
Figure 2.
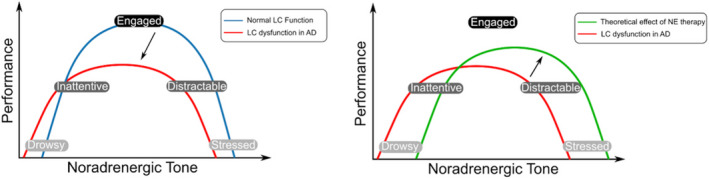
Schematic showing the Yerkes–Dodson arousal curve and the possible effects of noradrenergic therapy. (A) Shows the two theoretical versions of the arousal curve; one representing normal LC function in health (blue), and one representing the curve that may be seen with LC dysfunction in AD (red). The black arrow represents the transformation between the two curves. Pathology in this system in AD is likely to affect the dynamics of the ascending arousal system and disturb the balance of arousal seen in health. This dysfunction results in the curve moving to the left, representing a decreased likelihood that they will be in an ‘engaged’ state, whilst they also have an increased tendency to be in low performance states; ‘drowsy’ and ‘stressed’. (B) Shows the same curve for LC dysfunction in AD as well as the theoretical curve seen patients who have received noradrenergic therapy. The black arrow represents the transformation between the two curves. Noradrenergic therapy is theorised to heighten the noradrenergic tone in patients, moving the curve to the right, and therefore leading to an increasing likelihood that patients will be in an ‘engaged’ state. Successful use of noradrenergic treatments may rely on dose titration in order to ‘tune’ the system to the central peak of the classic inverted‐U curve. 136 It has the potential to lead to ‘over‐arousal’, however, with the line shifted too far to the right, and therefore patients may be more ‘stressed’ than ‘engaged’. LC, locus coeruleus; AD, Alzheimer's disease, NE, noradrenaline.