

Abstract
Intentional and unintentional firearm injury is the second leading cause of death for youth, underscoring the need for effective primary prevention approaches that focus on increasing safe storage by caregivers and decreasing handling/carriage among youth. This article describes the state of the science for prevention of firearm injuries among children and adolescents. We applied PRISMA guidelines to present results from a scoping review using PubMed, Scopus, CINAHL, and CJ Abstracts for original research articles published between January 1, 1985 and March 1, 2018 in the U.S. focusing on primary screening or interventions for primary prevention of pediatric firearm injuries. In total, 46 articles met inclusion criteria: safe storage (23), screening (2), firearm handling/carriage/use (21). Across school, healthcare, and community settings, few evidenced-based programs exist, and data on firearm safety technologies are lacking. Programs have generally not employed rigorous designs, and/or assessed behavioral (e.g., carriage) or injury-related firearm outcomes. Evidenced-based prevention programs are needed to mitigate firearm morbidity and mortality among youth.
Keywords: Universal prevention, Primary prevention, Firearm injury, Safe storage, Firearm carriage, Children, Adolescents
Background
Firearm-related injuries are the second leading cause of deaths among children and adolescents in the U.S. (Cunningham et al., 2018), with the majority of fatalities involving a handgun (Fowler et al., 2017). Among adolescents, homicide and suicide are the leading causes of firearm injuries and death (Fowler et al., 2017; Reich et al., 2002), whereas unintentional firearm injuries are more common among younger children. Younger children are also more likely than adolescents to be killed in incidents related to intimate partner violence (IPV; Fowler et al., 2017). Overall, firearm-related homicide rates among Black children are greater than 10 times the rates among White children or among Asian children (Fowler et al., 2017). In contrast, firearm-related suicide fatalities among White children and among First Nations children are 4–5 times higher than among Black, Asian, or Hispanic children (Fowler et al., 2017). This firearm-related morbidity among youth underscores the urgent need for evidenced-based prevention approaches to decrease firearm handling (e.g. playing with a found gun), carriage (e.g., bringing a gun to school, carrying a gun while out with friends), or use among children and adolescents; one primary way of doing this is by increasing safe storage of firearms by caregivers (e.g., use of gun safe or gun lock, bullets stored separately).
Recent reviews underscore high regional variability in estimates of the presence of guns in U.S. homes (Parikh et al., 2017), with less than 50% being stored safely (e.g., locked and unloaded; (Rowhani-Rahbar et al., 2016; Scott et al., 2018). The need to increase safe storage and prevent access by youth is further underscored for families of youth at risk for suicide, given that one-third of parents of children with a history of self-harm stored guns unlocked and unloaded (Scott et al., 2018). Moreover, one-third of adolescents report access to a handgun (Loh et al., 2010), highlighting the need to encourage safe storage and to decrease handling, carriage and use among adolescents as well as children.
The first step in establishing recommendations for primary prevention strategies (defined as interventions delivered to broad groups of individuals prior to injury) to reduce firearm access among youth (e.g., increase safe storage of all firearms, decrease handling/carriage among youth) requires understanding the current state of the science across foci of interventions (individual, family, and community level; firearm safety technology) and settings (e.g., homes, schools, healthcare, community). Prior reviews of the firearm literature, focusing on epidemiology and risk/protective factors (Crossen et al., 2015; Dowd, 1999; Fein & Mollen, 1999; Komro, 1999; Parikh et al., 2017; Williamson et al., 2014), recommend additional research to identify effective prevention approaches to reduce youth access to firearms (Parikh et al., 2017). Further, these reviews conclude that screening for firearms in the home, and counseling to increase safe storage, inconsistently occurs in healthcare settings (Roszko et al., 2016). For example, data from the American Academy of Pediatrics shows that only 21% of pediatricians “Always” try to identify families who have firearms in the homes (American Academy of Pediatrics, 2016). Nonetheless, counseling is effective in improving safe storage when combined with providing a firearm safe storage device (e.g., trigger locks which prevents the gun from being fired; (Rowhani-Rahbar et al., 2016). Of note, previous literature reviews have neither examined firearm handling, carriage, use, nor safe storage intervention efforts across multiple community settings (e.g., schools, healthcare, community centers and/or community-level).
This review describes the extant research literature pertaining to primary prevention strategies to reduce firearm access by children and adolescents under 18 years of age, exemplifying how these prevention efforts can be done without conflict with the Second Amendment and the legal rights of adults to own firearms. It is important to mention that there are no restrictions on physicians in asking and counseling about firearm storage (Rivara & Fan, 2017). Hereafter, the term children will refer to youth 0–9 years of age (e.g., preschool and elementary) and the term adolescents will refer to those between 10 and 17 years of age (e.g., middle and high school). Specifically, we conducted a scoping review to identify gaps in this literature for the purpose of informing future prevention and intervention work in child and adolescent firearm injuries. This review focuses on screening tools and interventions for: (1) safe storage and (2) firearm handling, carriage, and use.
Methods
We applied the 5-step scoping review method (Arksey & O’Malley, 2005) and utilized the PRISMA framework for reporting standards (Moher et al., 2009), which includes: (1) identifying the research question; (2) identifying relevant studies; (3) selecting studies; (4) charting the data; and (5) collating, summarizing and reporting results. We used the findings from the scoping review to establish recommendations for research and intervention to address current gaps in the science.
Literature search strategies
We conducted a scoping review using PubMed, Scopus, CINAHL, CJ Abstracts for English-language original research articles published between January, 1985 and March, 2018 on primary prevention of youth firearm related outcomes in the U.S. The initial comprehensive search was created in PubMed and subsequently duplicated in other databases. Searches combined keywords including firearm, firearm carriage, ownership, unintentional injury, intentional injury, self-inflicted injuries, youth, child, and adolescent. (See “Appendix” for example list of PubMed search terms). Citation tracking was conducted using the EndNote citation management software for articles that met inclusion criteria.
Eligibility criteria
Articles were eligible if the sample included youth (ages 0–17), or if the sample was of comprised parents/caregivers of youth. Articles were not included if they were a literature review of empirical articles, or non-empirical recommendations, such as opinion/perspective pieces or professional society statements. Also, we excluded studies for these reasons: international and non-English articles; were not focused on 0–17 year olds; articles without specific focus on firearms (e.g., general violence interventions without mention of firearm criteria in the title or abstract, intervention components or outcomes); could not obtain the abstract/article; and non-primary or non-universal prevention intervention articles (e.g., focused on epidemiology, risk/protective factors, policy, secondary prevention, case studies, or treatment/medical management of gunshot wounds).
Data abstraction and analysis
Title and abstract review was completed using the web-based program Rayyan (Ouzzani et al., 2016). To establish the protocol for determining eligibility, two content experts reviewed 100 title abstracts independently and blindly. Once the expert reviewers established eligibility criteria and achieved full consensus, trained research assistants applied the criteria for article identification and inclusion. During the title and abstract screening, the independent reviewers erred on inclusion. Data was extracted using a form that captured design, sample and setting, intervention description, outcomes, and limitations.
Results
Article identification and selection
The initial search strategy identified a total of 1780 articles (Fig. 1); removing duplicates (498) resulted in 1282 articles. The title and abstract of the 1282 articles were reviewed for inclusion, with 90 articles meeting eligibility criteria. Experts also identified 12 articles for potential inclusion. The full text of the 102 articles (search identified + expert identified) was reviewed, with 46 articles continuing to meet inclusion criteria included in the scoping review, which focused on: safe storage (23), screening (2), firearm carriage/handling/use (21).
Fig. 1.
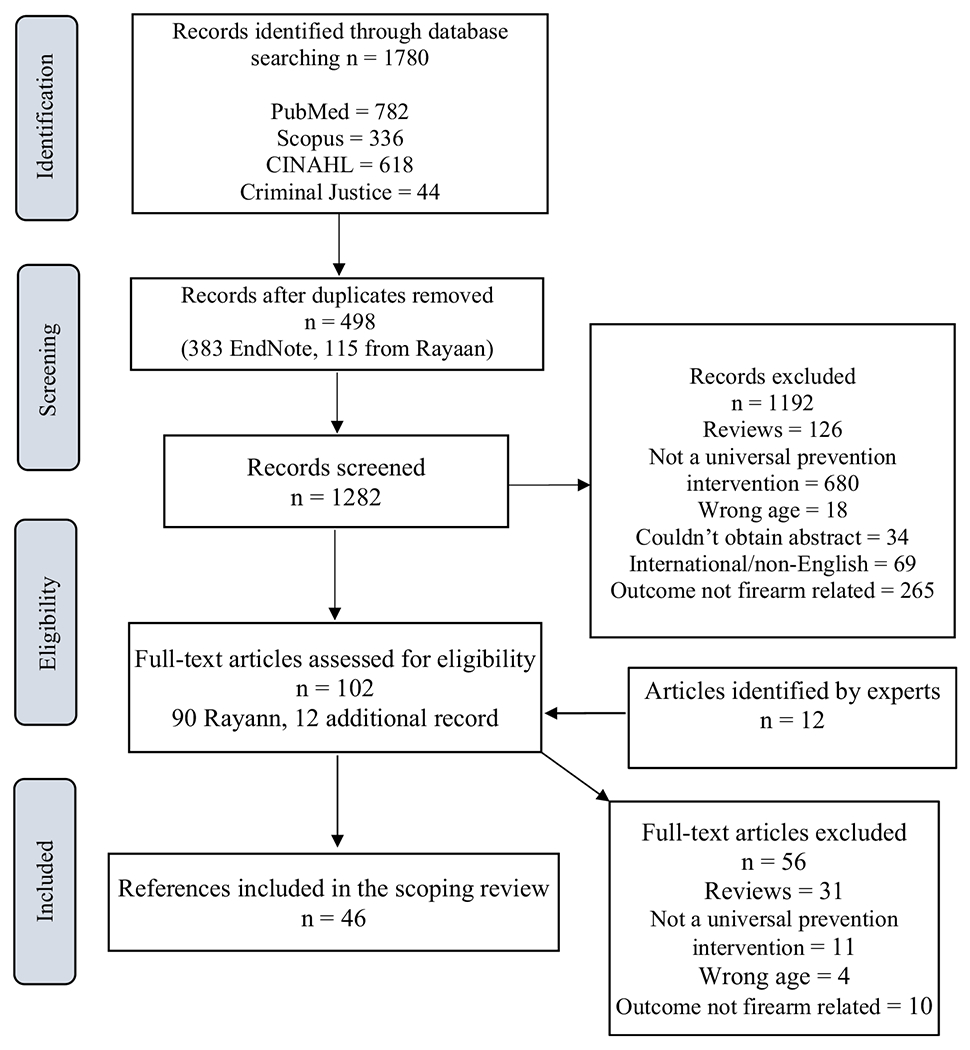
PRISMA diagram: Primary Intervention Article Identification (1985–2018)
Firearm safe storage
In total, 23 articles focused on primary prevention efforts for safe storage (e.g., safes and/or trigger locks), which include individual-level interventions with caregivers in health care settings as well as community-level interventions (see Table 1).
