

 This work is licensed under a
This work is licensed under a Abstract
Poorly differentiated thyroid carcinoma (PDTC) is a rare thyroid carcinoma originating from follicular epithelial cells. No explicit consensus can be achieved to date due to sparse clinical data, potentially compromising the outcomes of patients. In this comprehensive review from a clinician’s perspective, the epidemiology and prognosis are described, diagnosis based on manifestations, pathology, and medical imaging are discussed, and both traditional and emerging therapeutics are addressed as well. Turin consensus remains the mainstay diagnostic criteria for PDTC, and individualized assessments are decisive for treatment option. The prognosis is optimal if complete resection is performed at early stage but dismal in nearly half of patients with locally advanced and/or distant metastatic diseases, in which adjuvant therapies such as 131I therapy, external beam radiation therapy, and chemotherapy should be incorporated. Emerging therapeutics including molecular targeted therapy, differentiation therapy, and immunotherapy deserve further investigations to improve the prognosis of PDTC patients with advanced disease.
Keywords: poorly differentiated thyroid carcinoma, PDTC
Introduction
The incidence of thyroid cancer, the most common endocrine malignancy, has been increasing over the past decades. More than 87% of thyroid cancers are distinguished as differentiated thyroid carcinoma (DTC), including papillary thyroid cancer carcinoma (PTC), follicular thyroid carcinoma (FTC), and Hürthle cell cancer (1). Notwithstanding diverse biological features, most DTC patients are characterized with a favorable prognosis, as reflected by 10-year survival rates of about 90% (2). On the opposite, anaplastic thyroid carcinomas (ATCs), which are characterized by aggressive and rapidly fatal nature, typically confer a dismal outcome as reflected by 2-year survival rates of about 10–15% (3).
As an individual form of thyroid carcinoma derived from follicular epithelial cells, poorly differentiated thyroid carcinoma (PDTC) ranks between DTC and ATC regarding the degree of differentiation (4). PDTC was initially proposed as a separate entity by Sakamoto et al. in 1983 (5), immediately followed by Carcangiu et al. who deemed the histologic growth pattern as ‘insular’ carcinoma in 1984 (6). Twenty years later, PDTC was recognized as a distinct pathologic entity in the classification of thyroid tumors by World Health Organization (WHO) Classification of Endocrine Tumors (7). In 2006, pathologists from Italy, Japan, and the United States refined the definition of PDTC in Turin by reviewing a cohort of 83 cases that had been selected according to the presence of solid/trabecular/insular (STI) growth patterns. Heretofore, a consensus of pathological diagnostic criteria of PDTC was initially developed based on the characteristics of morphological features (8). The latest 2017 WHO Classification of Tumors of Endocrine Organs adopted the Turin criteria for PDTC and indicated that any poorly differentiated component should be mentioned in the pathology report.
PDTC accounts for 3–5% of all thyroid carcinomas (9, 10), and the variation in incidence is commonly ascribed to environmental factors and differences in histopathological interpretation (11). A mean age between 55 and 63 years and a slight female preponderance can be found, which is similar to those of DTC and ATC (12, 13). The 5-, 10-, and 15-year survival rates of PDTC patients were 50–85%, 34–50%, and 0%, respectively (14, 15, 16, 17). Despite low constituent ratio in thyroid carcinoma, a relatively high number of deaths related to thyroid carcinoma are attributable to PDTC.
Currently, sparse clinical data, insufficient diagnosis, and no explicit management algorithm make the standard treatment of PDTC unclear. The clinical therapeutic options mainly extrapolated from the preformed experiences on DTC and ATC may prevent PDTC patients from getting maximum benefit. We performed a comprehensive PubMed search combined with hand search using the term ‘poorly differentiated thyroid carcinoma’, yielding 1568 articles prior to June 31, 2021. Hereby, the clinical diagnosis and treatment including surgery, 131I therapy, external beam radiation therapy (EBRT), chemotherapy, and emerging therapeutics are addressed in detail in this dedicated review.
Diagnosis
A lump neck with rapid volume growth is the most common symptom and sign of PDTC, along with hoarse voice, dyspnea, or dysphagia if laryngeal nerve, weasand, or esophagus is invaded. However, none of the clinical features can accurately diagnose PDTC. Minority of cases may be recognized by fine-needle aspiration biopsy (FNAB) (18). As is demonstrated in Fig. 1, the definitive diagnosis mainly relies on histopathology, while immunohistochemistry and molecular characteristics substantially increase the diagnostic accuracy (19). There is a higher frequency of TP53 and TERT promoter mutations in PDTC compared to DTCs (19). Besides, although 15% of PDTC patients are metastatic at presentation, it is of note that distant metastases occurred in up to 37–85%, and 60% died of distant disease over the course (20, 21, 22), which strengthen the significance of comprehensive assessments for patients as the basis of treatment strategy (23).
Figure 1.
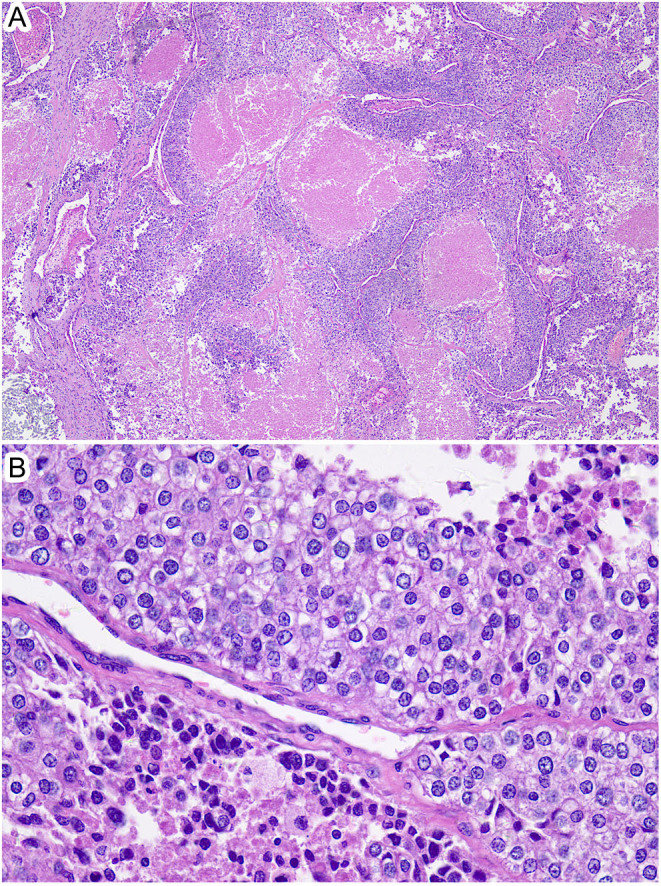
Poorly differentiated thyroid carcinoma in a 64-year-old male. Panel A shows marked tumor necrosis (×40). Panel B shows solid trabecular tumor without nuclear features of papillary thyroid carcinoma. Foci of necrosis are found in the upper and lower parts of the photo. Mitotic figure is presented in the center of the figure (×400). Hematoxylin and eosin staining. Somatic mutation of TERT promoter (C228T) was confirmed by next-generation sequencing.
Pathology
PDTC is traditionally defined by a specific histopathology assisted with immunohistochemistry and molecular genetics, which is substantially compensated by the biological behaviors of tumor. The Turin standards based on the growth pattern of STI and the Memorial Sloan Kettering Cancer Center (MSKCC) standards based on proliferative grading are mainly involved in the histopathological definition of PDTC.
Histopathology nature
According to the Turin consensus, the following requirements for diagnosis of PDTC should be met: I. STI microscopic growth pattern; II. lack of well-developed nuclear features of papillary carcinoma; III. presence of at least one of the following features: convoluted nuclei, mitotic activity ≥3/10 high power microscopic fields (HPF), and necrosis (24). The above ‘Turin consensus criteria’ was adopted as a uniform definition for histopathological diagnosis for PDTC in the WHO Classification of Endocrine Tumors (25). A representative histopathologic figure is presented (Fig. 1).
