
Figure 3. Arrhythmogenic left ventricular cardiomyopathy and inflammation: case presentations.
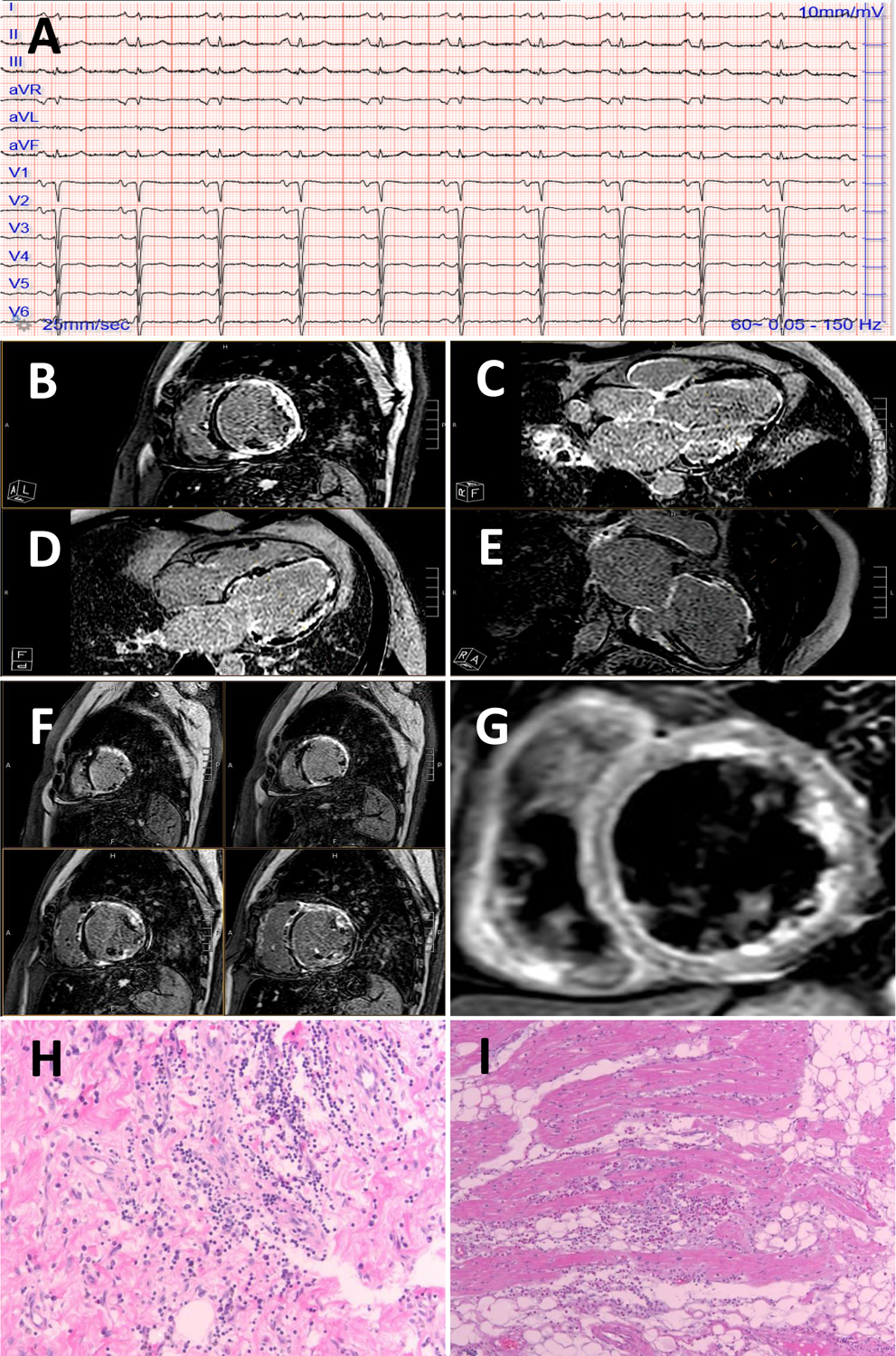
A 49-year-old male with a history of chest pain, troponin elevation, normal epicardial coronary arteries presented several weeks dyspnea, NTproBNP 1500 pg/ml. A 12-lead ECG showed sinus rhythm with T-wave inversion in the lateral leads (I, aVL, V5, V6) and poor R wave progression across the precordial leads (panel A).
A CMR showed extensive left ventricular late gadolinium enhancement with near circumferential ring-like pattern of the basal, mid and apical segments (panels B-F). T2 STIR imaging also showed edema (panel G). An arrhythmogenic cardiomyopathy and dilated cardiomyopathy panel was sent revealing a pathogenic DSP variant c.478C>T (p.Arg160Ter).
An unrelated patient who had died of a sudden cardiac death event on histological analysis showed lymphocytic infiltrates of the left ventricular myocardium (negative for viral PCR), hematoxylin and eosin 10 × panel (H) and magnified 20 × (I). This patient tested positive for a truncating pathogenic DSP variant.