Table 1.
Firearm safe storage and means restrictions
| First author, date | Title | Design | Sample | Intervention | Outcome | Limitations |
|---|---|---|---|---|---|---|
| Training | ||||||
| Dingeldein et al. (2012) | Evaluation of a firearm injury prevention web-based curriculum | Two group RCT | n = 92 pediatric medical student residents in clinics | 3 online training scenarios: 1 related youth firearm injury prevention | Intervention group showed significant improvements in attitudes and self-efficacy as compared to control for physician role in firearm safety at immediate posttest | Opt-in for training may indicate possibility for bias No physician behaviors measured (patient counseling) |
| Health care settings | ||||||
| Kruesi et al. (1999) | Suicide and violence prevention: Parent education in the emergency department | Two group Pretest/Posttest, non-randomized | Parents of n = 103 youth (6–19 years mean age 13.7) in emergency department for mental health | Means restriction staff training: firearms, medications, alcohol | Among 15 parents with firearms at ED visit, those trained were significantly more likely to restrict means than those non-trained at 2 month follow-up | Small Sample size Non-randomized design |
| Oatis et al. (1999) | Pediatric practice based evaluation of the Steps to Prevent Firearm Injury program | One group Pretest/Posttest | n = 1617 parents in pediatrician office; youth 0–17 years | Educational program | No statistically significant reductions in firearmn ownership, storing guns outside of a locked container, or keeping a gun loaded over a 9–11 month follow up | Low posttest retention rate (23.6%) Reliance on self-report No control group |
| Grossman et al. (2000) | Firearm safety counseling in primary care pediatrics: A randomized, controlled | Two group RCT | n = 1295 parents at well-child visits (ages 2 months to 18 years) | Single session gun safety counseling | No statistically significant changes in the rate of acquisition of new guns, removal of guns, or proportion of purchasing trigger locks between the treatment and control groups at 3 month follow up | Impossible to blind treatment providers to group assignment Intervention was not effective |
| Stevens et al. (2002) | A pediatric, practice-based, randomized trial of drinking and smoking prevention and bicycle helmet, gun, and seatbelt safety promotion | Two group RCT, 15 clinics; comparative efficacy | n = 2183 parent/5th and 6th grade youth dyads | Physician counseling, booster call and letter: alcohol/tobacco or safety (safe storage) | At 3-year follow-up, no differences by group in alcohol, tobacco, firearm storage, seatbelt; bike helmet use significantly increased | No control group, so potentially underpowered for comparative efficacy Lack of evidence of effectiveness of program |
| Albright and Burge (2003) | Improving firearm storage habits: Impact of brief office counseling by family physicians randomized | Two group Pretest/Posttest Non-randomized |
n = 156 adult gun owners in family practice (41% children in home) | Physician counseling, with or without storage materials | Intervention participants in both groups were 3 times more likely to make safe changes in gun storage compared to participants in the control at 2–3 month follow up | Small sample size Non-random assignment Reliance on self-report |
| Carbone et al. (2005) | Effectiveness of gun-safety counseling and a gun lock giveaway in a Hispanic community | Two groups Pretest/Posttest, Non-randomized | n = 151 gun owning parents in a pediatric clinic (children 0–17 years, mean age 6–7) | Physician counseling, educational brochure, and gun lock | No significant differences between groups on number of guns removed from household significantly greater frequency of locked storage of firearm and improved type of storage than controls at 1 month follow up | Baseline differences between intervention and control in gun storage Non-randomized Reliance on self-report |
| Barkin et al. (2008) | Is office-based counseling about media use, timeouts, and firearm storage effective? | Two group RCT | n = 137 pediatric practices, mostly moms with child (2–11 years) | Physician counseling about media, discipline, firearm storage, free cable | Approximately half of gun owners reported use of locks on all firearms Significant increases in use of cable locks by intervention as compared to control group over 6 month follow up | Reliance on self-report |
| Runyan et al. (2016) | Lethal Means Counseling for Parents of Youth Seeking Emergency Care for Suicidality | One group Pretest/Posttest | n = 114 parents with suicidal child (12–17 years) in psychiatric emergency services | Trained discharge counselors provided 5 min counseling on safe storage of medications and firearms, with free lock boxes | 33 of 33 parents with guns at home indicated all were locked 2–3 weeks post-discharge | Reliance on self-report No control group Lock boxes only offered for medication storage, not gun storage |
| Community settings: trigger locks and safes, etc. | ||||||
| Coyne-Beasley et al. (2001) | Love our kids, lock your guns: a community-based firearm safety counseling and gun lock distribution program | One group Pretest/Posttest | n = 112 adults (63% had children) | Single session counseling, with up to 4 gun locks provided | Significant increase in storage of guns in locked compartment, use of gun locks, and asking friends about ownership and storage over 6 month follow up | Small sample size No control group Reliance on self-report |
| Roberto et al. (2002) | Promoting gun trigger-lock use: Insights and implications from a radio-based health communication intervention | Two group, Pretest/Posttest Non-randomized |
n = 1500 randomly selected from 2 counties (63% had children under 18 years) | Radio public service announcements with toll-free number to obtain free trigger-lock | 17% of gun-owning households exposed to PSA 799 individuals called to get a trigger-lock At 6-week follow-up, 95% reported trying the lock and 87% reported that the lock was on one of their guns Significant increase in gun safety knowledge | No longitudinal comparison of treatment and control groups |
| Horn et al. (2003) | Community based program to improve firearm storage practices in rural Alaska | One group Pretest/Posttest | n = 40 randomly selected households with 2 or more guns in home (average 2.4 children under 16 years) | Distribution of one gun safe and 1 trigger lock and provision of gun storage education | AT 3-months, 86% of the provided safes were found to be locked with guns inside and 78% of participants reported that all guns were now secure in the household Only 30% of the trigger locks were reported to be in use at 3 month follow up. | Small sample size No comparison/control group Reliance on self-report |
| Wafer and Carruth (2003) | Locks for Life: A gun lock distribution community health intervention program | One group Pretest/Posttest | n = 135 adults attending a local festival (majority had children in household) | Provision of a trigger locks (n = 216) and gun safety literature | 216 gun locks distributed Among, 19 participants, 14 reported using trigger locks and 5 with intent to use trigger locks at 3 month follow up |
86% attrition No comparison/control group |
| Sidman et al. (2005) | Evaluation of a community-based handgun safe-storage campaign | Two groups Pretest/Posttest, Non-randomized | n = 302 households with child (< 18 years) and a firearm | TV and radio safe storage campaign, billboards, and coupons for lock | Increases in intervention and control counties in locking handguns between 1996 and 2001 Significant intervention effects found for households with at least 3 handguns relative to controls |
Rate of lock box discount coupon was not confirmed Non-random assignment Reliance on self-report Control counties had other gun safety initiatives |
| Grossman et al. (2012) | Improving firearm storagein Alaska Native villages: A randomized trial of household gun cabinets | Two group RCT | n = 255 households with at least 1 gun (~ 70% reported children in household) | Free metal gun cabinet installed, safety handout | Intervention group had significantly lower percentage of unlocked guns and ammunition in home compared to controls at 12-months follow-up | Gun cabinet used were designed for rifles and shotguns might not be suitable for urban or non-Native communities |
| Wargo et al. (2013) | Community gun safety in Central Pennsylvania | One group Pretest/Posttest | n = 58 adults attending a Head 6 years or younger) | Gun safety education, gun lock instruction, and a free gun lock | Significant reduction in keeping guns in closet or unattended, and more using a gunlock at 12-month follow-up. No effects of loaded guns, storage of ammunition or reapply lock after removal | 26% retention rate Small sample size No control group Reliance on self-report |
| Simonetti et al. (2017) | Evaluation of a community-based safe firearm and ammunition storage intervention | One group Pretest/Posttest | N = 208 adults attending 2 community-based firearm safety events (53.4% reported children under 18 years) | Brief safety messages for means restriction to prevent suicide, free trigger lock or lock box with practice | Significant increase in firearms stored locked and unloaded. Non-significant increase in ammunition locked up. Significant increase in reports of using all 3 firearm safety procedures at 4–6 weeks | 66% retention rate. No control group Reliance on self-report Lock box used only fit 1 handgun and some ammunition, limiting use for multiple guns or rifles/shot guns |
| Community settings: buyback programs | ||||||