Nevertheless, the deficiencies of the above Turin consensus exist. First, features distinguishing PDTC from other follicular epithelial cell-derived tumors are unclear. For instance, some overlap exists in the differential diagnosis between PDTC and the solid variant of papillary carcinoma or DTCs with predominant solid or trabecular growth patterns (26). A recent study has demonstrated that PTC with high-grade features, which has a higher BRAFV600E mutation rate, a trend toward more gene fusions compared with those with PDTC, and more aggressive behavior, should be considered a distinct group from PDTC (27). Secondly, there has not been a threshold of the minimum proportion of poorly differentiated (PD) area in DTC tissue to diagnose PDTC since the survival data in patients with PD area >50% did not differ from those with PD area >10%, and no difference was found in the outcomes of PDTC and DTC with PD area (28, 29), which makes us wonder the presence of any PD area should be enough to label a tumor as PDTC rather than the proportion. Finally, Hiltzik et al. showed that growth patterns did not correlate with overall survival using multivariate analysis, suggesting that the growth pattern may not be representative of tumor aggressiveness (30).
Besides, Volante found that PDTC patients with a low numerical score demonstrated a survival curve similar to DTC group, while necrosis and high mitotic rate represented the worst and most relevant prognostic factors (31). Innovatively, the head and neck pathologists at MSKCC diagnose this tumor using high mitotic rate (≥5 mitosis/10 HPF) and/or fresh tumor necrosis (30, 32). Meanwhile, high-grade pathological parameters, including a mitotic index of >3/HPF, necrosis, predominant presence of an insular component, have been found to be associated with a poor prognosis in terms of ongoing disease or death (33, 34).
Immunohistochemical features
Immunohistochemistry has been widely considered to increase the accuracy of diagnosis by narrowing the differential diagnoses and reflecting the progression of tumor. Moreover, the results of immunohistochemistry confirm the theory of a continuum from DTC to ATC through PDTC. However, no specific immunohistochemical marker has been established for the detection of PDTC yet (14, 18).
Majority of DTCs express high levels of thyroglobulin (Tg); however, the expression of Tg was absent or weakly positive in more than half of PDTCs (35). Although the role of Tg expression as a diagnosis criterion of PDTC remains undetermined, a study has shown that Tg expression in PDTC may predict the iodine avidity of lesions (36). PDTC is immunoreactive for thyroid transcription factor 1 (TTF1), PAX-8, and cytokeratin, confirming that PDTC originates from follicular epithelial cells in another perspective. Contrarily, ATC, rarely expressing Tg or TTF1, is diagnostically supported by strong positive immunoreaction with cytokeratin, and 85% of ATC was reported to be positive for PAX-8 (18, 37). The absence of membranous expression of E-cadherin, which relates to the differentiation level of thyroid carcinomas, helps distinguishing PDTC from DTC (38).
In addition, the negative expression of calcitonin, chromogranin, and carcinoembryonic antigen in PDTC can exclude neuroendocrine tumors, that is, medullary thyroid carcinoma (39). Likewise, PDTC is not immunoreactive with hematopoietic cellular markers, such as B-lymphocyte antigen (CD19 and CD20) and plasma cell marker (CD138), which helps ruling out lymphoproliferative disorders (14). In addition, high expression of IMP3, which is associated with tumor-associated death, lymph node metastasis, and distant metastasis, is useful for predicting poor prognosis (11).
Molecular characteristics
From the perspective of molecular characteristics, increasing evidence prove that PDTC is derived from DTC and is the intermediate state between DTC and ATC (40). The genetic alterations, including RAS (including HRAS, NRAS, and KRAS) mutation, BRAF mutation(predominantly V600E), TERTpromotermutations (C228T and C250T ) activating telomerase and contributing to tumorigenesis, inactivating TP53 mutations, and ATMmutations, have been found in PDTC. The understanding of tumor’s molecular characteristics becomes more detailed and comprehensive given the next-generation sequencing. The heterogeneity of genetic characteristics may be reflected by different response to a certain targeted treatment, providing implication for treatment options and their clinical outcomes (40). To date, however, the role of molecular profiling in directing therapy for PDTC remains indeterminate due to insufficient data (31).
High frequencies of mutually exclusive mutations of RAS and BRAF have been found in PDTCs. RAS activates both the MAP kinase pathway and the PI3K/AKT pathway, and the presence of RAS gene alterations could be found in 25–35% of PDTCs (41, 42, 43). BRAF is specific to the activation of the MAP kinase pathway and the BRAF mutation is present in 15–27% of patients with PDTC (41, 42). The strong association of PDTC-Turin tumors with RAS mutations had been found, whereas PDTC-MSK tumors were strongly associated with BRAF (44). Moreover, PDTCs derived from papillary thyroid cancer with mutant BRAF possess a higher probability of regional nodal metastases, and distant metastases occur more frequently in patients with follicular thyroid cancer-derived RAS-mutant PDTC (1, 44).
As another kind of common alteration in PDTC, TERT promoter mutation has been identified with a frequency of 40%, ranking in the middle of PTC (9%) and ATC (65–73%) (44). TERT encodes the reverse transcriptase component of the telomerase complex and is highly expressed in most human cancer cells (45). Mutations of TERT promoter gene in PDTC usually indicate an aggressive phenotype and a dismal prognosis. In PDTC and ATC, a significant co-occurring association between TERT promoter mutation and BRAF or RAS mutation has been identified (44). This is most likely due to the de novo binding elements on the mutant TERT promoter for MAPK signaling-activated E-26 family of transcription factors (46), causing TERT over-expression and induction of an immortalized phenotype.
As a tumor suppressor gene, however, p53 gene plays vital role in hindering or reversing carcinogenic effects. Mutant TP53, which is more prevalent in ATC (65–73%), is highly prevalent in patients with PDTC (16–28%) but rarely associated with DTC (15, 47, 48). On the other side, alterations in p53gene were circumscribed in the less differentiated part of tumor histological samples containing both DTC and PDTC components. Therefore, p53 mutations may predict that tumor will be triggered by dedifferentiation and evolution to PDTC and ATC (15). ATM, another tumor suppressor gene controlling the cell-cycle checkpoint and repair DNA, mutates in 7% of PDTC and 9% of ATC. This finding suggests that PDTC carrying ATM mutation may possess an aggressive behavior before progression to ATC (44). Lastly, RET/PTC rearrangement and PAX8:PPARγ rearrangement which occur in other thyroid carcinomas are almost never found in PDTC (42, 47). PDTC in children and adolescents were strongly associated with DICER1 mutations, which are distinct from adult-onset PDTC (49).
Medical imaging
Local recurrence and distant metastasis have been revealed as independent predictors for worse disease-specific survival (50). Meanwhile, the extent of invasion appears to be an important parameter that affects the clinical outcome for patients with PDTC (51). Therefore, the individual assessment becomes indispensable not only for diagnosis but also for management. Anatomic imaging assessments have been strongly compensated by molecular imaging in the last decade, which has been recently updated by our group (52).
High-resolution sonography and FNAB are sensitive and convenient diagnostic tools for thyroid carcinoma. PDTC commonly presents as relatively low echo or heterogeneous echo mass with a circumscribed margin and an oval-to-round shape on sonography (23). As vocal cord and laryngeal nerve are frequently affected in patients with extrathyroidal extension, the preoperative evaluation is critical. Esophagography, esophagoscopy, bronchoscopy, and the evaluation of vocal cord function may lay an important foundation for therapeutic decision-making via assessing neighboring structures possibly involved (47). If extrathyroidal extension or extensive local invasion is suspected, the use of enhanced CT and MRI helps to clarify the anatomic relationship between the lesion and surrounding structures (47).
