
Figure 2.
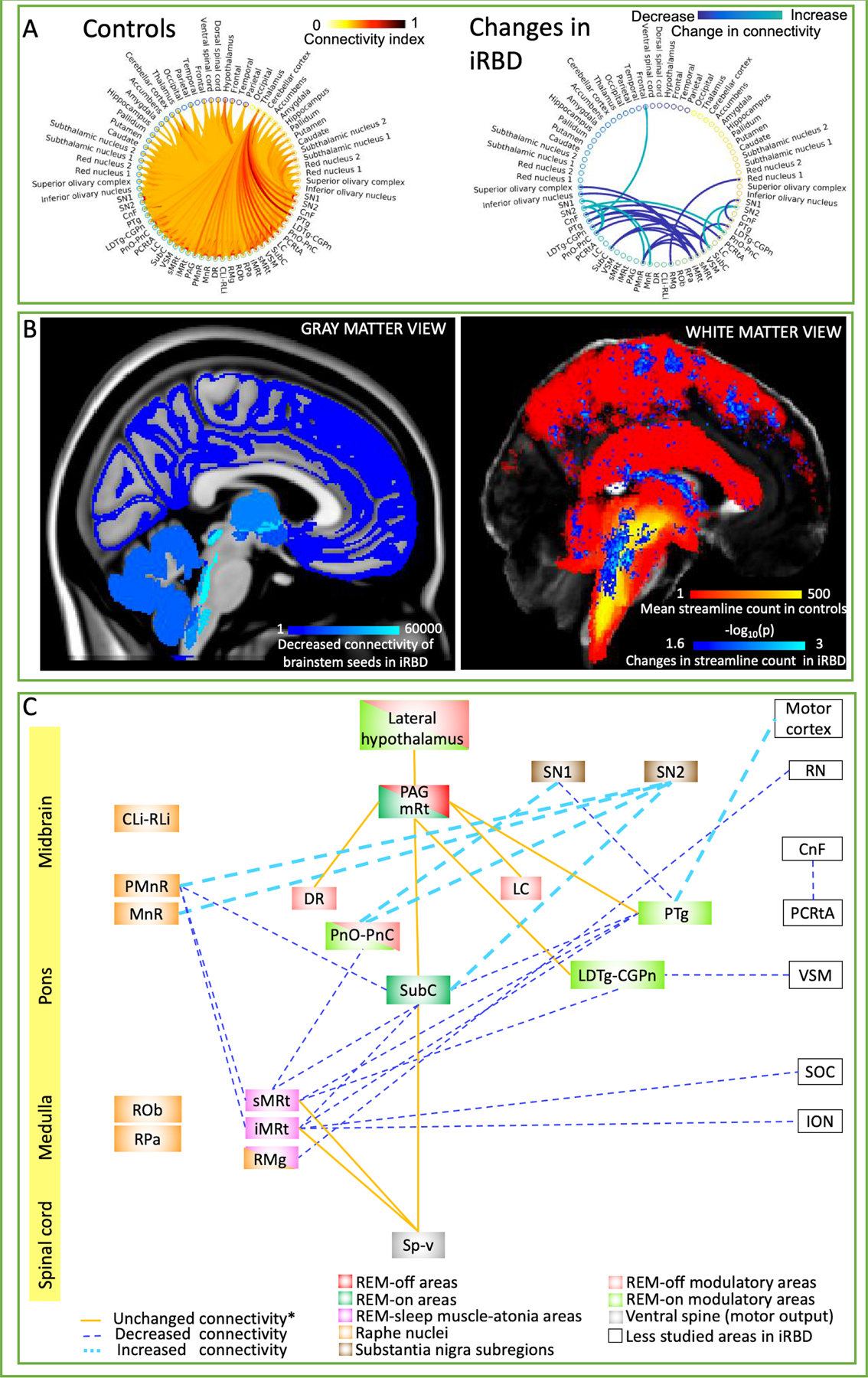
A) Left: Structural tractography-based connectome of 20 brainstem nuclei relevant for iRBD/premanifest synucleinopathy (list of nuclei shown in Fig. 1A) in controls (average connectivity index across 12 controls displayed). Right: Statistically significant differences in structural connectivity between iRBD patients and controls (Wilcoxon test, p < 0.01, n = 12); note that, except for a significant link with the frontal cortex, alterations of connectivity pathways in iRBD occurred exclusively within brainstem nuclei. Specifically, PnO-PnC and SN showed increased reciprocal connectivity bilaterally, as well as PMnR and MnR to SN subregion 2 in the left hemisphere. In the right hemisphere iMRt, sMRt and SubC showed decreased connectivity with PMnR and contralateral PTg and SubC among other nuclei in iRBD compared to controls. Further, other nuclei such as VSM, PTg, PCRtA (on the right hemisphere) and RMg showed decreased connectivity with ipsilateral LDTg-CGPn, ipsilateral SN subregion 1, contralateral CnF and right RN subregion 1 respectively. PTg on the left hemisphere showed increased connectivity with ipsilateral frontal cortical areas (including central and paracentral gyrus) in iRBD compared to controls. B) Left: Pictorial summary of the decreased structural connectivity changes in iRBD patients in target gray matter regions overlaid on MNI-space. Count of decreased streamlines reaching each target region (cortical and subcortical, including brainstem nuclei), when propagated by any of our 20 brainstem nuclei seeds. Right: Pictorial view of white matter changes in iRBD versus controls. In red-yellow, the mean tract density in controls of all the brainstem nuclei relevant for iRBD/premanifest synucleinopathy. In blue-light blue, changes (both increases and decreases) in streamline count between iRBD and controls (Wilcoxon test, p < 0.05 uncorrected for multiple comparisons, 14 brainstem seeds) overlaid on a FA-MNI-template. C) Diagram summarizing the structural connectivity changes in iRBD human subjects in the present study. The iRBD relevant nuclei/regions were color-coded based on their functions as previously reported in animal and human lesion studies of non-idiopathic RBD.3,11,17 Note that further studies are needed with regard to the homology of these anatomical areas between human and animal models. Unchanged structural connectivity between groups (indicated with *) among nuclei has been simplified to only display relevant connections for iRBD based on animal studies.3,12 Notably, decreased structural connectivity (possibly indicating neurodegenerative mechanisms) mainly occurred in ponto-medullary brainstem nuclei previously postulated to be involved in REM atonia,11 while increased connectivity (possibly indicating compensatory mechanisms) was found in meso-pontine brainstem nuclei. Moreover, the direct pathway between SubC and the spinal cord was preserved, while the indirect pathway through the medullary reticular formation (sMRt, iMRt) displayed decreased connectivity. Interestingly, REM-off areas (PAG, mRt (mesencephalic reticular formation), DR, LC and lateral hypothalamus) mostly did not show differences in connectivity between groups. Rather, our results showed mainly impaired connectivity in iRBD between REM-on (SubC, PnO, and REM-on modulatory areas LDTg and PTg) and REM-sleep muscle-atonia areas (mainly the medullary reticular formation nuclei sMRt, iMRt).