| Callahan et al. (1994) | Money for guns: Evaluation of the Seattle Gun Buy-Back Program | One group Pretest/Posttest | Police records and trauma data; self-report surveys (n varied; 11–91 years old; 2.4% under age 21) | Gun buy-back program | 1772 firearms relinquished, most commonly because they were no longer wanted. No statistically significant changes in firearm-related robberies, assaults, homicides, deaths, and admissions to the trauma center 6 months later | Program unable to detect changes in firearm-related outcomes due to variations in rates over time No comparison/control community |
| Celeste Kallenborn et al. (2004) | Cease Fire Tampa Bay: A three-tiered approach to Firearm injury | One group, Post-test | n = 6 counties Firearm curriculum 3rd and 6th graders/community education program parents of students |
Gun buy-back program, firearm safety education for children and adults, give up to 3 gun locks | 6981 firearms relinquished over ~ 3 years | No outcomes reported beyond the collection of guns No comparison/control community |
| McGuire et al. (2011) | Goods for guns-the use of a gun buyback as an injury prevention/community education tool | One group Posttest only, Non-randomized |
n = 534 adults that learned of the buyback program (37% had children 14 years old or younger | Buyback program, counseling and gun locks, gun destroying ceremony | 1861 guns collected over 8 years; 75 gun locks distributed. Two-thirds said safety was the reason for relinquishing gun, citing children in the home. Downward trend in firearm injuries and mortality in buyback county compared to other counties in state | Outcomes of buyback program not assessed Reliance on self-report Study setting of police headquarters may have biased responses |
| Violano et al. (2014) | Gun buyback programs: a venue to eliminate unwanted guns in the community | One group Pretest | n = 301 adults (27% reported having children in the home) |
Gun buyback program | Relinquished firearms were less likely to have been kept locked; safety reported as the motivation for return. Those with additional firearms in the house were less likely to report having trouble storing the gun. Those knowing someone injured by a firearm were more likely to keep guns locked | Program outcomes not evaluated No control/comparison group Reliance on self-report |
| Green et al. (2017) | Are “goods for guns” good for the community? An update of a community gun buyback program | One group Pretest | n = 109 adults (21% had children who could access guns) | Gun buyback program at police departments | 339 firearms relinquished, with safety as the most common reason;61% reported other guns at home; 21% reported that children could access them; 14% reported a household member with mental illness, suicide, or domestic violence | Survey response rate <60% No control/comparison group Reliance on self-report |
| Kasper et al. (2017) | And the survey said… evaluating rationale for participation in gun buybacks as a tool to encourage higher yields | One group Pretest | n = 273 adults (48% had children living or frequenting their home) | Gun buyback program at police departments | 943 firearms relinquished, with half citing safety reasons as motivation for return. Of households with guns remaining, 27% were potentially accessible to children. 42% of participants took gunlocks home | No comparison/control community No behavioral outcome data reported, including firearm outcomes |
Healthcare settings
In pediatric or health care settings, eight studies examined physician-provided educational messages to parents with children or adolescents in the home (See Table 1) around safe firearm storage (in a gun lock box or with trigger locks which prevent a gun from being fired), either alone or with provision of free locking devices. Generally, studies focused on safe storage as a way of: (1) reducing risk for accidental discharge by children or (2) restricting access to lethal means of self-harm for older children at risk for suicide.
Reducing risks for unintentional discharge of firearms
When examining education of families without provision of safe storage devices, three studies (Grossman et al., 2000; Oatis et al., 1999; Stevens et al., 2002) found no change in firearm storage; however, one other study reported that participants were three times more likely to implement safe storage practices (Albright & Burge, 2003). When examining the combination of education and provision of a safe storage device, two randomized controlled trials (RCTs) found positive effects (Barkin et al., 2008; Carbone et al., 2005), particularly among younger children (< 12 years old). In the largest study that has been conducted, Barkin (Barkin et al., 2008) randomized 137 practices to provider-delivered motivational-interviewing based patient education on a range of safety behaviors, including information on safe firearm storage, car seats, and bike helmets, and provided free gun cable locks to families (with children 2–11 years old) that reported having firearms in the home (~ 24%); over a six-month follow-up, this study found a significant increase in safe firearm storage (Odds Ratio: 2.0; 22% difference between groups).
Restricting access to lethal means for self-harm
Two studies examined safe storage counseling (talking with parents/caregivers about limiting youth access to potential methods of suicide, such as firearms and medications) in emergency departments (Kruesi et al., 1999; Runyan et al., 2016). One study showed that parents of children receiving safe storage counseling in the emergency department were 4 times more likely to limit access to firearms and medications compared to those parents who did not receive safe storage counseling (Kruesi et al., 1999). In a second study, psychiatric emergency clinicians (i.e., psychiatrists, psychologists, and social workers) participated in online training in safe storage counseling, after which 89% of youth presenting for suicidal ideation or attempt received safe storage counseling with provision of a free lock box, and at follow-up all caregivers reported locking firearms (Runyan et al., 2016). More research is needed in health care settings to optimize delivery of combined counseling, and provision of safety devices, and to measure impact on firearm injury-related outcomes. Additionally, more research is needed on measurement of safe storage as all but one of the studies (Grossman et al., 2000) above used self-report to measure safe storage.
Training of healthcare providers
Finally, one study, separate from those in the two sections above, examined training resident physicians to deliver educational messages to patients during office visits, which is key to delivering safe storage messages to patients in healthcare settings (Dingeldein et al., 2012). The study found increases in reported self-efficacy in discussing firearm safety with patients after a web-based curriculum; however, effects on actual delivery of counseling, or on patient outcomes, were not evaluated (Dingeldein et al., 2012). Additional research is needed to determine whether and what aspects of these trainings may be effective in increasing delivery of counseling to patients and whether the counseling delivered has an impact on patient behaviors and outcomes such as safe storage of firearms or reductions in firearm injuries.
Community settings
Community-based interventions for safe firearm storage have generally included firearm lock box give-away programs, firearm buy-back programs, and/or community education programs. Eight studies evaluated locking device giveaways (Coyne-Beasley et al., 2001; Grossman et al., 2012; Horn et al., 2003; Roberto et al., 2002; Sidman et al., 2005; Simonetti et al., 2018; Wafer & Carruth, 2003; Wargo et al., 2013), with findings generally indicating that distribution of safe storage devices led to an increase in self-reports of safe firearm storage, regardless of where they were dispersed; however, none of the studies evaluated the effects on youth firearm-related injury.
Safe storage education programs
Two community education initiatives report mixed results. Assessment of a radio public service announcement (PSA) about safe storage, with toll-free number to obtain trigger locks, found that ~ 20% of the population heard the PSA but only 3% of gun-owning households in the community called to obtain trigger locks. However, 87% of those who requested gun locks used them (Roberto et al., 2002). A multifaceted community safe firearm storage educational campaign (with lock box coupons) found a significant difference between individuals in intervention and control counties (i.e., individuals in intervention counties were more likely to lock guns) in a subset of firearm owners (with 3 or more firearms; intervention: 233% increase; control: 39% decrease) (Sidman et al., 2005).
Firearm buyback programs
Finally, six studies examined firearm buyback programs (Callahan et al., 1994; Green et al., 2017; Celeste Kallenborn et al., 2004; Kasper et al., 2017; McGuire et al., 2011; Violano et al., 2014), consistently finding that reasons for participation were for safety, particularly in the context of having children at home, with one study finding younger participants more often cited needing money as the reason (Callahan et al., 1994). Although most studies do not assess firearm-related outcomes from these buyback programs, one study showed no effects on rates of assault injuries or death (Callahan et al., 1994) whereas another reported a non-significant decreasing trend on firearm injuries in the intervention versus control communities (McGuire et al., 2011).
Firearm handling, carriage, and use
In total, 2 studies focused on screening tools and 21 articles described primary prevention interventions for firearm handling, carriage, or use (see Table 2) conducted in healthcare, school, and community settings, with focus typically on children or adolescents.
Table 2.