Nuclear medicine imaging, such as 131I whole-body scan and 18F-FDG PET scan, offers detailed information on disease at molecular and cellular levels based on metabolism and biochemical processes (51). Of note, the dedifferentiation of tumor with consequent deficiency of the sodium/iodine symporter trafficking to membrane may result in negative 131I scans, while 18F-FDG PET/CT is able to detect distant metastases in 71% of patients with a history of PDTC, increased thyroglobulin levels, and negative 131I imaging (‘flip-flop’ theory) (Fig. 2). Besides, 18F-FDG PET/CT is also useful in planning EBRT and assessing response to treatment since the total volume of FDG-avid disease has been recognized as a single risk factor predicting survival (53, 54). As a demonstration of tumor heterogeneity, different patterns of tumoral uptakes were detected on 18F-FDG, 68Ga-DOTATATE, and 68Ga-PSMA PET/CT (55).
Figure 2.
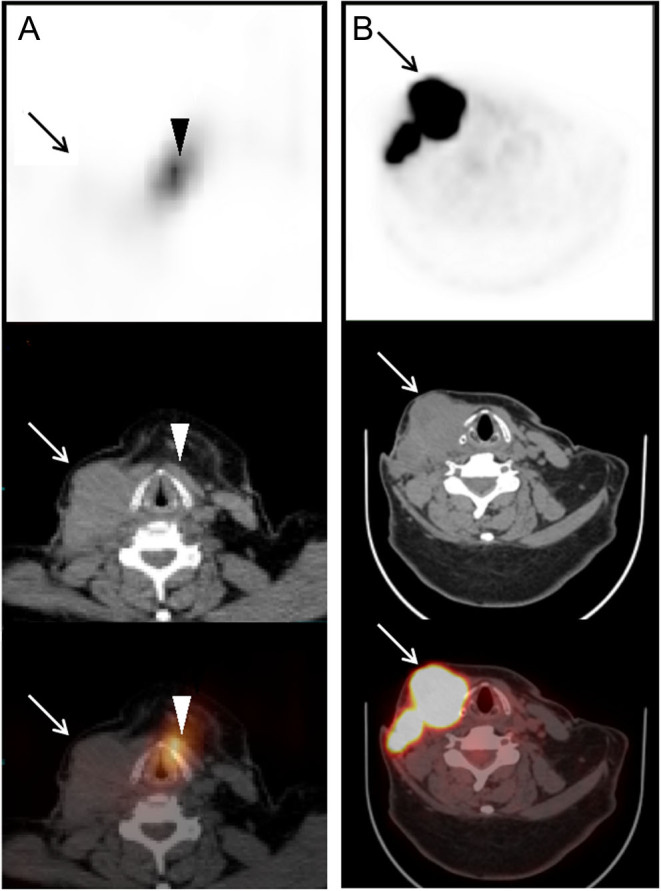
‘Flip-flop’ phenomenon in a 60-year-old woman with PDTC. Panel A shows 131I-nonavid lymph node metastases by SPECT/CT scan (upper, SPECT image; middle, CT image; lower, SPECT/CT fusion image). Panel B shows lymph node metastases uptaking fluorodeoxyglucose by 18F-FDG PET/CT imaging with maximum standardized uptake value of 33.6 (upper, PET image; middle, CT image; lower, PET/CT fusion image). Arrow, lymph node metastases; Aarrow head, thyroid remnant.
Management
Currently, it is difficult to draw conclusions about the uniform recommendations from the literatures available concerning the therapeutic procedures for PDTC. Surgery remains the mainstay of treatment among the traditional therapeutic modalities. Multimodal therapy may prolong 5-year-survival rate, varying between 47% and 89% (Table 1).
Table 1.
The characteristics and outcomes of patients with PDTC in cohort studies classified by therapeutic regimen.
| Therapeutics | Reference | Sample size | Age (mean) | Diagnosis criteria for PDTC | Tumor size (cm, mean) | ETI (%) | LM (%) | DM (%) | 5-year survival rate (%) |
|---|---|---|---|---|---|---|---|---|---|
| TT | Tanaka 2011 (13) | 29 | 57 | TIS pattern | 3.1 | 55.2 | 72.4 | 13.8 | 89.3 |
| Wong 2019 (51) | 47 | 57 | 2017 Endocrine WHO criteria | 4.3 | 100 | 38 | 19 | 67 | |
| TT/thyroidectomy and RT | Volante 2004 (17) | 183 | 56.3 | TIS pattern | 5.3 | 54 | NR | NR | 85 |
| Hiltzik 2006 (30) | 58 | 56.5 | Follicular cell differentiation + necrosis or mitotic index >5/10 HPF | 5.6 | 64 | 12 | 66 | 60 | |
| Cherkaoui 2015 (61) | 7 | 60 | Turin criteria | 4 | NR | 51.7 | NR | 85 | |
| Yu 2017 (57) | 18 | 62 | Turin criteria | 5.8 | 44 | 28 | 28 | 83 | |
| TT and RT and EBRT | Jung 2007 (32) | 49 | 49.3 | TIS pattern + necrosis | 4.7 | 59 | 29 | 33 | 68 |
| Lin 2007 (56) | 67 | 50.3 | TIS pattern | 4.2 | NR | NR | 49.3 | 67 | |
| Ibrahimpasic 2013 (20) | 27 | 70 | Follicular cell differentiation + necrosis or mitotic index >5/10 HPF | NR | 30 | 80 | 37 | 47 | |
| Ibrahimpasic 2014 (50) | 91 | 59 | Follicular cell differentiation + necrosis or mitotic index >5/10 HPF | NR | 30 | 40.7 | 26 | 62 | |
| TT and RT and EBRT and CH | Siironen 2010 (60) | 8 | 66 | Turin criteria | 5.6 | 63 | 37.5 | 37.5 | 50 |
| TT and RT and EBRT and TKI | de la Fouchardière 2018 (10) | 104 | 62 | Turin criteria | NR | 40 | 21.2 | 35.8 | 72.8 |
| RT and EBRT | Zhang 2021 (66) | 522 | NR | NR | NR | NR | 51.7 | NR | 73.7 |
CH, chemotherapy; DM, distant metastasis; ETI, extrathyroidal invasion; LM, lymph node metastasis; NR, not reported; RT, radioiodine therapy; TKI, tyrosine kinase inhibitors; TT, total thyroidectomy.
Surgery
Total thyroidectomy with lymph node dissection is the first-line management for PDTC ideally. Esophageal submucosal resection, unilateral recurrent nerve resection, or palliative surgery would be chosen if tumor invades surrounding structures, such as esophagus, trachea, larynx, and recurrent nerve (20). The policy in the management of patients with PDTC and gross extrathyroidal extension is to achieve removal of all gross diseases in order to control the central compartment of the neck, minimize the risk of locoregional recurrence, and hence prevent life-threatening airway obstruction or hemorrhage. Nevertheless, data on the impact of operative approaches on clinical outcomes are insufficient to draw any conclusion (56). Satisfactory locoregional control with excellent 5-year locoregional control rate of 81% can be achieved by total thyroidectomy and clearance of all gross diseases (50, 57). One-third of PDTCs can be cured by lesion resection followed by 131I therapy (10). Besides, particular attention must be paid to non-cured patients or those with metastases, especially during follow-up.
131I therapy
Compared to DTC, PDTC does not usually respond to 131I therapy despite iodine avidity in some foci. To date, the majority of studies did not confirm the impact of 131I therapy on prolonging disease-specific survival or overall survival (47, 58, 59, 60). It was considered reasonable to utilize 131I therapy to control distant metastases which concentrate iodine well (50, 56, 61). The 131I-avidity, which is found in 70–80% of patients with PDTC, provides the basis for 131I therapy (22, 39, 50). Sanders et al. advocated that 131I therapy ought to be considered in every patient with PDTC after complete surgery, in light of the potential for 131I uptake and the lack of major side effects (62). Furthermore, the American Thyroid Association encourages that the patients with aggressive tumor histology should receive high dose (100–200 mCi) of 131I, including the insular variants (63, 64).
