

Abstract
Objective:
We examined whether the largest U.S. poverty alleviation program for families, the earned income tax credit (EITC), has different associations with birthweight among women of different racial backgrounds.
Design:
We analyzed data from the 1985-2015 waves of the Panel Study of Income Dynamics (PSID), a longitudinal cohort study of U.S. families (N=5,230 infants born to 3,672 women). The primary outcome was a continuous measure of birthweight, with secondary outcomes including low birthweight (LBW) and very LBW. Using rich sociodemographic data available in PSID, we calculated the amount of EITC benefit for which women were eligible. We then examined the association of EITC benefit size with each outcome using multivariable regressions, examining the sample overall as well as racial subgroups (White, Black, other).
Results:
We found that larger EITC benefits were not associated with increased infant birthweight for the overall sample (18.37 grams per $1,000 of EITC, 95% CI: −2.62, 33.36). There was an increase in birthweight for Black women (40.17 grams, 95% CI: 7.32, 73.02), but not for White women (−1.86 grams, 95% CI: −33.33, 29.60) or women of other races (−13.26 grams, 95% CI: −75.90, 49.38). There was no association between EITC benefit size and the probability of LBW or very LBW. Results were robust to alternative model specifications.
Conclusion:
Social policies to address poverty may be effective at reducing racial disparities in birthweight. Future work should examine potential mechanisms and the benefits of improved health outcomes for children later in life.
Keywords: racial disparities, birthweight, poverty, earned income tax credit, policy evaluation
INTRODUCTION
In the U.S., Black-White disparities in birthweight are stark. The rates of low birthweight (LBW) births among Black women are almost twice those among non-Hispanic White women (13.7% and 7.0%, respectively) (Martin et al., 2018). These disparities may contribute to racial inequities in later-life health, as low birthweight is associated with increased risk of cardiovascular disease, mental illness, and mortality, as well as later-life educational and economic outcomes (Barker, 1995; Bartley et al., 1994; Black et al., 2005; Braveman & Barclay, 2009; Malat et al., 2005). Research suggests that genetic factors do not explain these disparities, instead implicating current and historic socioeconomic and structural inequities. These may result in a higher burden of adverse birth outcomes among Black women due to chronic stress, and/or the inability to afford or access housing, nutritious food, or healthcare (Braveman et al., 2015; Lu & Chen, 2004; Mehra et al., 2017; Pearl et al., 2018). Indeed, it is increasingly recognized that women’s socioeconomic status during pregnancy is a critically important determinant of birthweight and subsequent child health. Racial inequalities in income and wealth have been identified as one manifestation of structural racism, with important public health ramifications (Bailey et al., 2017; Wallace et al., 2015). Poverty in particular has been repeatedly documented as a risk factor for LBW and other adverse birth outcomes (Bruckner et al., 2013; Hamad & Rehkopf, 2016; Strully et al., 2010). The poverty rate among the U.S. Black population is more than double that of the non-Hispanic White population (20% and 8%, respectively) (KFF, 2018).
Social and economic policies addressing poverty therefore have the potential to reduce Black-White disparities in birth outcomes at the population level by addressing these upstream determinants of health, yet there are few studies that evaluate such interventions. The largest U.S. poverty alleviation program for families with children is the earned income tax credit (EITC), a federal program that provides tax refunds to low-income working families. The average family receives over $3,000 as a lump-sum annual tax refund, with over 25 million families receiving over $60 billion in 2017 (IRS, 2019). Several studies have shown that the EITC has improved economic circumstances of low-income families, reduced poverty, increased labor force participation particularly for single women, and increased health insurance coverage (Baughman, 2012; Chetty et al., 2013; Dahl et al., 2009; Eissa & Hoynes, 2006; Meyer, 2002). There is also evidence that EITC benefits have improved maternal health behaviors, prenatal outcomes, and birth outcomes, including reduced rates of smoking during pregnancy and improved maternal stress levels (Blumenshine et al., 2010; Evans & Garthwaite, 2010; Noonan et al., 2007). In fact, cost-effectiveness analyses of the EITC have shown that state supplements are highly cost-effective and improve health-related quality of life among those with low incomes, with average program costs of $7,786 per quality-adjusted life year for a recipient (Muennig et al., 2016). Importantly, most previous studies used historical data on the EITC prior to 2000. Moreover, the majority were unable to identify EITC-eligible women due to a lack of information on income on birth certificates, instead using proxies like maternal educational attainment.