Prevention of firearm handling, carriage, and use
| First author, date | Title | Design | Sample | Intervention | Outcomes | Limitations |
|---|---|---|---|---|---|---|
| Screening | ||||||
| Hayes and Sege (2003) | FiGHTS: a preliminary screening tool for adolescent firearms-carrying | One group, Pretest | n = 15000 high school students | None: Screening measure development | Analyses of YRBS data from 1999 to identify items (FiGHTS) related to firearm carriage, with five items identified: Fighting, Gender, Hurt while fighting, Threatened, and Smoker | Longitudinal predictive validity unknown |
| Goldstick et al. (2017) | Development of the SaFETy Score: A clinical screening tool for predicting future firearm violence | Two group Pretest/posttest, non-randomized | n = 599 drug using youth (14–24 years) in emergency department | None: Screening measure development | 4 baseline questions (safety score) predicted firearm violence over 2 years: Serious fighting, community environment, friend weapon carriage (including gun), and firearm threats. 24-month follow up | Need for validation in future studies, including those without drug use entry criteria Reliance on self-report |
| Child-focused programs (ages 0–9 years) | ||||||
| Hardy et al. (1996) | A firearm safety program for children: They just can’t say no | Two group RCT | n = 48 daycare children (4–6 years) | Individual education not to play with guns | Children who played with guns were more likely to interact with guns at home and show more aggression in their play. The intervention and control did not differ in gun play at 2-week follow up | Intervention was not effective. Small sample size |
| Hardy (2002) | Teaching firearm safety to children: Failure of a program | Two group RCT | n = 70 daycare children (4–7 years) | 4 Lessons: Straight Talk bout Risks | 37 children (53%) played with the guns in the structured setting. No difference between groups in gun play at 1 week posttest | Lack of evidence of effectiveness of program. Possible contamination between groups |
| Liller et al. (2003) | Evaluation of the “Respect not Risk” firearm safety lesson for 3rd-graders | One group Pretest/Posttest | n = 433 3rd graders | 1 lesson on firearm safety with letter for families about free gun locks | Significant increases in knowledge at posttest, and sharing with family at 1-week posttest | No control group No behavioral outcome data reported, including firearm outcomes |
| Himle et al. (2004a) | An evaluation of two procedures for training skills to prevent gun play in children | Three group RCT Posttest only |
n = 31 preschool children (4–5 years) | Eddie Eagle Gun Safe Program and behavioral skills training (BST) | The Eddie Eagle group and the BST group scored significantly better on self-report than controls; only the BST group scored better on role-play assessments and no differences in groups based on in situ 1-week assessment | Small sample size Less than half of consent forms given out were returned (selection bias |
| Himle, Miltenberger, et al. (2004b) | Teaching safety skills to children to prevent gun play | One group Pretest/Posttest | n = 8 preschool children (4–5 years) | BST | Education alone was not effective, as in situ training was necessary for all children to require skills, which were maintained in all but 1 child up to 8 weeks | Small sample size No control group |
| Miltenberger et al. (2005) | Teaching safety skills to children to prevent gun play: An evaluation of in situ training | One group post-test | N = 10 preschool children (4–5 years) | BST | All 10 children executed the safety skills following BST with in situ training in school and home assessments at 3-month follow-up | Study did not directly compare BST with and without in situ training |
| Jostad et al. (2008) | Peer tutoring to prevent firearm play: Acquisition, generalization | One group Pretest/Posttest | n = 6 preschool children (4–5 years) | BST delivered by 6–7 year old peers | Multiple BST sessions were needed for skill acquisition for half the children, the remaining required in situ training, evidence for maintenance over 1-year was mixed | Small sample size No control group |
| Gatheridge et al. (2004) | Comparison of two programs to teach firearm injury prevention skills to 6 and 7-year-old children | Three group RCT | n = 45 children in after school programs (6–7 years) | 4, 15-min sessions of: Eddie eagle, or BST | Although both interventions increased knowledge, only the BST intervention scored better than controls based on role play and in situ assessments (1 week later) | No long-term follow-ups or assessment outside of the research environment (e.g., home). Unclear if data collectors were blinded to condition assignment |
| Howard (2005) | Evaluation of age-appropriate firearm safety interventions | Four group RCT | n = 57 K and 1st graders, from 8 schools | 4 groups: discussion alone, discussion and psychomotor, discussion, psychomotor and role plays, control | Knowledge about firearm safety increased in all intervention groups, but not in the controls. The discussion/psychomotor group had the greatest increase at 1-month follow-up | Small sample size No behavioral outcome data reported, including firearm outcomes |
| Kelso et al. (2007) | Teaching skills to 2nd and 3rd grade children to prevent gun play | Three group RCT, Posttest only | n = 30 children 8–9 years | 45 min Eddie eagle or BST | Both interventions were efficacious based on self-report; however, there were no differences between either intervention and control in role play and in situ assessments on gun play safety at immediate posttest | Small sample size Lack of evidence of effectiveness of program on gun play behaviors |
| Gross et al. (2007) | Preliminary evaluation of a parent training program to prevent gun play | One group Pretest/Posttest | n = 4, children 4–7 years | Parent BST | BST was effective for 3 of 4 participants and was implemented with fidelity by 3 of the 4 parents during training | Small sample size No control group |
| Kenny and Wurtele (2016) | Teaching preschoolers safety rules: A pilot study of injury prevention | Two group Pretest/Posttest non-randomized | n = 346 preschool children (3–5 years), primarily Latino | 10 one-hour sessions BST | Intervention group showed significant improvement self-report than control at 2–3 month (average 75 days) follow-up | Differential sample size between groups (e.g., 45 in control). Non-randomized design. No behavioral outcomes assessed |
| Adolescent-focused programs (ages 10–17 years) | ||||||
| Davidson et al. (1994) | The impact of the Safe Kids/Healthy Neighborhoods Injury Prevention Program in Harlem, 1988 through 1991 | Two group Pretest/Posttest | Youth in Harlem community (under 17 years) | Multi-component: park clean-up, leisure activities, injury prevention including guns | After 3 years, the intervention community showed decreases in assaults, but no differences in gun injuries, relative to the comparison. Significant findings were for motor vehicle injuries; falls were unchanged | Intervention community had greater baseline injury rates than the comparison. Non-randomized design. The many interventions preclude determination of efficacy of particular components. Unclear intervention focus on firearms |
| Thomas (et al. 1998) | Breaking the cycle of violence among youth living in metropolitan Atlanta: A case history of kids alive and loved | One group Pretest/Posttest | n = 58 African-Americansm (10–20 years; mean 15.8) | Support group for youth exposed to violence (lost a loved one from gun violence) | Increases in anecdotal reports of youth managing anger, conflict resolution, and increasing leadership; no systematic follow-up | No comparison/control group No behavioral outcome data reported, including firearm outcomes |
| Tucker et al. (1999) | Violence prevention: Reaching adolescents with the message | One group Pretest/Posttest | n = 99 5th–8th graders | Videos, anger management, and paralyzed gunshot victim testimonial | Program acceptability ratings reported at 1-month follow up | No comparison/control group No behavioral outcome data reported, including firearm outcomes |
| Durant et al. (2001) | Evaluation of a peaceful conflict resolution and violence prevention curriculum for sixth-grade students | Two group Pretest/Posttest non-randomized 4 schools | n = 704 middle school students (11–14 years) | 13 session violence prevention curriculum | Relative to control, at posttest intervention groups showed significant decrease in carrying a concealed gun, intention to use violence, and use of violence at 2 week posttest | Baseline violence differences (more in intervention schools) could have confounded findings. Data not analyzed nested by school Longer term outcomes unknown |
| Emde (2002) | Cops and Docs: A gun violence injury prevention program | One group Post-test | n = 5000 middle school students (13 years) | Cops and Docs program: 50-minute slides and discussion about gun violence | The program has been disseminated to school districts in WA and in 14 states; no follow-up | No control group No outcome data reported despite post-test Lack of evidence of effectiveness of program |
| Chang et al. (2005) | A multidisciplinary youth violence-prevention initiative: Impact on attitudes | One group Pretest/Posttest | n = 97 adolescents from community (mean 12.6 years) | Hospital tour showing video/slides of gun violence | Statistically significant reduction in beliefs supporting aggression and trend toward reduced likelihood of violence a month later (mean 25.8 days). | 49% completed posttest No control group No behavioral outcome data reported, including firearm outcomes |
| Regan (2009) | Implementation and evaluation of a youth violence prevention program for adolescents | One group Pretest/Posttest | n = 20 9th–10th graders | 4 sessions on gun and gang violence, field trip to trauma center | Significant improvement in perceived knowledge about the history of gang violence and its impact on American culture and methods to decrease gun violence immediately after program | Small sample size No control group No behavioral outcome data reported, including firearm outcomes |
| Kunkel et al. (2010) | A hospital-based violence prevention tour: A collaborative approach to empower youth | One group Pretest/Posttest | n = 185 adolescents from community (10–17 years) | Tour of hospital, discussion about gun violence, and PowerPoint slides | 84% reported an increase in awareness of violent injuries, which was significantly higher among girls than boys, immediately after program | Small sample size No control group No behavioral outcome data reported, including firearm outcomes |
| Goldberg et al. (2010) | An analysis of inner-city students’ attitudes towards violence before and after participation in the “Cradle to Grave” (C2G) program | One group Pretest/Posttest | n = 88 8th and 9th graders | 2-h program in trauma center with video about youth death from gunshot wound | Significant reduction in violent beliefs among those from a public school but not those from a charter school at 4-week follow up | No control group No behavioral outcome data reported, including firearm outcomes |
Screening tools
Two studies specifically examined firearm-related screening tools for identifying those at greatest risk for firearm-related injuries. Goldstick (Goldstick et al., 2017) recruited drug-using youth presenting to the emergency department and found that the 4-item SaFETy score predicted firearm violence over 2 years; however, this study oversampled those presenting for a fighting related injury (58%), all participants reported drug use (predominantly marijuana), and the sample included emerging adults (ages 14–24). Thus, replication is required to determine generalizability to more representative samples of youth. The five-item FIGHTS, was developed to screen youth for firearm carriage using cross-sectional YRBS data (Hayes & Sege, 2003), with 30% of adolescents screening positive (representing 82% of firearm carriers); however, longitudinal data is needed to verify the predictive validity of this tool.
Child-focused programs (ages 0–9 years)
Twelve studies have evaluated teacher-led programs to prevent children from handling firearms, with mixed overall findings. For example, two studies, using education only, found no effects (Hardy, 2002; Hardy et al., 1996), but one education program that included a letter to parents about how to obtain free gun locks, found significant improvements in knowledge among 3rd graders, who also reported sharing information with their families (Liller et al., 2003). Several studies suggest that behavioral skills rehearsal (e.g., Behavioral Skills Training) is necessary for skill acquisition, and is more effective than interactive education only (e.g., Eddie Eagle), on outcomes assessed in hypothetical situations (Gatheridge et al., 2004; Himle et al., 2004a; Howard, 2005; Jostad & Miltenberger, 2004; Miltenberger et al., 2005). Also, feasibility studies suggested that parents could be trained to teach their children firearm safety skills (Gross et al., 2007) and older peers (e.g., 6–7 year olds) can teach 4–5 year olds (Gatheridge et al., 2004; Himle et al., 2004b; Howard, 2005; Jostad & Miltenberger, 2004). However, this literature is limited by small samples sizes and either lack of assessment of behavioral outcomes (Kenny & Wurtele, 2016) or finding null effects for in situ “real life” situations (Himle et al., 2004a; Kelso et al., 2007). Thus, despite evidence that age appropriate firearm safety programs for children can change knowledge of firearm safety, effects on firearm handling (and injury) are unclear.