Nevertheless, there are also cases where the lesions show potential ability of uptaking 131I, but the therapeutic effect is not ideal. This may be ascribed to an impaired thyroid hormone synthesis system, yielding shortened 131I retention time and reduced radiation dose, which might be reflected by the discrepancy between pre-therapeutic 99mTc-pertechnetate scan and post-therapeutic 131I scintigraphy (Fig. 3). Favorable therapeutic effect may be achieved in patients with lesions retaining 131I for a sufficient period of time, which can be reflected by post-therapeutic whole body scan 3–7 days after 131I administration (Fig. 4). Recently, our group has demonstrated that the combined use of the maximum target/background ratio of 8.1 on the whole body scan and change rate of thyroid stimulating hormone-suppressed thyroglobulin level of 25.4% may efficiently identify biochemical responders/non-responders to next course of 131I therapy, warranting management optimization of patients with 131I-avid lesions (65).
Figure 3.

The discrepancy between 99mTc-pertechnetate and 131I scintigraphy in a 52-year-old woman with PDTC. Panel A shows multiple lesions accumulating 99mTc-pertechnetate in the skull and chest by 99mTc-pertechnetate WBS before thyroidectomy. SPECT/CT reveals 99mTc-pertechnetate-avid lesions in parietal bone (B, upper, SPECT image; middle, CT image; lower, SPECT/CT fusion image), left posterior rib (C, upper, SPECT image; middle, CT image; lower, SPECT/CT fusion image), and the right breast (D, upper, SPECT image; middle, CT image; lower, SPECT/CT fusion image). Histological analysis of punctured tissues from the right breast lump and the resected thyroid lobe demonstrates metastatic PDTC and PDTC, respectively. Panel E displays no 131I uptake in the above 99mTc-pertechnetate-avid lesions by post therapeutic 131I WBS on day 3 after the administration of 7.4 GBq of 131I. Arrow head, parietal bone metastasis; thin arrow, left posterior rib metastasis; thick arrow, right breast metastasis.
Figure 4.

Response to radioiodine therapy in a 62-year-old man with PDTC. Panel A shows several ‘hot spots’ in neck and chest, diffuse distribution of 131I in both lungs by post-therapeutic whole-body scan on day 3 after the initial administration of 7.4 GBq of 131I. SPECT/CT scan shows 131I-avid mediastinal lymph node measuring 34 mm × 28 mm (B, upper, SPECT image; middle, CT image; lower, SPECT/CT fusion image). Panel C shows similar findings to the initial post-therapeutic 131I whole body scan on day 3 after the second administration of 7.4 GBq. Panel D shows the shrinkage of the mediastinal lymph node measuring 29 mm × 25 mm (upper, SPECT image; middle, CT image; lower, SPECT/CT fusion image). Arrow head, mediastinal lymph node.
External beam radiation therapy
EBRT has been confirmed as an option for controlling local disease for patients with PDTC, which is based on extrapolation from studies about poor-prognosis DTC where substantial data exist regarding treatment benefit (47, 62). Sanders et al. suggested that EBRT should be considered in patients with tumors larger than 4 cm, extrathyroidal extension, lymph node metastasis or irradical surgery, unresectable disease. Therefore, EBRT may be selected as a palliative treatment for PDTC if 131I treatment fails in localized tumors, like local bone metastasis (62). According to the latest research, only the PDTC patients in high-risk cohort based on individualized nomogram were found eligible to benefit from postoperative radiotherapy (66). Intensity-modulated radiotherapy may be considered for adequately planning target volume coverage and minimizing dose to spinal cord (22, 67). During the course of radiation therapy, moderate skin erythema, dry or moist desquamation, and the mucositis of the esophagus, trachea, and larynx rarely occurred and are acceptable (68) but may make the subsequent surgery more difficult (69).
Chemotherapy
At present, there are no effective chemotherapy drugs or regimens dedicated for PDTC. Early studies of in vitro cell culture and chemosensitivity testing may prevent the administration of ineffective chemotherapeutic drugs, including adriamycin, cisplatin, cyclophosphamide, etoposide, and carboplatin (70). Several dosage regimens, such as adriamycin (68), a combination of methotrexate, adriamycin, bleomycin, and vinblastine (71), adriamycin-cisplatin combination, and paclitaxel-carboplatin regimen (72), have been explored for the chemotherapy of PDTC. Despite efforts to find a chemotherapeutic agent or a combination of agents to modulate PDTC progression, systemic chemotherapy has not yet produced clinically promising results.
Emerging therapeutics
Emerging therapeutics, including molecular targeted therapy, differentiation therapy, and immunotherapy are primarily used for thyroid carcinomas poorly controlled by traditional treatment, although most of the relevant researches remain ongoing.
Molecular targeted therapy
Inhibiting angiogenesis and tumor cell proliferation are the two mechanisms involved in molecular targeted therapy for advanced or progressive 131I-refractory thyroid carcinoma (63). Sorafenib and lenvatinib have been approved by the US Food and Drug Administration after seminal multicenter phase 3 studies for follicular cell-derived thyroid cancer in cases of progressive, recurrent, or metastatic disease not responsive to 131I therapy. In addition, several drugs listed in the Clinical Trials.gov database are being evaluated in ongoing trials, including cediranib, dabrafenib, cabozantinib, etc. (73). These agents selectively target multiple kinases, improving progression-free survival in patients with advanced DTC (74). When PDTC becomes 131I-refractory, kinase inhibitor therapy should not be ignored in patients with rapidly progressive disease and those with tumor-relevant symptoms (64).
A significant reduction in tumor size in PDTC patients and enhancement in proapoptotic activity in PDTC cells in vitro have been reported by treatment with sunitinib (75) and erlotinib (76), respectively. The enhancement of doxorubicin-induced proapoptotic activity by erlotinib provided a preliminary experimental basis of the combined application of targeted therapy and chemotherapy (76). Lenvatinib can be used to obtain hemodynamic stability with a neoadjuvant intent before thyroidectomy and radioiodine therapy (77) and has been demonstrated to be safe and effective in PDTC patients including complete and long-term remission when combined with pembrolizumab (78). Thus, the application of targeted therapy in advanced or 131I-refractory thyroid carcinoma may provide a new option for PDTC, and the exploration of relationship between PDTC and radioiodine-refractory differentiated thyroid carcinoma may be helpful to discover the pathological basis of radioiodine-refractory differentiated thyroid carcinoma. What we should not ignore is that most multikinase inhibitors do not bring significant overall survival benefit but induce a number of adverse effects in different grades, sometimes significantly impair quality of life, including fatigue, weight loss, indigestion, etc. (72). Our real-world study indicates that targeted therapy should be individualized to maximize survival benefit (79).
Differentiation therapy
Differentiation therapy has been deemed as a promising strategy that facilitates PDTC to recover the ability of 131I uptake and leads to prolonged survival. Several treatment strategies, such as retinoic acid (80), peroxisome proliferator-activated receptor gamma agonists (81), tyrosine kinase inhibitors (82, 83, 84), and neuro trophin receptor kinase inhibitors (85) have been explored for the differentiation therapy. Moreover, miRNA, DNA, and histones modifications may also lead to profound gene expression changes to facilitate differentiation of thyroid cancer (86, 87, 88).
Unfortunately, accumulating evidences have shown that their clinical effectiveness remains insufficient (89). For instance, it was revealed that tyrosine kinase inhibitors induced visible 131I uptake in only nearly 60% of subjects, and objective response was achieved in approximately one-third of patients who subsequently received therapeutic dose of 131I. Besides, the preparation of thyrogen prior to 131I therapy and sustained administration of tyrosine kinase inhibitor during 131I therapy are questionable.