Prior work also suggests that there may be racial differences in the association of EITC benefits with health. This may be due to racial disparities in knowledge of the EITC, or disproportionately higher reduction of poverty levels among Black recipients (Alegría et al., 2003; Maag, 2005). One study found higher rates of very LBW among Black women receiving the EITC in California, although this study used historical data prior to 2000 and used low educational attainment and Medicaid eligibility as proxies for EITC eligibility (Bruckner et al., 2013). Other prior work has suggested that Black women experience greater benefits in birthweight relative to White women, and the most recent study suggested that state EITC programs, which provide a modest supplemental income boost to the federal EITC benefit, improved birth outcomes, particularly for Black women (Hoynes et al., 2015; Komro et al., 2019).
This study contributes to the literature by examining whether the EITC is associated with infant birthweight differentially across racial subgroups, using recent nationwide granular data from a longitudinal survey of U.S. families. As the EITC is an active area of current policymaking, especially in the wake of economic turmoil due to the COVID-19 pandemic, this evidence may help inform policy discussions and future economic interventions targeting pregnant women to optimize the benefits for birthweight and achieve health equity.
METHODS
Sample
The sample was drawn from the Panel Study of Income Dynamics (PSID), a large nationwide cohort study conducted annually during 1968-1999 and biennially thereafter (PSID, 2017). Details on PSID and the sampling strategy have been described previously (McGonagle et al., 2012). We restricted the sample to children born after 1985, the year in which PSID started collecting information on birthweight. Our analysis included observations through 2015, which was the most recent year available when we commenced the analysis. We also restricted the analysis to children whose mothers were the head of household or the spouse, since data on earned income was not available for other household members. The final sample size was 5,230 infants born to 3,672 women (Figure 1).
Figure 1. Sample flowchart.
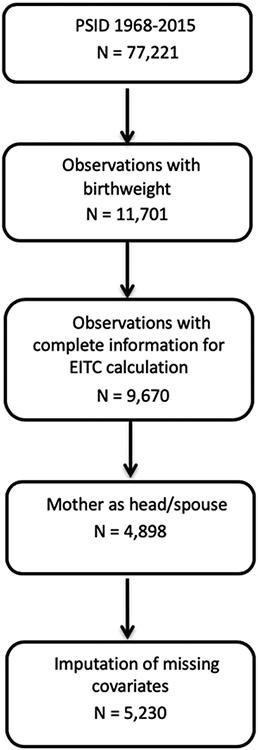
EITC: earned income tax credit; PSID: Panel Study of Income Dynamics.
Exposure
The primary exposure variable was the total EITC benefit amount for which the child’s mother was eligible. As in most national surveys, PSID does not query recipients about EITC receipt. We therefore calculated the EITC benefit amount for which each mother was eligible using Internal Revenue Service (IRS) formulas, implemented using the Taxsim package for Stata (College Station, Texas) (Feenberg & Coutts, 1993). Inputs for these formulas included the household head’s age, marital status, pre-tax earned income, number of children, state of residence, and tax year. This method allows calculation of individual-level EITC benefit amounts and has been used in numerous prior evaluations of the EITC (Dahl & Lochner, 2012; Eissa & Hoynes, 2006; Hamad et al., 2018; Hamad & Rehkopf, 2016; Rehkopf et al., 2014; Schmeiser, 2009). We assumed that all individuals eligible for an EITC benefit actually received it, similar to other studies of the EITC (Dahl et al., 2009; Hamad & Rehkopf, 2016; Hoynes et al., 2015). About 80% of eligible families actually receive the EITC benefit for which they are eligible (IRS, 2017), so this results in some misclassification but is analogous to an intent-to-treat approach. Moreover, our technique is an alternative to—and perhaps an improvement on—prior studies that used only mother’s educational attainment to infer EITC benefit receipt. In our sample, we found that 71.4% of women eligible for the EITC based on Taxsim imputations had less than a high school education, and 40.8% of non-EITC-eligible women had less than a high school education (Supplemental Table S1). Regrettably, neither our study nor prior health evaluations of the EITC have been able to link health data with administrative tax data from the IRS to verify EITC eligibility or receipt, so the results from all of these studies involve some degree of misclassification and should be interpreted with caution.
Outcomes
Birthweight was reported by PSID participants for all children in the household, including for years between surveys. We operationalized this as three outcomes: 1) continuous (grams), 2) LBW (<2500 grams), and 3) very LBW (<1500 grams).
