
Fig. 3.
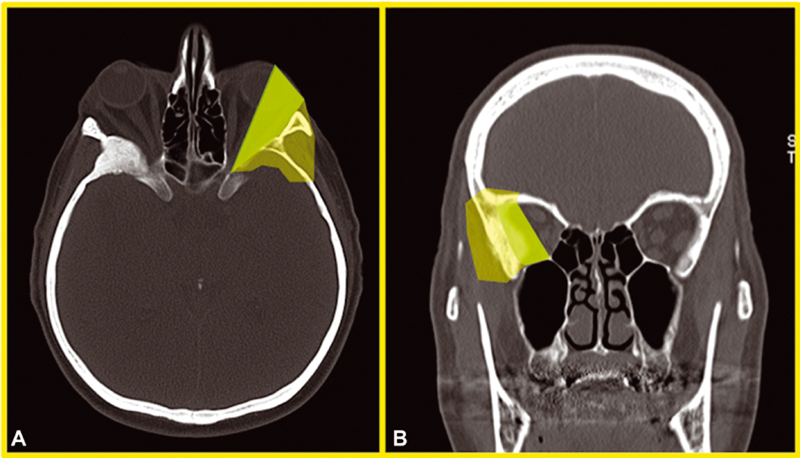
Anatomical criteria for endoscopic superior eyelid approach (SEA) choice. ( A,B ) Axial and coronal bone window computed tomography (CT) scans of an spheno-orbital meningioma (SOM) patient demonstrating a green area (heavily shaded in black-and-white version) and a more transparent periphery area in the left orbital region. The darker area comprehends the intraorbital area, lateral to the optic nerve, that may be easily accessed through an endoscopic SEA for the removal of intra- and extraconal pathologies or for the control of the intraorbital growing of a symptomatic SOM. When a patient complains of ocular-related symptoms that are reasonably linked to the osseous or parenchymatous growing of an SOM in such area, it eventuality represents a strong indication for an endoscopic SEA from a purely anatomical point of view. The more peripheral area, comprehending anterior and middle cranial base, lateral orbital wall with temporalis muscle, up to the most anterior part of temporal lobe, may be also accessed from a transorbital route, although for such cases, the decision to perform an endoscopic SEA should be even more carefully counterbalanced in light of the other factors discussed in the text (age, eventual comorbidities, desired extent of resection, etc.) that may favor a craniotomic approach with a consequent higher chance of obtaining a gross total resection.