
Figure 4.
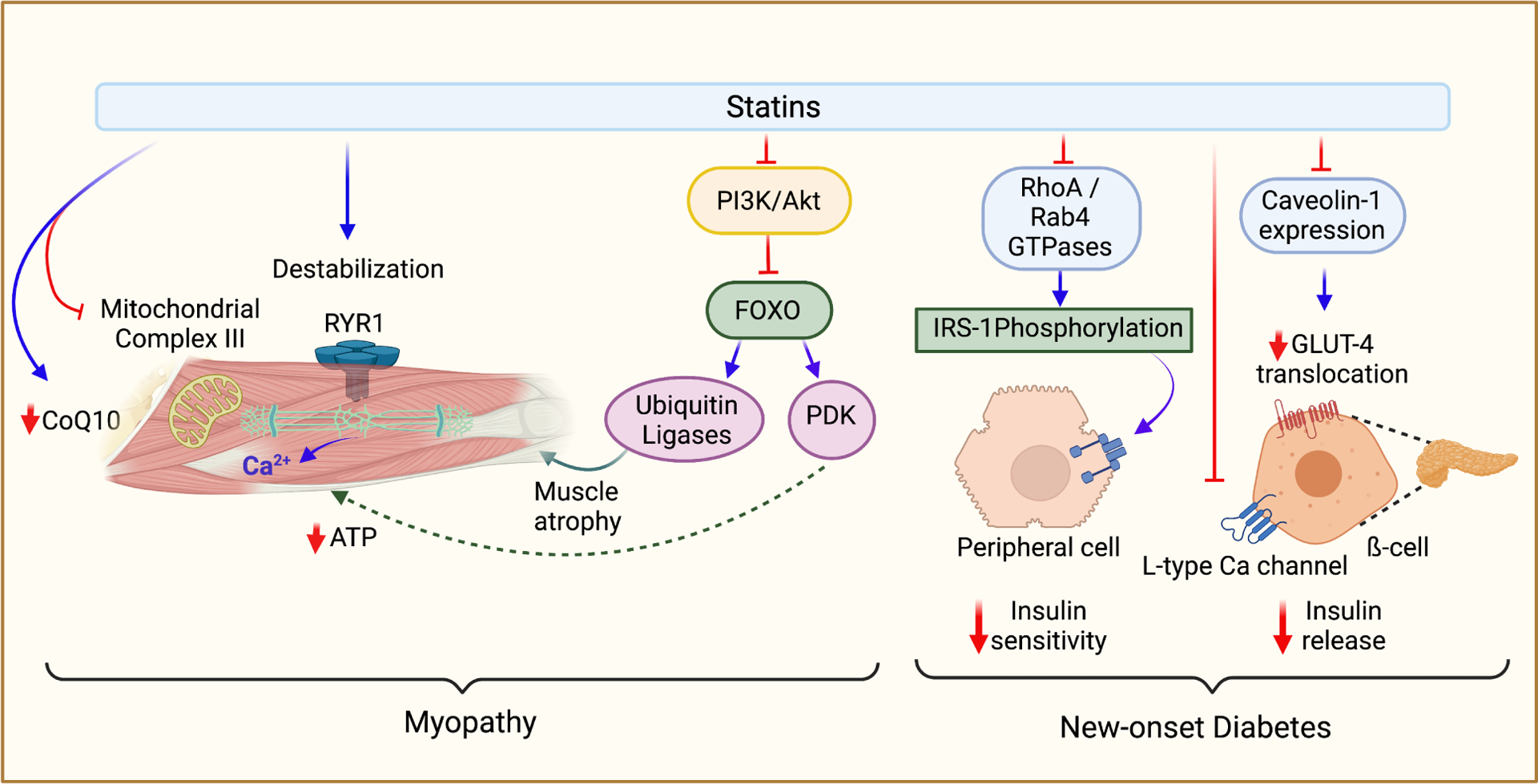
Adverse effects of statins. The two most common adverse effects associated with statins are myopathy and new-onset type 2 diabetes; the mechanisms of this pathology are described above. Myopathy is primarily due to reduced coQ10 production following statin treatment. Reduced levels of coQ10 can decrease mitochondrial respiration, leading to less ATP production in skeletal muscle cells. In a similar mechanism, lactone statins have also been shown to inhibit complex III of the electron transport chain by offsite binding to the Q0 site. Myopathy can also be triggered by destabilized activation of RYR1, leading to excess calcium release in a pathology similar to malignant hyperthermia. PI3K/Akt inhibition by statins leads to activation of the FOXO protein, which can then increase the nuclear expression of ubiquitin ligases and PDK, both of which can lead to muscle atrophy. There are multiple mechanisms of statin-induced diabetes. Insulin release from pancreatic ß-cells may be impaired by statin-mediated downregulation of GLUT-2 transporter. Inhibition of L-type calcium channels in pancreatic ß-cells (due to cholesterol depletion-associated membrane alteration) can lead to impaired insulin release from the pancreas. Several mechanisms may also lead to insulin resistance. Inhibition of prenylation of RhoA and Rab4 GTPases can lead to inhibition of IRS-1 phosphorylation and thus inhibition of downstream insulin signaling pathways. Downregulation of caveolin-1 expression can lead to decreased GLUT4 translocation to cellular membranes.