
FIGURE 2.
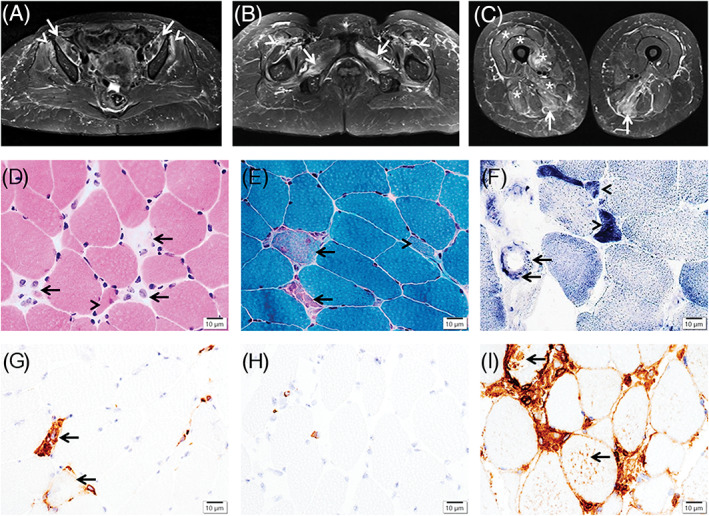
Magnetic resonance imaging of the thigh muscles and immune‐mediated necrotizing myopathy pathology. Axial short‐tau inversion recovery images demonstrate increased signal intensity in the bilateral iliopsoas (A) (arrows), gluteus minimus (A) (arrowheads), adductors and obturator externus (B) (arrows), and semimembranosus (C) (arrows) muscles, and mild intermuscular edema between the rectus femoris and vastus lateralis (B) (arrowheads), with milder involvement of the left vastus medialis, intermedius, and lateralis, as well as right adductor magnus and biceps femoris (C) (asterisk). The vastus lateralis muscle biopsy shows necrotic myofibers in (D) (hematoxylin‐eosin stain) and (E) (Gomori trichrome stain) (arrows), regenerating myofibers in (D‐F) (arrowheads), and capillary endothelial cells containing positive granules in (F) (succinate dehydrogenase stain) (arrows), scattered to aggregated CD68+ macrophages in (G) (arrows), rare CD8+ T cells in (H), and major histocompatibility complex‐1 expression extensively in the necrotic myofibers and focally in some non‐necrotic myofibers in (I) (arrows). Scale bars = 10 μm in (D‐I)