Covariates
We included covariates that represent potential confounders of the relationship between the exposure and outcomes of interest. These included child’s sex, and mother’s age, marital status, education level, number of children, and pre-tax household earned income and income squared (to account for possible non-linear relationships). Income and EITC benefit amount were inflation-adjusted. In analyses in the overall sample, we also adjusted for the race of the household head (White, Black, other). PSID only asks about the race of the household head, and it does not include consistent coding of Hispanic or other racial/ethnic groups across all survey waves. We included fixed effects (i.e., indicator variables) for year to adjust for secular trends. We also included fixed effects for state to adjust for time-invariant unobserved characteristics of states, since states with more generous EITC policies may also have other unobserved characteristics that lead to differences in birth outcomes.
Missing Data
The percent of missing values for covariates ranged from <1% for mother’s age to 4.6% for mother’s education. Of note, PSID gathers information on earned income even during non-survey years, reducing missingness for this key variable. To account for missing values, we performed multiple imputation using chained equations (MICE) with the mi package in Stata. This form of imputation does not require normality assumptions, allowing us to specify a model for a variety of variable types. We assumed data were missing ‘at random’ (as opposed to missing ‘completely at random’) (Paul, 2002). We included all variables including outcomes in imputation models to improve the prediction. We did not, however, impute missing outcomes, as this is thought to add noise to subsequent estimates (Von Hippel, 2007). We produced 50 sets of imputed values, which is sufficient to reduce sampling variability from the imputation process (Horton & Lipsitz, 2001).
STATISTICAL ANALYSES
Primary Analyses
We first tabulated sample characteristics for the overall sample and by race. We then examined the association between each outcome and the EITC benefit amount. To do so, we carried out multivariable regressions controlling for the covariates above. We ran linear models for continuous outcomes and logistic models for binary outcomes. Standard errors were clustered at the level of the mother to account for correlated observations among children with the same mother.
Subgroup Analyses
To determine whether there were differences in the association of the EITC with birth outcomes by race, we conducted subgroup analyses, stratifying our main models by race. To determine whether point estimates from these stratified models were statistically significantly different from one another, we ran an additional analysis for each outcome that included an interaction term between EITC benefit size and race. Given the low number of cases of very LBW among participants of other races (N = 5), we dropped this subgroup from this analysis. We also conducted a stratified analysis with separate models for married and single women to examine if the association of the EITC with birth outcomes differed by marital status. Due to small cell sizes, estimates for very LBW were unstable and this outcome was therefore dropped for this subgroup analysis.
Sensitivity Analyses
We conducted additional analyses to test the robustness of results to alternative specifications. First, we conducted an analysis in which we used only complete cases (i.e., unimputed data). We then carried out an analysis in which the primary exposure was the federal EITC benefit size (i.e., without inclusion of the state EITC benefit), which eliminates any possible confounding by unobserved state characteristics. In a third analysis, we restricted the sample to women with income greater than $0 and less than $100,000, i.e., excluding unemployed and high-income women who may represent inappropriate comparison groups for EITC-eligible women. Because this last sensitivity analysis resulted in a smaller sample size that precluded the ability to conduct subgroup analyses by race, this model was not used as the primary model.
ETHICS APPROVAL
This study involved the use of public deidentified data, so ethics approval was not required.
RESULTS
Sample Characteristics
In the overall sample, roughly 80% of women were married, and about half had completed more than a high school education (Table 1). The average age of women was 28.3 years (SD 5.1), and mean household earned income was $64,020 (SD $60,260). About a fifth of the sample was eligible for the EITC at some point during the study period, with a mean estimated benefit size of $1,937 (SD $1,623).
Table 1.