Immunotherapy
Immune checkpoint inhibitors are a promising treatment option in a number of malignancies (90). Combination strategies that target multiple aspects of the tumor microenvironment could provide a more durable benefit for PDTC patients. There is only one recent study which discovered that 25% were positive for PD-L1 among the 28 PDTC patients, and 29% co-expressed IDO1, making immune checkpoint inhibitors as monotherapy or in combination with an IDO1 inhibitor become a novel treatment modality for selected patients with PDTC (91).
Conclusions
PDTC has been recognized as a rare entity with poor overall prognosis and challenging management. The intermediate state of differentiation between DTC and ATC correlates both molecular characteristics and clinical manifestations. Comprehensive assessments based on pathological diagnosis and medical imaging are critical for therapeutic decision-making and follow-up. Surgery, 131I therapy, and EBRT constitute the mainstay of traditional treatment for patients with advanced disease, while emerging therapies based on molecular alterations are promising, deserving further investigation to improve the prognosis of patients.
Declaration of interest
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of this review.
Funding
This study was sponsored by the Natural Science Foundation of China (81671711 and 82171981) and Shanghai Tenth People’s Hospital, Tongji University School of Medicine (2021SYPDRC064).
Author contribution statement
Junyu Tong and Maomei Ruan wrote this manuscript. Yuchen Jin, Hao Fu performed clinical diagnosis. Lin Cheng and Qiong Luo collected samples and contributed to data collection. Zhiyan Liu, Zhongwei Lv and Libo Chen conceived the project and reviewed the manuscript. All authors approved the final version of the manuscript. Junyu Tong and Maomei Ruan contributed equally to this work and share co-first authorship.
Acknowledgments
The authors thank the technical staff from Department of Nuclear Medicine for image acquisition.
References
- 1.Fagin JA, Wells SA. Biologic and clinical perspectives on thyroid cancer. New England Journal of Medicine 20163751054–1067. ( 10.1056/NEJMra1501993) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, Caillou B, Ricard M, Lumbroso JD, De Vathaire Fet al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. Journal of Clinical Endocrinology and Metabolism 2006912892–2899. ( 10.1210/jc.2005-2838) [DOI] [PubMed] [Google Scholar]
- 3.Molinaro E, Romei C, Biagini A, Sabini E, Agate L, Mazzeo S, Materazzi G, Sellari-Franceschini S, Ribechini A, Torregrossa Let al. Anaplastic thyroid carcinoma: from clinicopathology to genetics and advanced therapies. Nature Reviews: Endocrinology 201713644–660. ( 10.1038/nrendo.2017.76) [DOI] [PubMed] [Google Scholar]
- 4.Veiga LHS, Neta G, Aschebrook-Kilfoy B, Ron E, Devesa SS. Thyroid cancer incidence patterns in Sao Paulo, Brazil, and the U.S. SEER Program, 1997–2008. Thyroid 201323748–757. ( 10.1089/thy.2012.0532) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sakamoto A, Kasai N, Sugano H. Poorly differentiated carcinoma of the thyroid. A clinicopathologic entity for a high-risk group of papillary and follicular carcinomas. Cancer 1983521849–1855. () [DOI] [PubMed] [Google Scholar]
- 6.Carcangiu ML, Zampi G, Rosai J. Poorly differentiated (‘insular’) thyroid carcinoma. A reinterpretation of Langhans’ ‘wuchernde struma’. American Journal of Surgical Pathology 19848655–668. ( 10.1097/00000478-198409000-00005) [DOI] [PubMed] [Google Scholar]
- 7.Volante M, Papotti M. Poorly differentiated thyroid carcinoma: 5 years after the 2004 WHO classification of endocrine tumours. Endocrine Pathology 2010211–6. ( 10.1007/s12022-009-9100-4) [DOI] [PubMed] [Google Scholar]
- 8.Volante M, Collini P, Nikiforov YE, Sakamoto A, Kakudo K, Katoh R, Lloyd RV, LiVolsi VA, Papotti M, Sobrinho-Simoes Met al. Poorly differentiated thyroid carcinoma: the Turin proposal for the use of uniform diagnostic criteria and an algorithmic diagnostic approach. American Journal of Surgical Pathology 2007311256–1264. ( 10.1097/PAS.0b013e3180309e6a) [DOI] [PubMed] [Google Scholar]
- 9.Sassolas G, Hafdi-Nejjari Z, Remontet L, Bossard N, Belot A, Berger-Dutrieux N, Decaussin-Petrucci M, Bournaud C, Peix JL, Orgiazzi Jet al. Thyroid cancer: is the incidence rise abating? European Journal of Endocrinology 200916071–79. ( 10.1530/EJE-08-0624) [DOI] [PubMed] [Google Scholar]
- 10.de la Fouchardière C, Decaussin-Petrucci M, Berthiller J, Descotes F, Lopez J, Lifante JC, Peix JL, Giraudet AL, Delahaye A, Masson Set al. Predictive factors of outcome in poorly differentiated thyroid carcinomas. European Journal of Cancer 20189240–47. ( 10.1016/j.ejca.2017.12.027) [DOI] [PubMed] [Google Scholar]
- 11.Asioli S, Erickson LA, Righi A, Jin L, Volante M, Jenkins S, Papotti M, Bussolati G, Lloyd RV. Poorly differentiated carcinoma of the thyroid: validation of the Turin proposal and analysis of IMP3 expression. Modern Pathology 2010231269–1278. ( 10.1038/modpathol.2010.117) [DOI] [PubMed] [Google Scholar]
- 12.Saglietti C, Onenerk AM, Faquin WC, Sykiotis GP, Ziadi S, Bongiovanni M. FNA diagnosis of poorly differentiated thyroid carcinoma. A review of the recent literature. Cytopathology 201728467–474. ( 10.1111/cyt.12497) [DOI] [PubMed] [Google Scholar]
- 13.Tanaka K, Sonoo H, Saito W, Ohta Y, Shimo T, Sohda M, Yamamoto Y, Kurebayashi J. Analysis of clinical outcome of patients with poorly differentiated thyroid carcinoma. ISRN Endocrinology 20112011308029. ( 10.5402/2011/308029) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bongiovanni M, Sadow PM, Faquin WC. Poorly differentiated thyroid carcinoma: a cytologic-histologic review. Advances in Anatomic Pathology 200916283–289. ( 10.1097/PAP.0b013e3181b50640) [DOI] [PubMed] [Google Scholar]
- 15.Nikiforov YE.Genetic alterations involved in the transition from well-differentiated to poorly differentiated and anaplastic thyroid carcinomas. Endocrine Pathology 200415319–327. ( 10.1385/ep:15:4:319) [DOI] [PubMed] [Google Scholar]
- 16.Shaha AR.Implications of prognostic factors and risk groups in the management of differentiated thyroid cancer. Laryngoscope 2004114393–402. ( 10.1097/00005537-200403000-00001) [DOI] [PubMed] [Google Scholar]
- 17.Volante M, Cavallo GP, Papotti M. Prognostic factors of clinical interest in poorly differentiated carcinomas of the thyroid. Endocrine Pathology 200415313–317. ( 10.1385/ep:15:4:313) [DOI] [PubMed] [Google Scholar]
- 18.Bongiovanni M, Bloom L, Krane JF, Baloch ZW, Powers CN, Hintermann S, Pache JC, Faquin WC. Cytomorphologic features of poorly differentiated thyroid carcinoma: a multi-institutional analysis of 40 cases. Cancer 2009117185–194. ( 10.1002/cncy.20023) [DOI] [PubMed] [Google Scholar]
