-promoter cholesterol metabolite in human breast cancers acting through the glucocorticoid receptor. Proc Natl Acad Sci U S A. 2017;114:9346–9355. doi: 10.1073/pnas.1707965114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Nelson ER, Wardell SE, Jasper JS, Park S, Suchindran S, Howe MK, et al. 27-Hydroxycholesterol links hypercholesterolemia and breast cancer pathophysiology. Science. 2013;342:1094–1098. doi: 10.1126/science.1241908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Griffin JD, Lichtenstein AH. Dietary Cholesterol and Plasma Lipoprotein Profiles: Randomized-Controlled Trials. Curr Nutr Rep. 2013;2:274–282. doi: 10.1007/s13668-013-0064-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Ni H, Liu H, Gao R. Serum Lipids and Breast Cancer Risk: A Meta-Analysis of Prospective Cohort Studies. PLoS One. 2015;10:e0142669. doi: 10.1371/journal.pone.0142669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Ikonen E. Cellular cholesterol trafficking and compartmentalization. Nat Rev Mol Cell Biol. 2008;9:125–138. doi: 10.1038/nrm2336. [DOI] [PubMed] [Google Scholar]
- 92.Barclay M, Skipski VP, Terebus-Kekish O, Merker PL, Cappuccino JG. Serum lipoproteins in rats with tumors induced by 9,10-dimethyl-1,2-benzanthracene and with transplanted Walker carcinosarcoma 256. Cancer Res. 1967;27:1158–1167. [PubMed] [Google Scholar]