Sample characteristics
| Variables | Overall N=4,898 Mean (SD) or % (n) |
White N=2,920 Mean (SD) or % (n) |
Black N=1,426 Mean (SD) or % (n) |
Other Race N=552 Mean (SD) or % (n) |
|---|---|---|---|---|
| Sociodemographic Characteristics | ||||
| Child female | 49.4 (2417) | 49.2 (1436) | 50 (713) | 48.6 (268) |
| Mother married | 79.3 (3884) | 92.1 (2689) | 51.9 (740) | 82.4 (455) |
| Mother’s age (years) | 28.3 (5.1) | 28.7 (5.2) | 27.7 (4.9) | 27.9 (5.5) |
| Number of children | 1.0 (1.2) | 0.8 (0.9) | 1.3 (1.3) | 1.3 (1.4) |
| Incomea (USD) | 64,020 (60,260) | 79,538 (64,799) | 36,569 (39,412) | 52,844 (51,582) |
| Mother’s education | ||||
| Less than high school | 12.8 (626) | 7.3 (214) | 18.8 (268) | 26.1 (144) |
| High school | 34.6 (1694) | 31.6 (924) | 40.7 (580) | 34.4 (190) |
| College | 27.8 (1362) | 27.8 (813) | 29.7 (423) | 22.8 (126) |
| More than college | 24.8 (1216) | 33.2 (969) | 10.9 (155) | 16.7 (92) |
| EITC eligible | 21.5 (1051) | 13.0 (379) | 34.6 (493) | 32.4 (179) |
| EITC benefit size (USD) | 1,937 (1,623) | 1,766 (1,589) | 2,047 (1,636) | 1,906 (1,619) |
| Health Outcomes | ||||
| Birthweight (grams) | 3,339 (604) | 3,426 (574) | 3,153 (638) | 3,358 (564) |
| Low birthweight | 7.6 (370) | 4.9 (142) | 13.6 (194) | 6.2 (34) |
| Very low birthweight | 0.9 (42) | 0.4 (12) | 1.9 (27) | 0.5 (3) |
Note: The study sample was drawn from the Panel Study of Income Dynamics for survey years 1985-2015. Sample characteristics were calculated using unimputed data (N=4,898). EITC: earned income tax credit.
Inflation-adjusted household pre-tax earned income
Black women were more likely to be unmarried, with larger households and lower income relative to White women. They were also more likely to qualify for the EITC, and those who qualified were eligible for larger benefits. Black women were also more likely to have infants with lower birthweights compared with other women.
In terms of variation in the exposure, the size of the EITC benefit has grown over time, and families with two or more children were eligible for larger benefits after major expansions to the federal EITC in the early 1990s (Figure S1).
EITC and Birthweight
Eligibility for larger EITC benefits was associated with increased birthweight (18.37 grams per $1,000, 95%CI: −2.62, 39.37) although the 95% confidence interval included the null (Figure 2). There was an increase in birthweight for Black women (40.17 grams, 95% CI: 7.32, 73.03), but not for White women (−1.86 grams, 95%CI: −33.33, 29.61) or women of other races (−13.26 grams, 95%CI: −75.90, 49.38). The estimate for Black women was also statistically significantly different from the estimates for White women and women of other races. There was no association between EITC benefit size and the probability of LBW or very LBW in the sample overall or among racial subgroups (Figures 3 and 4). Results for all outcomes were similar for single and married women (Supplemental Table S4).
Figure 2. Association of the earned income tax credit with continuous birthweight, Panel Study of Income Dynamics, 1985-2015.
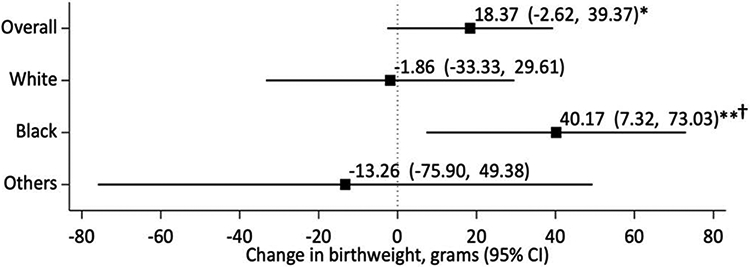
* p < 0.10 and ** p < 0.05 from overall/stratified models; † p < 0.05 on the interaction term between race and EITC benefit size, indicating that the estimate is statistically significantly different than the reference group (White women).
N = 5,230. Sample was drawn from the Panel Study of Income Dynamics for survey years 1985-2015. Coefficients represent the association between EITC and the outcome per $1,000 of EITC benefit. Estimates for White, Black, and other races represent stratified results by race. EITC: earned income tax credit.
Figure 3. Association of the earned income tax credit with low birthweight, Panel Study of Income Dynamics, 1985-2015.