- 19.Nylén C, Mechera R, Maréchal-Ross I, Tsang V, Chou A, Gill AJ, Clifton-Bligh RJ, Robinson BG, Sywak MS, Sidhu SBet al. Molecular markers guiding thyroid cancer management. Cancers 2020122164. ( 10.3390/cancers12082164) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ibrahimpasic T, Ghossein R, Carlson DL, Chernichenko N, Nixon I, Palmer FL, Lee NY, Shaha AR, Patel SG, Tuttle RMet al. Poorly differentiated thyroid carcinoma presenting with gross extrathyroidal extension: 1986–2009 Memorial Sloan-Kettering Cancer Center experience. Thyroid 201323997–1002. ( 10.1089/thy.2012.0403) [DOI] [PubMed] [Google Scholar]
- 21.Chao TC, Lin JD, Chen MF. Insular carcinoma: infrequent subtype of thyroid cancer with aggressive clinical course. World Journal of Surgery 200428393–396. ( 10.1007/s00268-003-7264-5) [DOI] [PubMed] [Google Scholar]
- 22.Ibrahimpasic T, Ghossein R, Shah JP, Ganly I. Poorly differentiated carcinoma of the thyroid gland: current status and future prospects. Thyroid 201929311–321. ( 10.1089/thy.2018.0509) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hahn SY, Shin JH. Description and comparison of the sonographic characteristics of poorly differentiated thyroid carcinoma and anaplastic thyroid carcinoma. Journal of Ultrasound in Medicine 2016351873–1879. ( 10.7863/ultra.15.09058) [DOI] [PubMed] [Google Scholar]
- 24.Volante M, Landolfi S, Chiusa L, Palestini N, Motta M, Codegone A, Torchio B, Papotti MG. Poorly differentiated carcinomas of the thyroid with trabecular, insular, and solid patterns: a clinicopathologic study of 183 patients. Cancer 2004100950–957. ( 10.1002/cncr.20087) [DOI] [PubMed] [Google Scholar]
- 25.Lloyd RV.WHO Classification of Tumours of Endocrine Organs, 4th ed. Geneva, Switzerland: WHO, 2017. [Google Scholar]
- 26.Volante M, Rapa I, Papotti M. Poorly differentiated thyroid carcinoma: diagnostic features and controversial issues. Endocrine Pathology 200819150–155. ( 10.1007/s12022-008-9040-4) [DOI] [PubMed] [Google Scholar]
- 27.Wong KS, Dong F, Telatar M, Lorch JH, Alexander EK, Marqusee E, Cho NL, Nehs MA, Doherty GM, Afkhami Met al. Papillary thyroid carcinoma with high-grade features versus poorly differentiated thyroid carcinoma: an analysis of clinicopathologic and molecular features and outcome. Thyroid 202131933–940. ( 10.1089/thy.2020.0668) [DOI] [PubMed] [Google Scholar]
- 28.Dettmer M, Schmitt A, Steinert H, Haldemann A, Meili A, Moch H, Komminoth P, Perren A. Poorly differentiated thyroid carcinomas: how much poorly differentiated is needed? American Journal of Surgical Pathology 2011351866–1872. ( 10.1097/PAS.0b013e31822cf962) [DOI] [PubMed] [Google Scholar]
- 29.Bichoo RA, Mishra A, Kumari N, Krishnani N, Chand G, Agarwal G, Agarwal A, Mishra SK. Poorly differentiated thyroid carcinoma and poorly differentiated area in differentiated thyroid carcinoma: is there any difference? Langenbeck’s Archives of Surgery 201940445–53. ( 10.1007/s00423-019-01753-6) [DOI] [PubMed] [Google Scholar]
- 30.Hiltzik D, Carlson DL, Tuttle RM, Chuai S, Ishill N, Shaha A, Shah JP, Singh B, Ghossein RA. Poorly differentiated thyroid carcinomas defined on the basis of mitosis and necrosis: a clinicopathologic study of 58 patients. Cancer 20061061286–1295. ( 10.1002/cncr.21739) [DOI] [PubMed] [Google Scholar]
- 31.Volante M, Lam AK, Papotti M, Tallini G. Molecular pathology of poorly differentiated and anaplastic thyroid cancer: what do pathologists need to know? Endocrine Pathology 20213263–76. ( 10.1007/s12022-021-09665-2) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Jung TS, Kim TY, Kim KW, Oh YL, Park DJ, Cho BY, Shong YK, Kim WB, Park YJ, Jung JHet al. Clinical features and prognostic factors for survival in patients with poorly differentiated thyroid carcinoma and comparison to the patients with the aggressive variants of papillary thyroid carcinoma. Endocrine Journal 200754265–274. ( 10.1507/endocrj.k06-166) [DOI] [PubMed] [Google Scholar]
- 33.Kazaure HS, Roman SA, Sosa JA. Insular thyroid cancer: a population-level analysis of patient characteristics and predictors of survival. Cancer 20121183260–3267. ( 10.1002/cncr.26638) [DOI] [PubMed] [Google Scholar]
- 34.Rufini V, Salvatori M, Fadda G, Pinnarelli L, Castaldi P, Maussier ML, Galli G. Thyroid carcinomas with a variable insular component: prognostic significance of histopathologic patterns. Cancer 20071101209–1217. ( 10.1002/cncr.22913) [DOI] [PubMed] [Google Scholar]
- 35.Basolo F, Pisaturo F, Pollina LE, Fontanini G, Elisei R, Molinaro E, Iacconi P, Miccoli P, Pacini F. N-ras mutation in poorly differentiated thyroid carcinomas: correlation with bone metastases and inverse correlation to thyroglobulin expression. Thyroid 20001019–23. ( 10.1089/thy.2000.10.19) [DOI] [PubMed] [Google Scholar]
- 36.Nilsson JN, Siikanen J, Hedman C, Juhlin CC, Ihre Lundgren C. Pre-therapeutic measurements of iodine avidity in papillary and poorly differentiated thyroid cancer reveal associations with thyroglobulin expression, histological variants and Ki-67 index. Cancers 2021133627. ( 10.3390/cancers13143627) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lai WA, Hang JF, Liu CY, Bai Y, Liu Z, Gu H, Hong S, Pyo JY, Jung CK, Kakudo Ket al. PAX8 expression in anaplastic thyroid carcinoma is less than those reported in early studies: a multi-institutional study of 182 cases using the monoclonal antibody MRQ-50. Virchows Archiv 2020476431–437. ( 10.1007/s00428-019-02708-4) [DOI] [PubMed] [Google Scholar]
- 38.Rocha AS, Soares P, Fonseca E, Cameselle-Teijeiro J, Oliveira MC, Sobrinho-Simões M. E-cadherin loss rather than beta-catenin alterations is a common feature of poorly differentiated thyroid carcinomas. Histopathology 200342580–587. ( 10.1046/j.1365-2559.2003.01642.x) [DOI] [PubMed] [Google Scholar]
- 39.Patel KN, Shaha AR. Poorly differentiated thyroid cancer. Current Opinion in Otolaryngology and Head and Neck Surgery 201422121–126. ( 10.1097/MOO.0000000000000037) [DOI] [PubMed] [Google Scholar]
- 40.Paulsson JO, Backman S, Wang N, Stenman A, Crona J, Thutkawkorapin J, Ghaderi M, Tham E, Stålberg P, Zedenius Jet al. Whole-genome sequencing of synchronous thyroid carcinomas identifies aberrant DNA repair in thyroid cancer dedifferentiation. Journal of Pathology 2020250183–194. ( 10.1002/path.5359) [DOI] [PubMed] [Google Scholar]
- 41.Cancer Genome Atlas Research Network. Integrated genomic characterization of papillary thyroid carcinoma. Cell 2014159676–690. ( 10.1016/j.cell.2014.09.050) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Nikiforov YE.Thyroid carcinoma: molecular pathways and therapeutic targets. Modern Pathology 200821 (Supplement 2) S37–S43. ( 10.1038/modpathol.2008.10) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Nikiforova MN, Nikiforov YE. Molecular genetics of thyroid cancer: implications for diagnosis, treatment and prognosis. Expert Review of Molecular Diagnostics 2008883–95. ( 10.1586/14737159.8.1.83) [DOI] [PubMed] [Google Scholar]