Adolescent-focused programs (ages 10–17 years)
School settings
Among adolescents, three school-based programs have specifically focused on preventing weapon carriage/use, primarily among middle school students. For example, one study conducted a RCT to evaluate a 13-week school based violence prevention curriculum in middle schools (2 control, 2 intervention), finding that at 2-weeks post-intervention, students in the intervention arm carried concealed weapons less frequently than at pretest (DuRant et al., 2001). Other school-based programs show significant effects on knowledge (Regan, 2009) and/or do not report outcomes (Emde, 2002). Thus, additional research on school-based curricula is necessary to examine the impact on prevention of firearm carriage.
Healthcare settings
Other adolescent-focused programs emphasizing medical consequences of gunshot wounds (e.g., videos, testimonials, with or without trauma center tour) show positive effects only on knowledge and beliefs regarding firearm consequences and safety (Chang et al., 2005; Goldberg et al., 2010; Kunkel et al., 2010); however, these studies have not had control groups nor measured behavioral outcomes (Tucker et al., 1999). Another program (Kids Alive and Loved; (Thomas et al., 1998) qualitatively described positive outcomes on anger management skills and assaultive behavior among youth who recently lost a loved one to violence but did not include a control group.
Community settings
Finally, a community-level intervention that included multiple components, such as park cleaning/greening, leisure activities, injury prevention (including firearms), did not show any specific effects on firearm injuries (Davidson et al., 1994).
Discussion
It is imperative to develop primary prevention efforts to prevent firearm-related injuries and deaths among children and adolescents given the individual, social, and economic costs (Fowler et al., 2017; Howell & Abraham, 2013) by increasing safe storage among caregivers and decreasing firearm handling/carriage among youth. To inform such prevention efforts, this scoping review assessed the state of the science regarding primary prevention approaches. We reviewed the literature on interventions focused on the safe storage of firearms and firearm handling, carriage, and use, identifying few evidenced-based programs in home, school, healthcare, or community settings. Overall, the literature is plagued with methodological weaknesses, with few RCTs and infrequent evaluation of longer-term behavioral outcomes (e.g., safe storage, firearm carriage and play), as well as the lack of assessment of the impact on firearm injury and mortality. These weaknesses likely relate to the lack of funding for rigorous trials. Nonetheless, some tentative conclusions and future directions can be provided.
Firearm safe storage
Interventions in health care settings have been most rigorously evaluated, providing evidence that clinician screening and education around firearm safety, particularly when paired with the distribution of free gun locks, increases self-reports of safe firearm storage in homes with children (Rowhani-Rahbar et al., 2015). Given that routine screening and education across health care settings is lacking (Roszko et al., 2016), improving adoption of screening and firearm safety education is needed. As safe storage education in health care settings have often focused on children, extension to adolescents is urgently needed given rates of suicide and homicide. In addition, there is little data regarding the feasibility and acceptability of screening and counseling approaches in health care settings from the perspective of patients. Finally, pediatric health care visits are constrained by time allotted to the visit, limited opportunities to reinforce messaging over time, and are typically attended by mothers (Barkin et al., 2008), which means that counseling in this setting may fail to reach other adults or gun owners in the household.
Thus, from a social ecological perspective (Centers for Disease Control and Prevention, 2015; Urie, 1979), prevention programs in health care settings are necessary but are not sufficient to prevent all youth firearm-related injuries, with community-level approaches needed to complement such efforts. As evidence supports that providing free gun locking devices leads to an increase in self-reports of safer storage, there is rationale to expand such practices across settings. However, measurement of safe storage was almost solely through self-report which may be plagued by social desirability issues, indicating a need for further research on methods of assessing safe storage. The one study that included field observations of safe storage did not indicate whether this observation was a cursory visual inspection, or if it included query and assessment of firearms that may not have been stored safely but were out of the visual field of the research team (Grossman et al., 2000). Verification of self-report of firearm storage is needed using approaches that are acceptable to gun owners, as some findings suggest that home visits may not be acceptable (Sangvai et al., 2007) as well as very expensive. Finally, although firearm buyback programs increase the number of firearms relinquished, their efficacy on reducing youth firearm injuries is not yet determined and requires more rigorous study.
Firearm carriage, handling, and use
Focusing on children, school-based interventions that include behavioral skills training to prevent firearm handling increase knowledge and hypothetical skills, but lack data on real world situations and effects on firearm injuries. Despite this unknown efficacy, development of scalable approaches to reduce handling of firearms among preschool and elementary-aged youth seems warranted. Similarly, among adolescents, school-based programs have positive outcomes on knowledge and attitudes, but effects on firearm carriage, handling and use behaviors are largely unknown, with a notable exception showing positive effects on weapon carriage at post-test (DuRant et al., 2001). In parallel, interventions for adolescents that use scare tactics (e.g., videos, testimonials, and/or tours illustrating gunshot wounds and emergency care settings) lack evidence for changing firearm carriage and firearm injury. Note that general violence prevention studies were not included in this review, as they did not measure firearm specific outcomes. For example, a single session intervention (Project Sync) for adolescents presenting to the emergency department for any reason reduced aggression, including firearm aggression (Carter et al., 2016), and a collaborative care intervention for hospitalized adolescents reduced weapon carriage, including firearms (Zatzick et al., 2014). A potential next step for research in this area is to test the potential impact of these promising prevention programs, such as SaferTeens, Project Sync, and others in the CDC technical package on violence, specifically on firearm outcomes in fully powered studies (Blueprints, 2018; Caldwell et al., 2010; Carter et al., 2016; Center for Disease Control and Prevention, 2018; Cunningham et al., 2012; DuRant et al., 2001; Reischl et al., 2011; Walton et al., 2010; Zatzick et al., 2014; Zimmerman et al., 2011).
Further, although multi-level community programs provide an opportunity to increase impact on prevention of youth firearm injuries, only one study was identified in this review that focused specifically on children or adolescents (Davidson et al., 1994). Among broader community samples, data suggest that vacant lot clean up and greening projects have an impact on firearm assaults (Branas et al., 2011; Garvin et al., 2013). Specifically, in a recent cluster randomized trial that fell outside of our search period, removal of blighted vacant lots reduced shootings, with no evidence that the shootings were displaced to adjacent areas (Moyer et al., 2019). Moreover, a recent study demonstrated that implementation of primary violence prevention efforts across the social ecology in a community (e.g., individual intervention, mentoring, vacant lot clean up) reduced assault injuries; however, firearm-related outcomes (e.g., carriage, use, injuries) were not assessed (Heinze et al., 2016). Finally, several community-level interventions focused primarily on gang members, and/or older samples (e.g., adults over 18 years; Cease Fire: (Skogan et al., 2009); Safe Streets: (Duncan et al., 2014; Milam et al., 2016; Whitehill et al., 2013), show promise for reducing firearm injury. Altogether, these studies underscore the potential impact of multi-sector community wide interventions.
Limitations
Several limitations must be noted. First, this scoping review may not have been fully comprehensive (e.g., did not include targeted searching of specific journals or hand searches in journals without an online presence). Second, studies published between the initial search and publication of this article will not be included. Third, we did not include non-English articles or successful prevention intervention efforts outside of the United States. Given the unique context of U.S. firearm ownership, we felt it was appropriate to focus on the state of the science in the U.S. Next, our review required firearms to be in the title or abstract, which could have excluded articles that describe prevention programs that did not list firearms specifically; however, such studies are not likely to measure firearm specific behaviors if not stated. This review did not include policy-level changes in relation to youth firearm outcomes as those are described elsewhere, nor did it focus on interventions for high-risk samples (e.g., youth with a prior firearm and/or assault injury) as these likely require a dedicated focus of their own. Despite these limitations, this scoping review provides useful insights into future directions.
Future directions for research and practice
Overall, research on firearm safety for children and adolescents require a broader focus and more rigorous methods, including: (1) use of RCT designs to control for societal level events (e.g., legislative changes, mass shootings); (2) measurement of multiple firearm behavioral outcomes that go beyond self-report, including storage, carriage and use, as well as firearm injuries and deaths; (3) assessment of longitudinal outcomes beyond post-test; (4) inclusion of diverse samples by age (children and adolescents), gender (caregiver and youth), race/ethnicity, and socio-economic resources; (5) enhanced attention to fidelity of intervention delivery; (6) focus on multiple risks for adverse firearm outcomes across youth violence, suicide, IPV, and unintentional injuries; (7) integration of interventions across the social ecology; (8) attention to implementation of evidenced-based approaches (e.g., see Wolk et al., 2017), including measurement of cost effectiveness. This is particularly true for research and interventions focusing on safe storage, and firearm handling, carriage, and use among children and adolescents.
Of critical importance, we recommend using a participatory action framework (Baum et al., 2006) to partner with firearm owners to further research and practice of prevention of youth firearm-related injuries. Two recent studies which fell outside of our article search time frame indicated that parents, healthcare providers, staff and clinic leaders found firearm interventions acceptable and feasible (Beidas et al., 2018; Wolk et al., 2018). Wolk and colleagues (2018) also found that firearm owners and non-owners had overall similar responses with regard to implementing an evidence-based approach to firearm safety promotion (Wolk et al., 2018). However, many of the interventions reviewed failed to mention whether they received input from firearm-owning caregivers, potentially creating a disconnect between program focus and what is acceptable, including reasons for firearm ownership (e.g., safety/protection, hunting, recreation) and barriers to safe storage. In a parallel manner, involvement of firearm owners in refining interventions to prevent carriage and use of firearms by adolescents is considered essential.