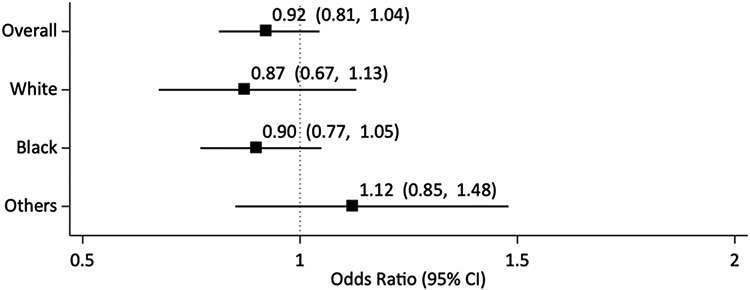
N = 5,120. Sample was drawn from the Panel Study of Income Dynamics for survey years 1985-2015. Coefficients represent the association between EITC and the outcome per $1,000 of EITC benefit. Estimates for White, Black, and other races represent stratified results by race. EITC: earned income tax credit.
Figure 4. Association of the earned income tax credit with very low birthweight, Panel Study of Income Dynamics, 1985-2015.
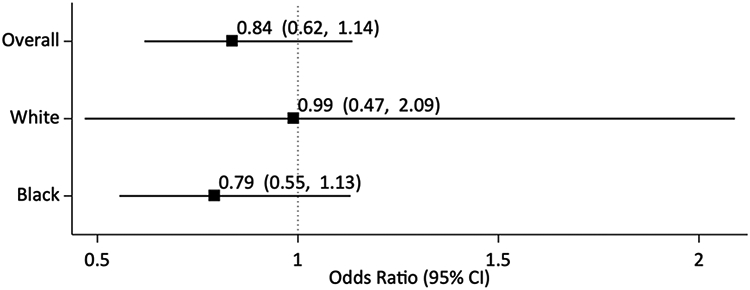
N = 2,945. Sample was drawn from the Panel Study of Income Dynamics for survey years 1985-2015. Coefficients represent the association between EITC and the outcome per $1,000 of EITC benefit. Estimates for White and Black represent stratified results by race. EITC: earned income tax credit.
Sensitivity Analyses
Using complete cases (i.e., unimputed data), we found similar results as in the primary models: EITC benefits were associated with increased birthweight in the overall sample (18.76 grams per $1,000, 95%CI: −2.43, 39.96), although the 95% confidence interval included the null (Supplementary Table S2). Similarly, there was an increase in birthweight for Black women (41.70 grams, 95%CI: 9.32, 74.07), but not for White women (−2.34 grams, 95%CI: −35.51, 30.83) or women of other races (−15.95 grams, 95%CI: −78.27, 46.37). Similar to the primary models, there was no association between EITC benefit size and the probability of LBW or very LBW using complete cases.
When we limited our exposure to the federal EITC only (Model 1, Supplementary Table S3) we found a similar effect size as in our primary models, but with wider confidence intervals (17.15 grams, 95%CI: −4.86, 39.16). In our analysis restricting the sample to those with earned income greater than $0 and less than $100,000, larger EITC benefit size was again associated with increased birthweight (23.99 grams, 95%CI: 2.19, 45.79).
DISCUSSION
In this study, we examined the association of the EITC—the largest U.S. poverty alleviation program for families with children—with racial disparities in birthweight. We found that eligibility for greater EITC benefits was associated with higher birthweight in the overall sample. This is consistent with previous studies of the EITC, although prior analyses typically used historical data prior to 2000 and inferred EITC eligibility using educational attainment alone (Bruckner et al., 2013; Hoynes et al., 2015; Strully et al., 2010). Our analyses suggest that the benefits of the EITC have persisted in more recent decades, despite changes to the national political and economic context. Importantly, we also found that benefits were larger for Black women. Because Black women have higher rates of low birthweight, this suggests that the EITC or similar programs have the potential to address racial disparities in birth outcomes at the population level. These findings contrast with one older study in California, which found that the EITC was associated with an increased risk of very LBW among Black women, although they are consistent with one older study of the federal EITC and another recent study of state EITC programs that found larger benefits for Black women (Bruckner et al., 2013; Hoynes et al., 2015; Komro et al., 2019).
Observed associations were also stronger when we limited the sample to those households making more than $0 and less than $100,000 in annual income. This is likely a more fitting comparison group, as higher income individuals are less likely to be exposed to financial stress, and unemployed individuals may not represent an appropriate control group for EITC recipients. Notably, we found increased birthweight only when we examined it as a continuous measure, but no association with LBW and very LBW, in contrast to prior work. It may be that the effects of the EITC on birthweight were modest and therefore not large enough to change the distribution of LBW and very LBW risk. Alternately, this may have been a result of reduced power when dichotomizing the outcome, or because our sample is smaller than those in prior studies that have examined the effects of the EITC on LBW (Hoynes et al., 2015).