- 44.Landa I, Ibrahimpasic T, Boucai L, Sinha R, Knauf JA, Shah RH, Dogan S, Ricarte-Filho JC, Krishnamoorthy GP, Xu Bet al. Genomic and transcriptomic hallmarks of poorly differentiated and anaplastic thyroid cancers. Journal of Clinical Investigation 20161261052–1066. ( 10.1172/JCI85271) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell 2011144646–674. ( 10.1016/j.cell.2011.02.013) [DOI] [PubMed] [Google Scholar]
- 46.Bell RJA, Rube HT, Kreig A, Mancini A, Fouse SD, Nagarajan RP, Choi S, Hong C, He D, Pekmezci Met al. Cancer. The transcription factor GABP selectively binds and activates the mutant tert promoter in cancer. Science 20153481036–1039. ( 10.1126/science.aab0015) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hannallah J, Rose J, Guerrero MA. Comprehensive literature review: recent advances in diagnosing and managing patients with poorly differentiated thyroid carcinoma. International Journal of Endocrinology 20132013317487. ( 10.1155/2013/317487) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Sobrinho-Simões M, Máximo V, Rocha AS, Trovisco V, Castro P, Preto A, Lima J, Soares P. Intragenic mutations in thyroid cancer. Endocrinology and Metabolism Clinics of North America 200837333–36, viii. ( 10.1016/j.ecl.2008.02.004) [DOI] [PubMed] [Google Scholar]
- 49.Chernock RD, Rivera B, Borrelli N, Hill DA, Fahiminiya S, Shah T, Chong AS, Aqil B, Mehrad M, Giordano TJet al. Poorly differentiated thyroid carcinoma of childhood and adolescence: a distinct entity characterized by DICER1 mutations. Modern Pathology 2020331264–1274. ( 10.1038/s41379-020-0458-7) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ibrahimpasic T, Ghossein R, Carlson DL, Nixon I, Palmer FL, Shaha AR, Patel SG, Tuttle RM, Shah JP, Ganly I. Outcomes in patients with poorly differentiated thyroid carcinoma. Journal of Clinical Endocrinology and Metabolism 2014991245–1252. ( 10.1210/jc.2013-3842) [DOI] [PubMed] [Google Scholar]
- 51.Wong KS, Lorch JH, Alexander EK, Marqusee E, Cho NL, Nehs MA, Doherty GM, Barletta JA. Prognostic significance of extent of invasion in poorly differentiated thyroid carcinoma. Thyroid 2019291255–1261. ( 10.1089/thy.2019.0263) [DOI] [PubMed] [Google Scholar]
- 52.Fu H, Sa R, Cheng L, Jin Y, Qiu X, Liu M, Chen L. Updated review of nuclear molecular imaging of thyroid cancers. Endocrine Practice 202127494–502. ( 10.1016/j.eprac.2020.10.001) [DOI] [PubMed] [Google Scholar]
- 53.Wang W, Larson SM, Fazzari M, Tickoo SK, Kolbert K, Sgouros G, Yeung H, Macapinlac H, Rosai J, Robbins RJ. Prognostic value of [18F]fluorodeoxyglucose positron emission tomographic scanning in patients with thyroid cancer. Journal of Clinical Endocrinology and Metabolism 2000851107–1113. ( 10.1210/jcem.85.3.6458) [DOI] [PubMed] [Google Scholar]
- 54.Wang W, Macapinlac H, Larson SM, Yeh SD, Akhurst T, Finn RD, Rosai J, Robbins RJ. [18F]-2-Fluoro-2-deoxy-D-glucose positron emission tomography localizes residual thyroid cancer in patients with negative diagnostic (131)I whole body scans and elevated serum thyroglobulin levels. Journal of Clinical Endocrinology and Metabolism 1999842291–2302. ( 10.1210/jcem.84.7.5827) [DOI] [PubMed] [Google Scholar]
- 55.Civan C, Isik EG, Simsek DH. Metastatic poorly differentiated thyroid cancer with heterogeneous distribution of 18F-FDG,68Ga-DOTATATE, and 68Ga-PSMA on PET/CT. Clinical Nuclear Medicine 202146e212–e213. ( 10.1097/RLU.0000000000003362) [DOI] [PubMed] [Google Scholar]
- 56.Lin JD, Chao TC, Hsueh C. Clinical characteristics of poorly differentiated thyroid carcinomas compared with those of classical papillary thyroid carcinomas. Clinical Endocrinology 200766224–228. ( 10.1111/j.1365-2265.2006.02712.x) [DOI] [PubMed] [Google Scholar]
- 57.Yu MG, Rivera J, Jimeno C. Poorly differentiated thyroid carcinoma: 10-year experience in a Southeast Asian population. Endocrinology and Metabolism 201732288–295. ( 10.3803/EnM.2017.32.2.288) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Walczyk A, Kowalska A, Sygut J. The clinical course of poorly differentiated thyroid carcinoma (insular carcinoma) – own observations. Endokrynologia Polska 201061467–473. [PubMed] [Google Scholar]
- 59.Lai HW, Lee CH, Chen JY, Tseng LM, Yang AH. Insular thyroid carcinoma: collective analysis of clinicohistologic prognostic factors and treatment effect with radioiodine or radiation therapy. Journal of the American College of Surgeons 2006203715–722. ( 10.1016/j.jamcollsurg.2006.07.008) [DOI] [PubMed] [Google Scholar]
- 60.Siironen P, Hagström J, Mäenpää HO, Louhimo J, Heikkilä A, Heiskanen I, Arola J, Haglund C. Anaplastic and poorly differentiated thyroid carcinoma: therapeutic strategies and treatment outcome of 52 consecutive patients. Oncology 201079400–408. ( 10.1159/000322640) [DOI] [PubMed] [Google Scholar]
- 61.Cherkaoui GS, Guensi A, Taleb S, Idir MA, Touil N, Benmoussa R, Baroudi Z, Chikhaoui N. Poorly differentiated thyroid carcinoma: a retrospective clinicopathological study. Pan African Medical Journal 201521 137. ( 10.11604/pamj.2015.21.137.6720) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Sanders EM, LiVolsi VA, Brierley J, Shin J, Randolph GW. An evidence-based review of poorly differentiated thyroid cancer. World Journal of Surgery 200731934–945. ( 10.1007/s00268-007-9033-3) [DOI] [PubMed] [Google Scholar]
- 63.American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini Fet al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009191167–1214. ( 10.1089/thy.2009.0110) [DOI] [PubMed] [Google Scholar]
- 64.Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger Met al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016261–133. ( 10.1089/thy.2015.0020) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Sa R, Cheng L, Jin Y, Fu H, Shen Y, Chen L. Distinguishing patients with distant metastatic differentiated thyroid cancer who biochemically benefit from next radioiodine treatment. Frontiers in Endocrinology 202011587315. ( 10.3389/fendo.2020.587315) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Zhang M, Lei S, Chen Y, Wu Y, Ye H. The role of lymph node status in cancer-specific survival and decision-making of postoperative radiotherapy in poorly differentiated thyroid cancer: a population-based study. American Journal of Translational Research 202113383–390. [PMC free article] [PubMed] [Google Scholar]
- 67.Rosenbluth BD, Serrano V, Happersett L, Shaha AR, Tuttle RM, Narayana A, Wolden SL, Rosenzweig KE, Chong LM, Lee NY. Intensity-modulated radiation therapy for the treatment of nonanaplastic thyroid cancer. International Journal of Radiation Oncology, Biology, Physics 2005631419–1426. ( 10.1016/j.ijrobp.2005.05.043) [DOI] [PubMed] [Google Scholar]
