
Fig. 3.
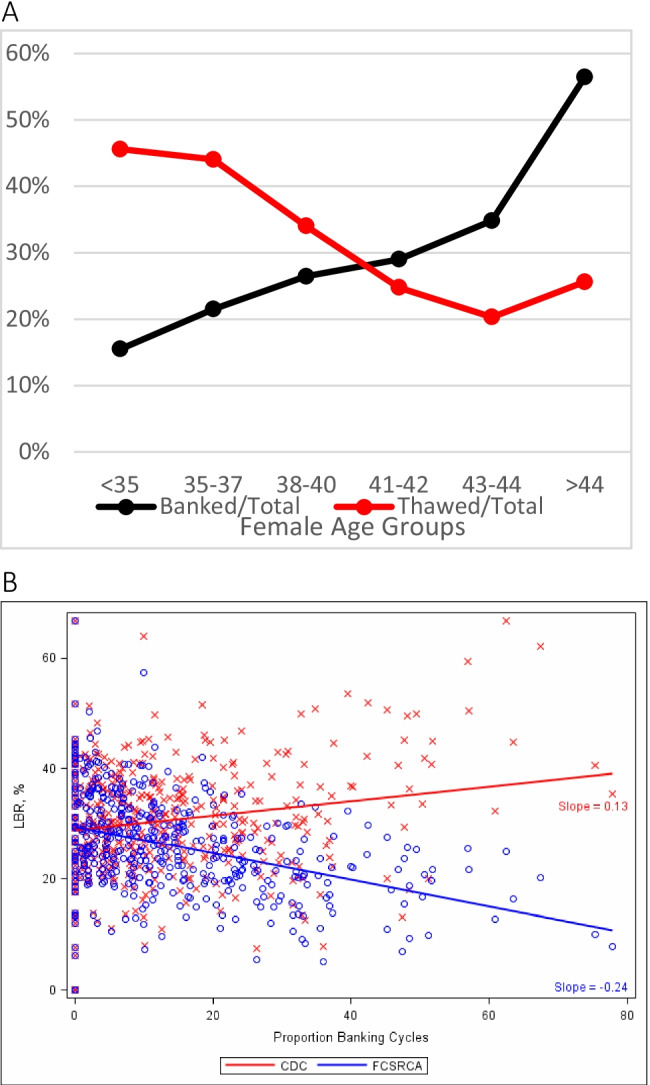
Embryo banking and thawing in the USA by age of patient. A: US IVF centers reporting to the CDC in 2013 modified with permission from Kushnir et al. [92, 93]. It depicts growing number of “banked” cycles with advancing female age, yet declining numbers of thawed cycles and, therefore, significant patient selection biases by US IVF centers in embryo cryopreservation disfavoring older women by not even using in older women embryos even in thaw cycles. Thereby not completing cycles with embryo transfers, those cycles’ outcomes then did not appear in the center’s outcome statistics reported to CDC. By removing older patients from consideration, better prognosis patients are left, artificially improving a center’s IVF cycle outcomes, demonstrated in B: Live birth rate of banked cycles according to two different calculations: The red line reflects live birth rates under the at that time reporting guidelines to the CDC that allowed exclusion of unresolved cycles and clearly suggests outcome improvements with higher banking rates. The blue line, in contrast, excluded banking cycles, demonstrating that rates actually declined with increasing banking. The authors also reported that only 13/341 IVF centers (3.8%) accounted for 50% of all from CDC-reporting excluded cycles. They uniformly were among the US centers reporting highest live birth rates. Once cycles were, however, appropriately adjusted, these centers’ live birth rates equally uniformly fell below the median of remaining over 300 centers