
Figure 1.
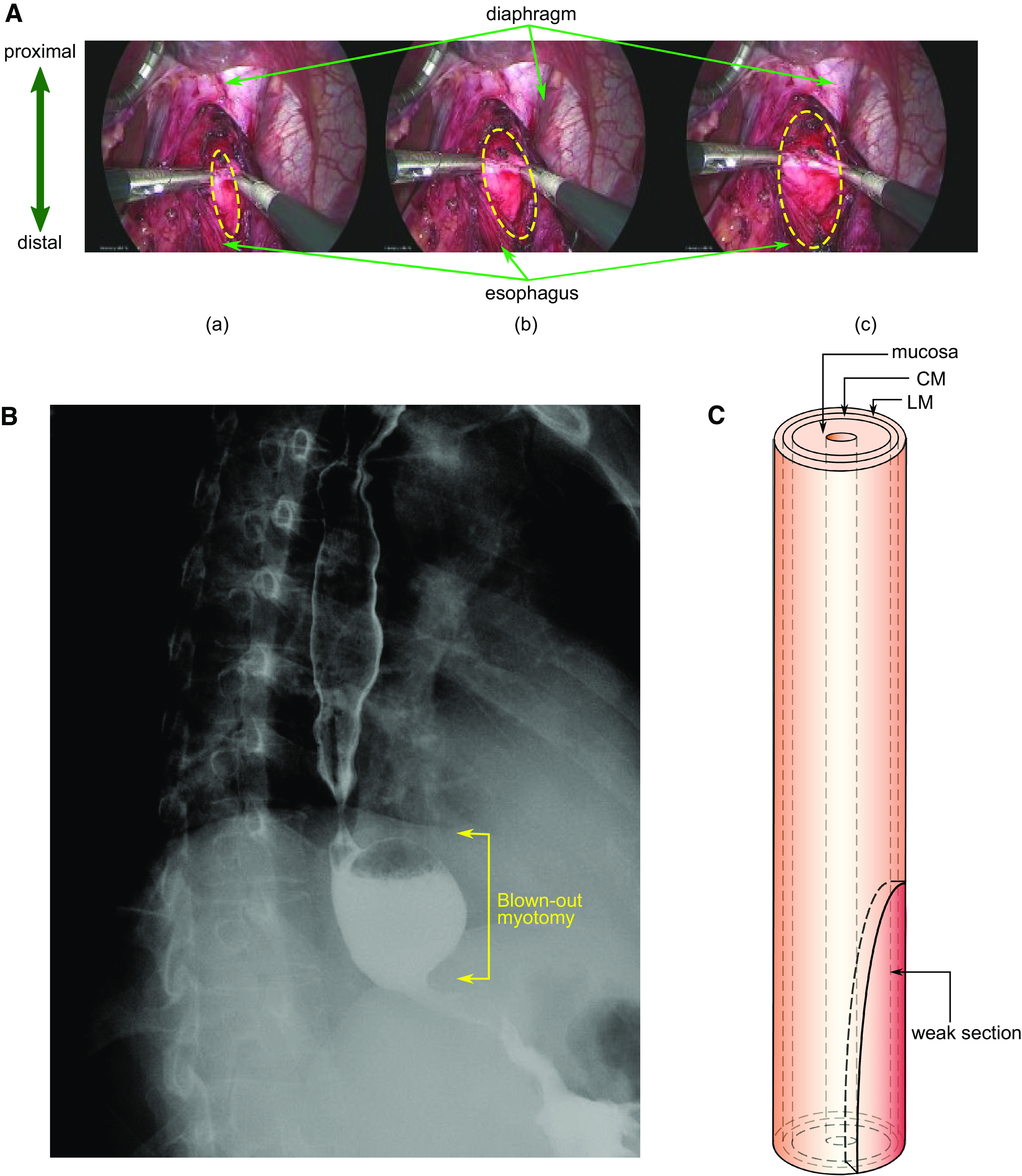
A: laparoscopic Heller myotomy. Distal esophagus during laparoscopic myotomy is shown. Top: the diaphragmatic crus arcing over the esophagus. The longitudinal muscle is separated, and the circular muscle is broken. The myotomy region takes the form of an ellipse. The upper half of the ellipse approximately extends from the LES to the distal esophagus. The lower half of the weak section extends from the LES into the stomach. a–c) three times during the myotomy are presented. The dashed yellow ellipses show the enlarging area of bared mucosa with progression of the myotomy. Maximum extension of the opened grasper (=2 cm) was used as a scale to calculate to the dimensions of myotomy and diameter of the esophagus. B: esophagram of a blown out myotomy (BOM). BOM formed in the patient after myotomy just above the diaphragm with the EGJ observed as the narrow region distal to the BOM. Barium is retained inside the pseudodiverticulum, almost filling it. C: vEsophagus model used in our simulations with three layers: LM, CM, and mucosa. The weakened region from the myotomy is shown as an ellipse at the distal end. During myotomy, the LM fibers are loosened and their connectivity with each other is disrupted; the CM fibers are broken. The matrix in which the muscle fibers are embedded remains in place, although its connection with the fibers might be broken. To model this behavior, we removed the muscle fibers in the CM and LM in an elliptical region near the distal end of the esophagus. We have modeled the myotomy affected region by weakening a half-elliptical section at the distal end of the esophagus (since the lower half extends into the stomach). CM, circular muscle; EGJ, esophagogastric junction; LES, lower esophageal sphincter; LM, longitudinal muscle.