
Figure 1.
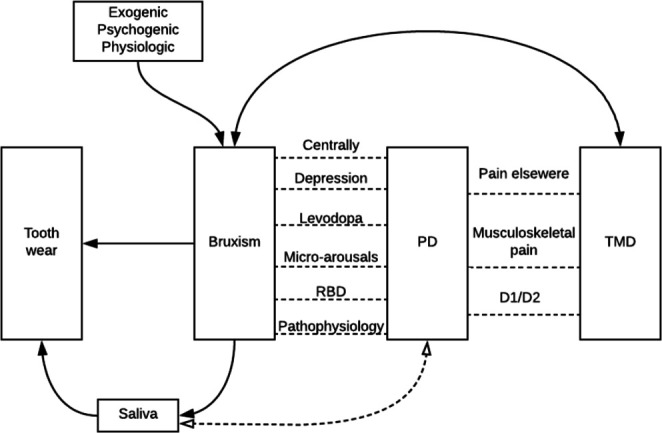
Visualisation of the possible interactions between the different research variables. Parkinson’s disease (PD) is associated with bruxism through different variables: the dopaminergic system (pathophysiology) plays a role in both PD and bruxism; the prodromal phase of PD (RBD) shows the same characteristics during sleep as does bruxism; sleep disturbances lead to micro-arousals that can lead to bruxism; dopaminergic medication (levodopa) can influence bruxism; depression is one of the risk factors for bruxism and is more prevalent in patients with PD and finally, both PD and bruxism are regulated centrally and not peripherally. PD is also associated with temporomandibular disorders (TMD): patients with PD experience pain in the entire body (ie, widespread pain), which is a risk factor for TMD pain; also, musculoskeletal pain (as in TMD pain) is frequently present and finally, alterations in the striatal dopaminergic system (D1/D2 ratio) could play a role in TMD pain. Bruxism itself is a risk factor for TMD pain and vice versa. Besides, tooth wear can be a consequence of bruxism. When bruxism occurs, saliva can be increased, which can be a protective factor for tooth wear. Also, saliva can be changed due to PD medication. Finally, several exogenic, psychogenic and physiological factors can be a risk for bruxism.