There is mounting evidence that in healthcare settings, clinician-provided education in tandem with gun locks is a promising intervention approach for child and adolescent firearm safety. Moreover, Beidas et al. (2018) and colleagues (in press) found that primary care physicians who were provided training, provided education about firearm safety commonly, although not routinely. This parallels promising preliminary evidence that community-based gun lock distribution and education may also be an effective approach to decreasing firearm injuries among children and adolescents (Simonetti et al., 2018). Although gun buy-back programs have reported more mixed results, additional research into these strategies are also needed to fully evaluate efficacy (Callahan et al., 1994; McGuire et al., 2011). Finally, a two-pronged approach could be used, based on whether firearms are present in the home. For families without firearms in the home, safe storage counseling would focus on prevention of access in other homes where their children may play; for families with firearms in the home, safe storage counseling and provision of free locking devices would be tailored based on the adults in the home, the number/type of firearms present, and whether the youth was at risk for suicide.
Notably, the majority of behavioral interventions across community settings are delivered using an individual, in-person delivery modality. Alternatively, to promote fidelity and scalability, future studies should consider harnessing digital modalities to support screening, and intervention delivery (e.g., videos, text messaging, websites), which could be integrated with in-person delivery. Moreover, there were no studies utilizing mobile health approaches (e.g., social media, smartphone apps, wearables) for firearm safety for youth.
Finally, the lack of research testing the efficacy of firearm safety technology (e.g., trigger locks, personalized smart sensors) on improving safety and accessibility of firearms by adults, while preventing negative firearm outcomes among youth, is a serious gap in the field. Such studies could be informed by research examining ergonomics of firearm safety mechanisms (Cornell & Khasawneh, 2008) as well as the preferences of gun owners. It is unknown what segments of gun owners may prefer higher technology gun locks, or smart firearm technology. Academic researchers, gun owners and industry manufacturers could partner in fruitful collaborations to further advancements in firearm design and technology (e.g., biosensors) that could potentially enhance firearm safety for children and adolescents while respecting preferences of gun owners. Research here may learn from similar changes in acceptability of car and safety seat technology over the past two decades.
Conclusions
There is a clear need for evidenced-based primary prevention approaches to reduce firearm injuries among children and adolescents, which to date are limited due to methodological weaknesses and an overall paucity of research. Best practices for prevention are needed across settings, including homes, schools, health care, and broader communities with attention to scalability, potentially using digital health approaches. To accelerate the process of filling this knowledge gap, we encourage researchers to incorporate firearm-related measures and outcomes into longitudinal studies of youth and to consider adapting promising, evidenced-based interventions to address firearm outcomes. These adapted interventions could be tested using hybrid efficacy-implementation studies (Curran et al., 2012). Partnering with community stakeholders and firearm owning parents, using a participatory action approach (Baum et al., 2006), will be critical during adaptation to maximize acceptability, efficacy and impact on youth. Finally, firearm safety technology both in safe storage devise and in firearms themselves is an emerging area that requires study to determine acceptability, feasibility and benefits and risks for families of children and adolescents.
While we recognize and discuss the need for further research, we believe the overall currently available evidence indicates that safe-storage of firearms will reduce the risk of firearm injury to children and adolescents. Physicians in the U.S. are allowed to and should ask families about firearms in the homes where youth live and regularly visit. Counseling about safe storage and provision of locking devices can potentially reduce firearm injuries and death among youth.
Acknowledgements
We would like to thank Gurpreet Kaur Rana, Informationist at the Taubman Health Sciences Library, University of Michigan, for creating the search strategies. We would also like to thank Jhuree Hong and Jaemin Park, and Stephanie Kostolansky for assisting with title abstract screening, organizing and summarizing articles for review.
Funding
This review was funded by NIH/NICHD 1R24HD087149-01A1. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies. Supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health K23 AA022641.
Appendix: PubMed scoping review search strategy
PubMed
Date Searched:
March 29, 2018
Final number of results:
782
(gun[tiab] OR guns[tiab] OR handgun[tiab] OR handguns[tiab] OR firearm[tiab] OR firearms[tiab] OR “fire-arms”[MeSH Terms] OR gunshot[tiab] OR gunshots[tiab] OR shooting[tiab] OR shootings[tiab]))) AND ((“Wounds and Injuries”[Mesh] OR “wounds, gunshot”[MeSH Terms] OR injury[tiab] OR injuries[tiab] OR mortality[-tiab] OR non-fatal[tiab] OR nonfatal[tiab] OR fatal[tiab] OR intentional[tiab] OR unintentional[tiab] OR accidental[tiab] OR Homicide[Mesh] OR killing*[tiab] OR murder*[tiab]))) AND (Prevent*[tiab] OR “prevention and control”[Subheading] OR “Primary Prevention”[MeSH Terms] OR “Preventive Health Services”[Mesh]) AND (Behavior[MeSH Terms] OR behavior[tiab] OR “violence prevention”[tiab] OR violence[MeSH] OR crime[MeSH Terms] OR “criminal justice”[tiab] OR Jurisprudence[MeSH] OR “legislation and jurisprudence”[Sub-heading] OR courts[tiab] OR judicial[tiab] OR counseling[MeSH Terms] OR “Health Promotion”[MeSH Terms] OR “Health Education”[MeSH Terms] OR “Mental Health Services”[MeSH Terms] OR “Community Health Services”[MeSH Terms] OR “community health”[tiab] OR “mental health”[tiab] OR “safe storage”[tiab] OR storage[tiab] OR “gun safety”[tiab] OR safety[MeSH] OR “Residence Characteristics”[MeSH Terms] OR Schools[MeSH Terms] OR “school-based”[-tiab] OR school*[tiab] OR “community-based”[tiab] OR communit* OR “Protective Devices”[MeSH Terms] OR bulletproof OR Technology[MeSH Terms] OR technolog*[MeSH Terms] OR “Protective Factors”[MeSH Terms]) AND (adolescent[MeSH Terms] OR youth[MeSH Terms] OR child[MeSH Terms] OR teenager[Title/Abstract] OR teen[Title/Abstract] OR adolescen*[Title/Abstract] OR child[Title/Abstract] OR youth[title/abstract] OR children[Title/Abstract] OR minor[Title/Abstract] OR minors[title/abstract] OR delinquent[Title/Abstract] OR delinquency[Title/Abstract] OR pediatric*[Title/Abstract] OR parent*[tiab]) AND (“1985/01/01”[PDat]: “2018/12/31”[PDat]).
Filters:
Publication date from 1985/01/01 to 2018/03/28.
Footnotes
Conflict of interest Quyen M. Ngo, Eric Sigel, Allante Moon, Sara F. Stein, Lynn S. Massey, Frederick Rivara, Cheryl King, Mark Ilgen, Rebecca Cunningham, and Maureen A. Walton declares that they have no conflict of interest.
Human and animal rights and Informed consent All procedures followed were in accordance with ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
References
- Albright TL, & Burge SK (2003). Improving firearm storage habits: Impact of brief office counseling by family physicians. The Journal of the American Board of Family Practice, 16, 40–46. [DOI] [PubMed] [Google Scholar]
- American Academy of Pediatrics. (2016). Survey: Gun violence prevention a big issue for most pediatricians. Retrieved from http://www.aappublications.org/news/2016/08/10/GunViolence081016. Accessed 9 Nov 2018.
- Arksey H, & O’Malley L (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8, 19–32. [Google Scholar]
- Barkin SL, Finch SA, Ip EH, Scheindlin B, Craig JA, Steffes J, et al. (2008). Is office-based counseling about media use, timeouts, and firearm storage effective? Results from a cluster-randomized, controlled trial. Pediatrics, 122, e15–e25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baum F, MacDougall C, & Smith D (2006). Participatory action research. Journal of Epidemiology and Community Health, 60, 854–857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beidas RS, Jager-Hyman S, Becker-Haimes EM, Wolk CB, Ahmedani BK, Zeber JE, et al. (2018). Acceptability and use of evidence-based practices for firearm storage in pediatric primary care. Academic Pediatrics. 10.1016/j.acap.2018.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blueprints for Healthy Youth Development. (2018). Blueprints for Healthy Youth Development. Retrieved from https://www.blueprintsprograms.org/. Accessed 9 Nov 2018.
- Branas CC, Cheney RA, MacDonald JM, Tam VW, Jackson TD, & Ten Have TR (2011). A difference-in-differences analysis of health, safety, and greening vacant urban space. American Journal of Epidemiology, 174, 1296–1306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caldwell CH, Rafferty J, Reischl TM, De Loney EH, & Brooks CL (2010). Enhancing parenting skills among nonresident African American fathers as a strategy for preventing youth risky behaviors. American Journal of Community Psychology, 45, 17–35. 10.1007/s10464-009-9290-4 [DOI] [PubMed] [Google Scholar]
- Callahan CM, Rivara FP, & Koepsell TD (1994). Money for guns: Evaluation of the Seattle gun buy-back program. Public Health Reports, 109, 472. [PMC free article] [PubMed] [Google Scholar]
- Carbone PS, Clemens CJ, & Ball TM (2005). Effectiveness of gun-safety counseling and a gun lock giveaway in a hispanic community. Archives of Pediatrics and Adolescent Medicine, 159, 1049–1054. 10.1001/archpedi.159.11.1049 [DOI] [PubMed] [Google Scholar]
- Carter PM, Walton MA, Zimmerman MA, Chermack ST, Roche JS, & Cunningham RM (2016). Efficacy of a universal brief intervention for violence among urban emergency department youth. Academic Emergency Medicine, 23, 1061–1070. 10.1111/acem.13021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2015). The social-ecological model: A framework for prevention. Atlanta, GA: CDC. Retrieved from https://www.cdc.gov/violenceprevention/overview/social-ecologicalmodel.html. Accessed 2 Nov 2018. [Google Scholar]
- Center for Disease Control and Prevention. (2018). Youth violence. Retrieved from https://www.cdc.gov/violenceprevention/youthviolence/index.html. Accessed 2 Nov 2018.