- 68.Yang H, Chen Z, Wu M, Lei T, Yu H, Ge M. Remarkable response in 2 cases of advanced poorly differentiated thyroid carcinoma with liposomal doxorubicin plus cisplatin. Cancer Biology and Therapy 201617693–697. ( 10.1080/15384047.2016.1167295) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Nutting CM, Convery DJ, Cosgrove VP, Rowbottom C, Vini L, Harmer C, Dearnaley DP, Webb S. Improvements in target coverage and reduced spinal cord irradiation using intensity-modulated radiotherapy (IMRT) in patients with carcinoma of the thyroid gland. Radiotherapy and Oncology 200160173–180. ( 10.1016/s0167-8140(0100382-6) [DOI] [PubMed] [Google Scholar]
- 70.Asakawa H, Kobayashi T, Komoike Y, Maruyama H, Nakano Y, Tamaki Y, Matsuzawa Y, Monden M. Chemosensitivity of anaplastic thyroid carcinoma and poorly differentiated thyroid carcinoma. Anticancer Research 1997172757–2762. [PubMed] [Google Scholar]
- 71.Auersperg M, Us-Krasovec M, Petric G, Pogacnik A, Besic N. Results of combined modality treatment in poorly differentiated and anaplastic thyroid carcinoma. Wiener klinische Wochenschrift 1990102267–270. [PubMed] [Google Scholar]
- 72.Crouzeix G, Michels JJ, Sevin E, Aide N, Vaur D, Bardet S. & French TUTHYREF network. Unusual short-term complete response to two regimens of cytotoxic chemotherapy in a patient with poorly differentiated thyroid carcinoma. Journal of Clinical Endocrinology and Metabolism 2012973046–3050. ( 10.1210/jc.2012-1630) [DOI] [PubMed] [Google Scholar]
- 73.Jin Y, Van Nostrand D, Cheng L, Liu M, Chen L. Radioiodine refractory differentiated thyroid cancer. Critical Reviews in Oncology/Hematology 2018125111–120. ( 10.1016/j.critrevonc.2018.03.012) [DOI] [PubMed] [Google Scholar]
- 74.Cabanillas ME, Habra MA. Lenvatinib: role in thyroid cancer and other solid tumors. Cancer Treatment Reviews 20164247–55. ( 10.1016/j.ctrv.2015.11.003) [DOI] [PubMed] [Google Scholar]
- 75.Duo LJ, Rong J, Bin W, Hua MC, Wei SL, Yuan LV. Transient partial response of poorly-differentiated thyroid carcinoma to sunitinib treatment: a case report. Oncology Letters 201510492–496. ( 10.3892/ol.2015.3174) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Landriscina M, Maddalena F, Fabiano A, Piscazzi A, La Macchia O, Cignarelli M. Erlotinib enhances the proapoptotic activity of cytotoxic agents and synergizes with paclitaxel in poorly-differentiated thyroid carcinoma cells. Anticancer Research 201030473–480. [PubMed] [Google Scholar]
- 77.Gay S, Monti E, Trambaiolo Antonelli C, Mora M, Spina B, Ansaldo G, Teliti M, Comina M, Conte L, Minuto Met al. Case report: lenvatinib in neoadjuvant setting in a patient affected by invasive poorly differentiated thyroid carcinoma. Future Oncology 20191513–19. ( 10.2217/fon-2019-0099) [DOI] [PubMed] [Google Scholar]
- 78.Dierks C, Seufert J, Aumann K, Ruf J, Klein C, Kiefer S, Rassner M, Boerries M, Zielke A, la Rosee Pet al. Combination of lenvatinib and pembrolizumab is an effective treatment option for anaplastic and poorly differentiated thyroid carcinoma. Thyroid 2021311076–1085. ( 10.1089/thy.2020.0322) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Cheng L, Fu H, Jin Y, Sa R, Chen L. Clinicopathological features predict outcomes in patients with radioiodine-refractory differentiated thyroid cancer treated with sorafenib: a real-world study. Oncologist 202025e668–e678. ( 10.1634/theoncologist.2019-0633) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Short SC, Suovuori A, Cook G, Vivian G, Harmer C. A phase II study using retinoids as redifferentiation agents to increase iodine uptake in metastatic thyroid cancer. Clinical Oncology 200416569–574. ( 10.1016/j.clon.2004.06.018) [DOI] [PubMed] [Google Scholar]
- 81.Kebebew E, Lindsay S, Clark OH, Woeber KA, Hawkins R, Greenspan FS. Results of rosiglitazone therapy in patients with thyroglobulin-positive and radioiodine-negative advanced differentiated thyroid cancer. Thyroid 200919953–956. ( 10.1089/thy.2008.0371) [DOI] [PubMed] [Google Scholar]
- 82.Hong CM, Ahn BC. Redifferentiation of radioiodine refractory differentiated thyroid cancer for reapplication of I-131 therapy. Frontiers in Endocrinology 20178 260. ( 10.3389/fendo.2017.00260) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Leboulleux S, Dupuy C, Lacroix L, Attard M, Grimaldi S, Corre R, Ricard M, Nasr S, Berdelou A, Hadoux Jet al. Redifferentiation of a BRAF(K601E)-mutated poorly differentiated thyroid cancer patient with dabrafenib and trametinib treatment. Thyroid 201929735–742. ( 10.1089/thy.2018.0457) [DOI] [PubMed] [Google Scholar]
- 84.Ho AL, Grewal RK, Leboeuf R, Sherman EJ, Pfister DG, Deandreis D, Pentlow KS, Zanzonico PB, Haque S, Gavane Set al. Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer. New England Journal of Medicine 2013368623–632. ( 10.1056/NEJMoa1209288) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Groussin L, Clerc J, Huillard O. Larotrectinib-enhanced radioactive iodine uptake in advanced thyroid cancer. New England Journal of Medicine 20203831686–1687. ( 10.1056/NEJMc2023094) [DOI] [PubMed] [Google Scholar]
- 86.Wächter S, Damanakis AI, Elxnat M, Roth S, Wunderlich A, Verburg FA, Fellinger SA, Bartsch DK, Di Fazio P. Epigenetic modifications in thyroid cancer cells restore NIS and radio-iodine uptake and promote cell death. Journal of Clinical Medicine 2018761. ( 10.3390/jcm7040061) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Chen M, Wei L, Law CT, Tsang FH, Shen J, Cheng CL, Tsang LH, Ho DW, Chiu DK, Lee JMet al. RNA N6-methyladenosine methyltransferase-like 3 promotes liver cancer progression through YTHDF2-dependent posttranscriptional silencing of SOCS2. Hepatology 2018672254–2270. ( 10.1002/hep.29683) [DOI] [PubMed] [Google Scholar]
- 88.Tang Y, Meng X, Yu X, Shang H, Chen S, Liao L, Dong J. Inhibition of microRNA-875-5p promotes radioiodine uptake in poorly differentiated thyroid carcinoma cells by upregulating sodium-iodide symporter. Journal of Endocrinological Investigation 202043439–450. ( 10.1007/s40618-019-01125-3) [DOI] [PubMed] [Google Scholar]
- 89.Dunn LA, Sherman EJ, Baxi SS, Tchekmedyian V, Grewal RK, Larson SM, Pentlow KS, Haque S, Tuttle RM, Sabra MMet al. Vemurafenib redifferentiation of BRAF mutant, RAI-refractory thyroid cancers. Journal of Clinical Endocrinology and Metabolism 20191041417–1428. ( 10.1210/jc.2018-01478) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Wang Q, Wu X. Primary and acquired resistance to PD-1/PD-L1 blockade in cancer treatment. International Immunopharmacology 201746210–219. ( 10.1016/j.intimp.2017.03.015) [DOI] [PubMed] [Google Scholar]
- 91.Rosenbaum MW, Gigliotti BJ, Pai SI, Parangi S, Wachtel H, Mino-Kenudson M, Gunda V, Faquin WC. PD-L1 and IDO1 are expressed in poorly differentiated thyroid carcinoma. Endocrine Pathology 20182959–67. ( 10.1007/s12022-018-9514-y) [DOI] [PMC free article] [PubMed] [Google Scholar]