
Fig. 3.
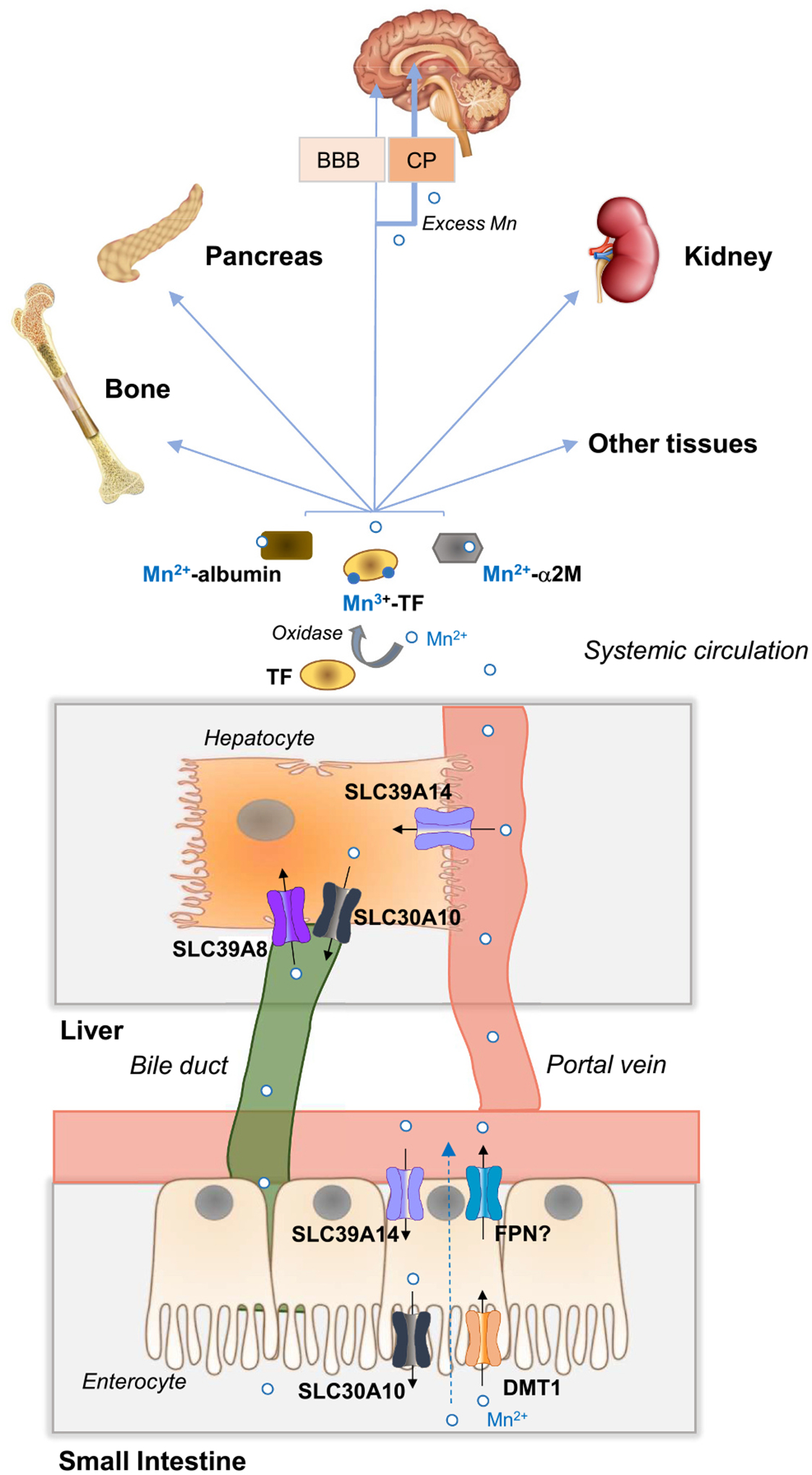
Whole-body Mn transport, metabolism, and distribution. In the small intestine, dietary Mn (Mn2+) is absorbed by incompletely characterized mechanisms that do not require DMT1 or FPN (dashed arrow). DMT1 may contribute significantly to Mn uptake in iron deficiency when DMT1 levels are upregulated. FPN may function in Mn export, but its exact contribution remains to be established. Mn2+ in portal blood is mostly taken up into the liver via SLC39A14 at the basolateral membrane of hepatocytes. Mn in plasma is found as Mn2+ associated with citrate and proteins such as albumin and α2M (α2-macroglobulin) or as Mn3+ bound to transferrin. The oxidation of Mn2+ to Mn3+ does not readily occur and therefore is likely catalyzed by an oxidase. Mn in plasma is taken up by all tissues, but primarily by the liver, pancreas, kidney, brain, and bone. Excess Mn accumulates preferentially in the bone, liver, kidney, pancreas, and brain, with net accumulation reflecting a balance between uptake and efflux of the metal. To enter the brain, Mn must cross the BBB (blood-brain-barrier) or the CP (choroid plexus). When plasma Mn levels are high, excess Mn enters the brain predominantly via the CP. In the liver, Mn that is not utilized by the hepatocyte is excreted into the bile via SLC30A10 located at the apical canalicular membrane. Hepatocyte SLC39A8 at the apical canalicular membrane reclaims Mn from the bile to prevent Mn deficiency. Mn in bile is secreted into the small intestine where it may undergo enterohepatic recirculation or be subsequently eliminated via feces. Mn in blood plasma can also be excreted directly by the intestine via SLC39A14 located on the enterocyte basolateral membrane and SLC30A10 located at the enterocyte apical membrane. Additional details are described in Section 4.1.