- Chang DC, Cornwell EE III, Sutton ER, Yonas MA, & Allen F (2005). A multidisciplinary youth violence-prevention initiative: Impact on attitudes. Journal of the American College of Surgeons, 201, 721–723. [DOI] [PubMed] [Google Scholar]
- Cornell MA, & Khasawneh MT (2008). An ergonomic comparison of firearm safety mechanisms. Ergonomics, 51, 1394–1406. [DOI] [PubMed] [Google Scholar]
- Coyne-Beasley T, Schoenbach VJ, & Johnson RM (2001). Love our kids, lock your guns: A community-based firearm safety counseling and gun lock distribution program. Archives of Pediatrics and Adolescent Medicine, 155, 659–664. [DOI] [PubMed] [Google Scholar]
- Crossen EJ, Lewis B, & Hoffman BD (2015). Preventing gun injuries in children. Pediatrics in Review, 36(2), 43–50. [DOI] [PubMed] [Google Scholar]
- Cunningham RM, Chermack ST, Zimmerman MA, Shope JT, Bingham CR, Blow FC, et al. (2012). Brief motivational interviewing intervention for peer violence and alcohol use in teens: One-year follow-up. Pediatrics, 129, 1083–1090. 10.1542/peds.2011-3419 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cunningham RM, Walton MA, & Carter PM (2018). The major causes of death in children and adolescents in the United States. New England Journal of Medicine, 379, 2468–2475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curran GM, Bauer M, Mittman B, Pyne JM, & Stetler C (2012). Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Medical Care, 50, 217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davidson LL, Durkin MS, Kuhn L, O’Connor P, Barlow B, & Heagarty MC (1994). The impact of the Safe Kids/Healthy Neighborhoods Injury Prevention Program in Harlem, 1988 through 1991. American Journal of Public Health, 84, 580–586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dingeldein L, Sheehan K, Krcmarik M, & Dowd MD (2012). Evaluation of a firearm injury prevention web-based curriculum. Teaching and Learning in Medicine, 24, 327–333. [DOI] [PubMed] [Google Scholar]
- Dowd MD (1999). Childhood injury prevention at home and play. Current Opinion in Pediatrics, 11, 578–582. [DOI] [PubMed] [Google Scholar]
- Duncan TK, Waxman K, Romero J, & Diaz G (2014). Operation PeaceWorks: A community program with the participation of a Level II trauma center to decrease gang-related violence. Journal of Trauma and Acute Care Surgery, 76, 1208–1213. [DOI] [PubMed] [Google Scholar]
- DuRant RH, Barkin S, & Krowchuk DP (2001). Evaluation of a peaceful conflict resolution and violence prevention curriculum for sixth-grade students. Journal of Adolescent Health, 28, 386–393. [DOI] [PubMed] [Google Scholar]
- Emde K (2002). Cops & docs: A gun violence injury prevention program. International Journal of Trauma Nursing, 8, 54–56. [DOI] [PubMed] [Google Scholar]
- Fein JA, & Mollen CJ (1999). Interpersonal violence. Current Opinion in Pediatrics, 11, 588–593. [DOI] [PubMed] [Google Scholar]
- Fowler KA, Dahlberg LL, Haileyesus T, Gutierrez C, & Bacon S (2017). Childhood firearm injuries in the United States. Pediatrics, e20163486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garvin EC, Cannuscio CC, & Branas CC (2013). Greening vacant lots to reduce violent crime: A randomised controlled trial. Injury Prevention, 19, 198–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gatheridge BJ, Miltenberger RG, Huneke DF, Satterlund MJ, Mattern AR, Johnson BM, et al. (2004). Comparison of two programs to teach firearm injury prevention skills to 6-and 7-year-old children. Pediatrics, 114, e294–e299. [DOI] [PubMed] [Google Scholar]
- Goldberg AJ, Toto JM, Kulp HR, Lloyd ME, Gaughan JP, Seamon MJ, et al. (2010). An analysis of inner-city students’ attitudes towards violence before and after participation in the “Cradle to Grave” programme. Injury, 41, 110–115. [DOI] [PubMed] [Google Scholar]
- Goldstick JE, Carter PM, Walton MA, Dahlberg LL, Sumner SA, Zimmerman MA, et al. (2017). Development of the SaFETy score: A clinical screening tool for predicting future firearm violence risk. Annals of Internal Medicine, 166, 707–714. 10.7326/M16-1927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green J, Damle RN, Kasper RE, Violano P, Manno M, Nazarey PP, et al. (2017). Are “goods for guns” good for the community? An update of a community gun buyback program. Journal of Trauma and Acute Care Surgery, 83, 284–288. [DOI] [PubMed] [Google Scholar]
- Gross A, Miltenberger R, Knudson P, Bosch A, & Breitwieser CB (2007). Preliminary evaluation of a parent training program to prevent gun play. Journal of Applied Behavior Analysis, 40, 691–695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grossman DC, Cummings P, Koepsell TD, Marshall J, D’Ambrosio L, Thompson RS, et al. (2000). Firearm safety counseling in primary care pediatrics: A randomized, controlled trial. Pediatrics, 106, 22–26. [DOI] [PubMed] [Google Scholar]
- Grossman DC, Stafford HA, Koepsell TD, Hill R, Retzer KD, & Jones W (2012). Improving firearm storage in Alaska native villages: A randomized trial of household gun cabinets. American Journal of Public Health, 102, S291–S297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hardy MS (2002). Teaching firearm safety to children: Failure of a program. Journal of Developmental and Behavioral Pediatrics, 23, 71–76. [DOI] [PubMed] [Google Scholar]
- Hardy MS, Armstrong FD, Martin BL, & Strawn KN (1996). A firearm safety program for children: They just can’t say no. Journal of Developmental and Behavioral Pediatrics: JDBP, 17, 216–221. [PubMed] [Google Scholar]
- Hayes DN, & Sege R (2003). FiGHTS: A preliminary screening tool for adolescent firearms-carrying. Annals of Emergency Medicine, 42, 798–807. [DOI] [PubMed] [Google Scholar]
- Heinze JE, Reischl TM, Bai M, Roche JS, Morrel-Samuels S, Cunningham RM, et al. (2016). A comprehensive prevention approach to reducing assault offenses and assault injuries among youth. Prevention Science: The Official Journal of the Society for Prevention Research, 17, 167–176. 10.1007/s11121-015-0616-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Himle MB, Miltenberger RG, Flessner C, & Gatheridge B (2004a). Teaching safety skills to children to prevent gun play. Journal of Applied Behavior Analysis, 37, 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Himle MB, Miltenberger RG, Gatheridge BJ, & Flessner CA (2004b). An evaluation of two procedures for training skills to prevent gun play in children. Pediatrics, 113, 70–77. [DOI] [PubMed] [Google Scholar]
- Horn A, Grossman DC, Jones W, & Berger L (2003). Community based program to improve firearm storage practices in rural Alaska. Injury Prevention, 9, 231–234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howard PK (2005). Evaluation of age-appropriate firearm safety interventions. Pediatric Emergency Care, 21, 473–479. [DOI] [PubMed] [Google Scholar]
- Howell EM, & Abraham P (2013). The hospital costs of firearm assaults. Washington, DC: Urban Institute. [Google Scholar]
- Kallenborn J Celeste, MBA, Gonzales R. Kathie, BSN, Crane NB, Pesce R. Karen, BSN, Swan R. Sherry, BSN, & Flint L (2004). Cease Fire Tampa Bay: A three-tiered approach to firearm injury prevention. Journal of Trauma Nursing, 11, 6. [DOI] [PubMed] [Google Scholar]
- Jostad CM, & Miltenberger RG (2004). Firearm injury prevention skills: Increasing the efficiency of training with peer tutoring. Child & Family Behavior Therapy, 26, 21–35. [Google Scholar]
- Kasper RE, Green J, Damle RN, Aidlen J, Nazarey P, Manno M, et al. (2017). And the survey said… evaluating rationale for participation in gun buybacks as a tool to encourage higher yields. Journal of Pediatric Surgery, 52(2), 354–359. [DOI] [PubMed] [Google Scholar]
- Kelso PD, Miltenberger RG, Waters MA, Egemo-Helm K, & Bagne AG (2007). Teaching skills to second and third grade children to prevent gun play: A comparison of procedures. Education and Treatment of Children, 30, 29–48. [Google Scholar]
- Kenny MC, & Wurtele SK (2016). Teaching preschoolers safety rules: A pilot study of injury prevention. Children’s Health Care, 45, 428–440. [Google Scholar]
- Komro KA (1999). Adolescents’ access to firearms: Epidemiology and prevention. Journal of Health Education, 30, 290–296. [Google Scholar]
- Kruesi MJ, Grossman J, Pennington JM, Woodward PJ, Duda D, & Hirsch JG (1999). Suicide and violence prevention: Parent education in the emergency department. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 250–255. [DOI] [PubMed] [Google Scholar]
- Kunkel P, Thomas CJ, Seguin C, Dereczyk D, Rajda C, & Brandt M-M (2010). A hospital-based violence prevention tour: A collaborative approach to empower youth. Journal of Trauma and Acute Care Surgery, 68, 289–293. [DOI] [PubMed] [Google Scholar]
