
Figure 5.
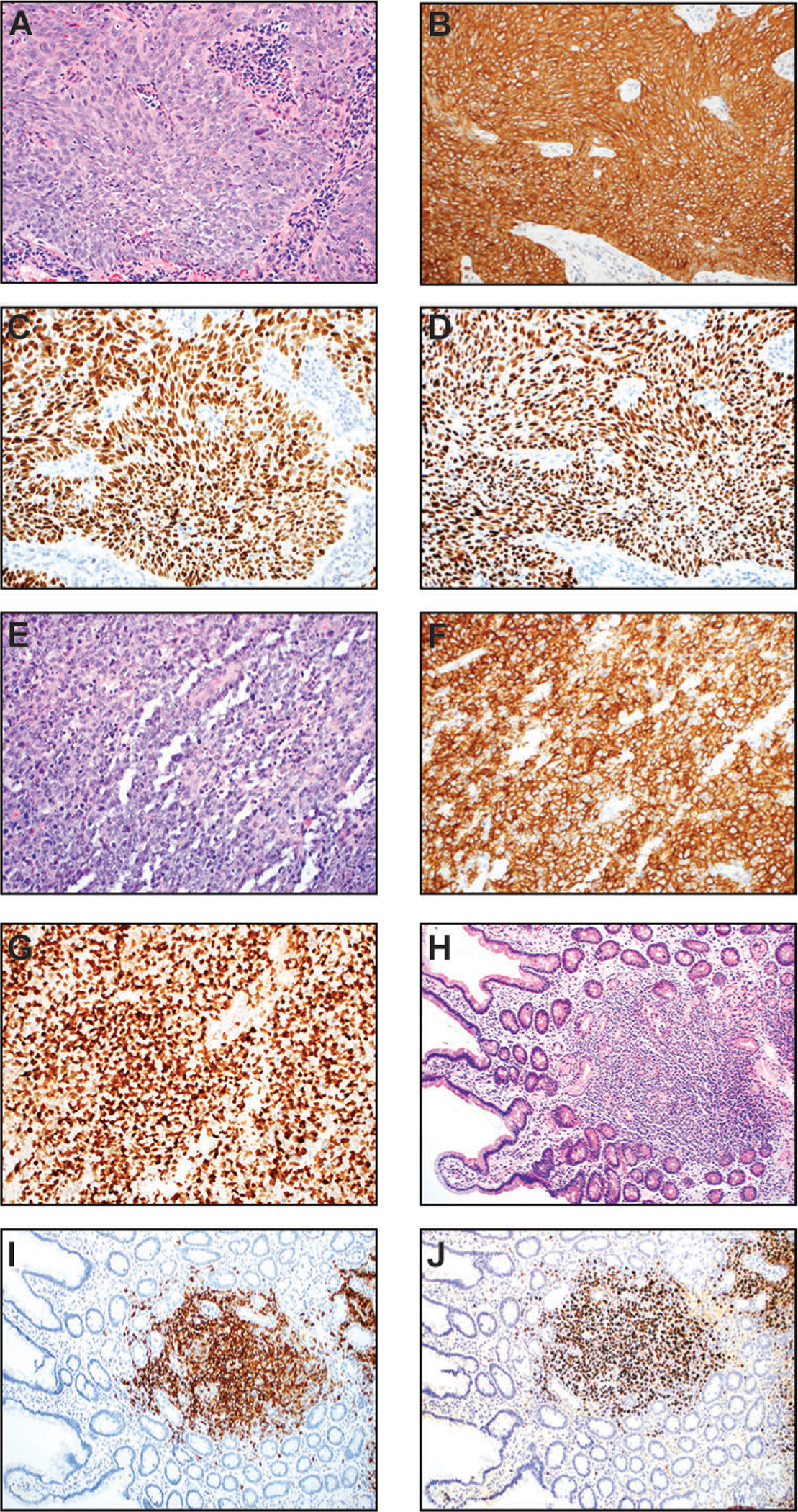
Nasopharyngeal carcinoma (NPC) (A-D) and posttransplant lymphoproliferative disorder (PTLD) (E-J). (A) In this medium power H&E image (200x), the NPC grows in syncytial nests and show a spindled cell morphology. The neoplastic cells are large with oval nuclei, vesicular chromatin, and prominent nucleoli. (B) CK5/6 immunostain (200x) is diffusely and strongly positive in tumor cells, supporting squamous differentiation. (C) EBV-encoded small RNA (200x) is virtually positive in all tumor nuclei. (D) The tumor nuclei are also diffusely and strongly positive for p63, another squamous cell marker (200x). (E-G): Monomorphic PTLD (diffuse large B-cell lymphoma type) in the central nervous system of a patient with prior renal transplant (15 years ago). (E) H&E (200x) shows a diffuse infiltrate of atypical large lymphoid cells with vesicular chromatin. Abundant apoptotic debris and mitotic figures are present. (F) CD20 immunostain (200x) confirms B-cell origin and large cell sizes. (G) Ki-67 (200x) immunohistochemistry highlights numerous neoplastic lymphoid cells with a very high proliferation index. (H-J) Duodenal polymorphic PTLD in a patient who had multiple stem cell transplants. (H) H&E section at a low power magnification (100x) shows mucosal involvement by a mixed hematolymphoid infiltrate. (I) CD20 (100x) demonstrates that the majority of cells are B-cells with variable sizes. (J) In situ hybridization for EBV-encoded small RNA (100x) highlights numerous EBV-positive lymphoid cells.