
Figure 6.
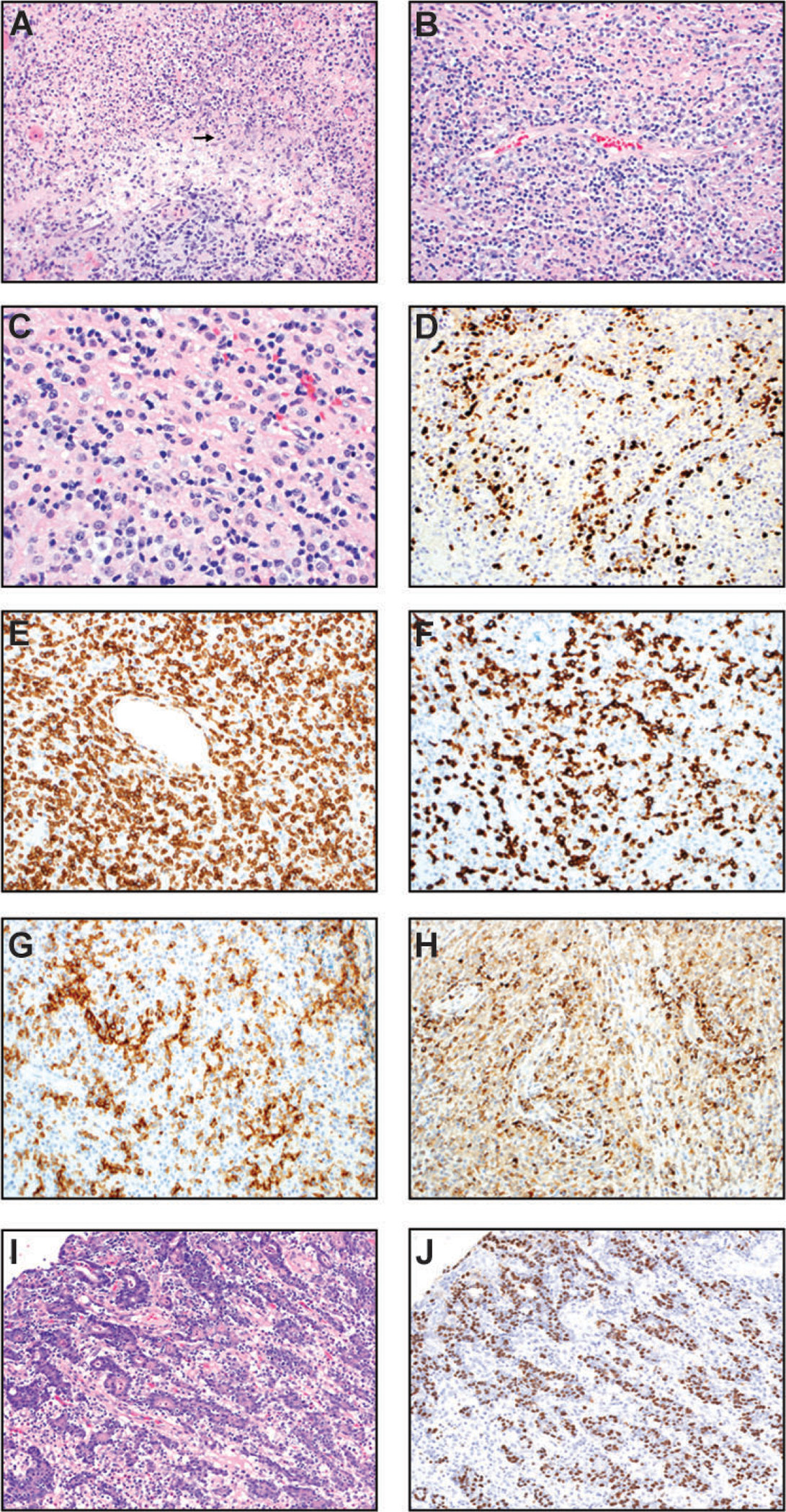
Extranodal natural killer (NK)/T cell lymphoma, nasal type (A-H) and gastric carcinoma associated with EBV (I-J). (A & B) H&E sections (200x) show angiodestruction by invading lymphoma cells with associated necrosis and karyorrhectic debris (arrow in Panel A). (C) In this high-power H&E image (400x), most lymphoma cells are small to intermediate-sized with irregular nuclear contours/folds. Many cells possess moderate amounts of clear/vacuolated cytoplasm. (D) In situ hybridization for EBV-encoded RNA (200x) is positive in the nuclei of most lymphoma cells. (E) CD3 (200x) demonstrates that the majority of the lymphoid infiltrate is T cells. (F) CD8 immunostain is positive in the neoplastic T cells with angiocentric pattern (200x). (G) CD56 immunostain highlights the angiocentric lymphoma cells (200x). (H) TIA-1 immunostain highlights the angiocentric lymphoma cells. (I-J) Gastric carcinoma associated with EBV: Gastric carcinoma with lymphoid stroma. (I) H&E (200x) slide shows epithelioid tumor cells in fused glands and cords. There are intraepithelial lymphocytes as well as mature lymphocytes scattered in the background. (J) In situ hybridization for EBV-encoded RNA (200x) is positive in the nuclei of the neoplastic epithelial cells but not the background lymphocytes.