- Liller KD, Perrin K, Nearns J, Pesce K, Crane NB, & Gonzalez RR (2003). Evaluation of the “Respect Not Risk” firearm safety lesson for 3rd-graders. The Journal of School Nursing, 19, 338–343. [DOI] [PubMed] [Google Scholar]
- Loh K, Walton MA, Harrison SR, Zimmerman M, Stanley R, Chermack ST, et al. (2010). Prevalence and correlates of handgun access among adolescents seeking care in an urban emergency department. Accident Analysis and Prevention, 42, 347–353. 10.1016/j.aap.2009.11.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGuire M, Manno M, Rook A, Maranda L, Renaud E, DeRoss A, et al. (2011). Goods for guns—the use of a gun buyback as an injury prevention/community education tool. Journal of Trauma and Acute Care Surgery, 71, S537–S540. [DOI] [PubMed] [Google Scholar]
- Milam AJ, Buggs SA, Furr-Holden CDM, Leaf PJ, Bradshaw CP, & Webster D (2016). Changes in attitudes toward guns and shootings following implementation of the Baltimore Safe Streets intervention. Journal of Urban Health, 93, 609–626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miltenberger RG, Gatheridge BJ, Satterlund M, Egemo-Helm KR, Johnson BM, Jostad C, et al. (2005). Teaching safety skills to children to prevent gun play: An evaluation of in situ training. Journal of Applied Behavior Analysis, 38, 395–398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moher D, Liberati A, Tetzlaff J, & Altman DG (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of Internal Medicine, 151, 264–269. [DOI] [PubMed] [Google Scholar]
- Moyer R, MacDonald JM, Ridgeway G, & Branas CC (2019). Effect of remediating blighted vacant land on shootings: A citywide cluster randomized trial. American Journal of Public Health, 109, 140–144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oatis PJ, Buderer NMF, Cummings P, & Fleitz R (1999). Pediatric practice based evaluation of the Steps to Prevent Firearm Injury program. Injury Prevention, 5, 48–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ouzzani M, Hammady H, Fedorowicz Z, & Elmagarmid A (2016). Rayyan: A web and mobile app for systematic reviews. Systematic Reviews, 5, 210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parikh K, Silver A, Patel SJ, Iqbal SF, & Goyal M (2017). Pediatric firearm-related injuries in the United States. Hospital Pediatrics, hpeds. 2016-0146. [DOI] [PubMed] [Google Scholar]
- Regan ME (2009). Implementation and evaluation of a youth violence prevention program for adolescents. The Journal of School Nursing, 25, 27–33. [DOI] [PubMed] [Google Scholar]
- Reich K, Culross PL, & Behrman RE (2002). Children, youth, and gun violence: Analysis and recommendations. The Future of Children, 12, 5–23. [PubMed] [Google Scholar]
- Reischl TM, Zimmerman MA, Morrel-Samuels S, Franzen SP, Faulk M, Eisman AB, et al. (2011). Youth empowerment solutions for violence prevention. Adolescent Medicine-State of the Art Reviews, 22, 581. [PubMed] [Google Scholar]
- Rivara FP, & Fan MD (2017). Pediatricians, firearms, and the First Amendment. JAMA Pediatrics, 171, 723–724. [DOI] [PubMed] [Google Scholar]
- Roberto A, Meyer G, Johnson AJ, Atkin C, & Smith P (2002). Promoting gun trigger-lock use: Insights and implications from a radio-based health communication intervention. Journal of Applied Communication Research, 30, 210–230. [Google Scholar]
- Roszko PJ, Ameli J, Carter PM, Cunningham RM, & Ranney ML (2016). Clinician attitudes, screening practices, and interventions to reduce firearm-related injury. Epidemiologic Reviews, 38, 87–110. 10.1093/epirev/mxv005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rowhani-Rahbar A, Simonetti JA, & Rivara FP (2016). Effectiveness of interventions to promote safe firearm storage. Epidemiologic Reviews, 38, 111–124. [DOI] [PubMed] [Google Scholar]
- Rowhani-Rahbar A, Zatzick D, Wang J, Mills BM, Simonetti JA, Fan MD, et al. (2015). Firearm-related hospitalization and risk for subsequent violent injury, death, or crime perpetration: A cohort study. Annals of Internal Medicine, 162, 492–500. [DOI] [PubMed] [Google Scholar]
- Runyan CW, Becker A, Brandspigel S, Barber C, Trudeau A, & Novins D (2016). Lethal means counseling for parents of youth seeking emergency care for suicidality. Western Journal of Emergency Medicine, 17, 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sangvai S, Cipriani L, Colborn DK, & Wald ER (2007). Studying injury prevention: Practices, problems, and pitfalls in implementation. Clinical Pediatrics, 46, 228–235. [DOI] [PubMed] [Google Scholar]
- Scott J, Azrael D, & Miller M (2018). Firearm storage in homes with children with self-harm risk factors. Pediatrics, e20172600. [DOI] [PubMed] [Google Scholar]
- Sidman EA, Grossman DC, Koepsell TD, D’Ambrosio L, Britt J, Simpson ES, et al. (2005). Evaluation of a community-based handgun safe-storage campaign. Pediatrics, 115, e654–e661. [DOI] [PubMed] [Google Scholar]
- Simonetti JA, Rowhani-Rahbar A, King C, Bennett E, & Rivara FP (2018). Evaluation of a community-based safe firearm and ammunition storage intervention. Injury Prevention, 24, 218–223. [DOI] [PubMed] [Google Scholar]
- Skogan W, Hartnett S, Bump N, & Dubois J (2009). Evaluation of CeaseFire-Chicago. Northwestern University Illinois. Retrieved from https://www.ncjrs.gov/pdffiles1/nij/grants/227181.pdf. Accessed 2 Nov 2018. [Google Scholar]
- Stevens MM, Olson AL, Gaffney CA, Tosteson TD, Mott LA, & Starr P (2002). A pediatric, practice-based, randomized trial of drinking and smoking prevention and bicycle helmet, gun, and seatbelt safety promotion. Pediatrics, 109, 490–497. [DOI] [PubMed] [Google Scholar]
- Thomas SB, Leite B, & Duncan T (1998). Breaking the cycle of violence among youth living in metropolitan Atlanta: A case history of kids alive and loved. Health Education & Behavior, 25, 160–174. [DOI] [PubMed] [Google Scholar]
- Tucker JB, Barone JE, Stewart J, Hogan RJ, Sarnelle JA, & Blackwood MM (1999). Violence prevention: Reaching adolescents with the message. Pediatric Emergency Care, 15, 436–439. [PubMed] [Google Scholar]
- Urie B (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard. [Google Scholar]
- Violano P, Driscoll C, Chaudhary NK, Schuster KM, Davis KA, Borer E, et al. (2014). Gun buyback programs: A venue to eliminate unwanted guns in the community. Journal of Trauma and Acute Care Surgery, 77, S46–S50. [DOI] [PubMed] [Google Scholar]
- Wafer MS, & Carruth A (2003). “Locks for life”: A gun lock distribution community health intervention program. Journal of Emergency Nursing, 29, 349–351. [DOI] [PubMed] [Google Scholar]
- Walton MA, Chermack ST, Shope JT, Bingham CR, Zimmerman MA, Blow FC, et al. (2010). Effects of a brief intervention for reducing violence and alcohol misuse among adolescents: A randomized controlled trial. JAMA, 304, 527–535. 10.1001/jama.2010.1066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wargo C, Erdman DA, Smith JG, Widom K, & Reardon J (2013). Community gun safety in Central Pennsylvania. Journal of Trauma Nursing, 20, 67–73. [DOI] [PubMed] [Google Scholar]
- Whitehill JM, Webster DW, & Vernick JS (2013). Street conflict mediation to prevent youth violence: Conflict characteristics and outcomes. Injury Prevention, 19, 204–209. [DOI] [PubMed] [Google Scholar]
- Williamson AA, Guerra NG, & Tynan WD (2014). The role of health and mental health care providers in gun violence prevention. Clinical Practice in Pediatric Psychology, 2, 88. [Google Scholar]
- Wolk CB, Jager-Hyman S, Marcus SC, Ahmedani BK, Zeber JE, Fein JA, et al. (2017). Developing implementation strategies for firearm safety promotion in paediatric primary care for suicide prevention in two large US health systems: A study protocol for a mixed-methods implementation study. British Medical Journal Open, 7, e014407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolk CB, Van Pelt AE, Jager-Hyman S, Ahmedani BK, Zeber JE, Fein JA, et al. (2018). Stakeholder perspectives on implementing a firearm safety intervention in pediatric primary care as a universal suicide prevention strategy: A qualitative study. JAMA Network Open, 1, e185309–e185309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zatzick D, Russo J, Lord SP, Varley C, Wang J, Berliner L, et al. (2014). Collaborative care intervention targeting violence risk behaviors, substance use, and posttraumatic stress and depressive symptoms in injured adolescents: A randomized clinical trial. JAMA Pediatrics, 168, 532–539. [DOI] [PubMed] [Google Scholar]
- Zimmerman MA, Stewart SE, Morrel-Samuels S, Franzen S, & Reischl TM (2011). Youth empowerment solutions for peaceful communities: Combining theory and practice in a community-level violence prevention curriculum. Health Promotion Practice, 12, 425–439. [DOI] [PubMed] [Google Scholar]