There are several mechanisms that may explain our findings. Prior work suggests that stress during pregnancy may lead to reduced birthweight, and it may be that the EITC improves mental health (Lobel et al., 2008; Strutz et al., 2014; Wadhwa et al., 1993); two recent studies suggest that this is the case, although these did not focus on pregnant women specifically (Boyd-Swan et al., 2016; Dow et al., 2019). Second, income from the EITC has also been shown to reduce food insufficiency and housing instability, both of which are risk factors for reduced birthweight (Pilkauskas & Michelmore, 2019; Rehkopf et al., 2014). Since Black women in the U.S. have higher rates of poverty and lower wealth due to structural inequities, it may be that the income boost from the EITC is even more impactful. Finally, greater income may increase access to healthcare; while a single study of the EITC recently found no association with short-term healthcare utilization, it did not focus on pregnant women (Hamad & Niedzwiecki, 2019). Since PSID does not include information on these mediating pathways, future studies can examine which of these mechanisms may explain the association between poverty alleviation and birthweight.
Our study has several strengths. First, we used three decades of data, including more recent years through 2015. This helps to provide more contemporary and relevant evidence of the effects of EITC on birthweight. Second, our use of detailed sociodemographic data from the PSID allowed us to impute EITC using more granular information than prior work.
Our study also has several limitations. First, we used self-reported outcomes and income, which may introduce measurement error into our findings. Second, we assumed that all families received the EITC benefit for which they were eligible; since roughly 80% of eligible families actually receive their EITC benefits, this may introduce measurement error into our analyses, but it is also analogous to an intent-to-treat analysis and a technique commonly used in the prior literature (Dahl & Lochner, 2012; Hamad & Rehkopf, 2015, 2016; Rehkopf et al., 2014). Third, our main analysis may be confounded due to state-level characteristics that affect both EITC generosity and birthweight, although our findings were robust to a sensitivity analysis in which we used only federal EITC benefit size as the exposure. Also, the EITC may influence birthweight through multiple mechanisms, e.g., providing income to purchase necessary resources, reducing stress related to poverty, incentivizing employment, and altering fertility. Our study does not tease apart which mechanism is more important for birth outcomes—in part due to limited information on these mechanisms in PSID—but rather provides evidence about the policy more holistically. Therefore, evidence from this study should be combined with evidence from evaluations of different financial interventions—e.g., basic income that is not contingent on employment—to distinguish these pathways. Additionally, PSID is limited in that it does not include information on gestational age at birth for all births, which prevents us from distinguishing LBW due to intrauterine growth restriction rather than shortened length of the pregnancy (i.e., preterm birth). Finally, it may be that subgroup analyses are underpowered, particularly for binary outcomes; nevertheless, larger data sets used in prior work (e.g., birth certificate data) are limited in the sociodemographic information available on participants, representing a trade-off between sample size and measurement error of the EITC exposure.
Implications for Practice and/or Policy
The EITC is among the largest poverty alleviation programs in the U.S. Recent policy proposals primarily focus on expanding the program for tax filers without children (Maag, 2020), even though a recent National Academy of Sciences report on child poverty explicitly recommends increasing investment in the EITC to support children (National Academies of Sciences Engineering and Medicine, 2019). Our study and others provide further evidence on the importance of the EITC for low-income families, and particularly for women of color who have been historically structurally and economically marginalized. Moreover, studies have found that only 80% of eligible families receive the benefits for which they are eligible (Jones, 2013), suggesting that there is room for improving take-up of the program to expand its benefits among vulnerable groups. With the COVID-19 pandemic, racial and economic disparities have widened, and federal and state EITC expansions may help to reduce these growing gaps in birth outcomes, especially for Black women.
CONCLUSIONS
In this study, we used contemporary nationwide data with granular information on sociodemographic characteristics and showed that the largest U.S. poverty alleviation policy has the potential to improve birthweight and in particular reduce Black-White disparities in birthweight. This evidence informs ongoing policymaking related to the EITC at the federal and state levels and is particularly relevant in the wake of the socioeconomic upheaval of the Covid-19 pandemic. Future research could extend this work to examine potential mechanisms by which raising incomes raises birthweights among Black women and investigate whether reduced racial disparities in adverse birth outcomes translate into improved child health.
Supplementary Material
Funding Statement
This work was supported by the National Institutes of Health (grant number K08-HL132106), the UCSF National Center of Excellence in Women’s Health, and the UCSF California Preterm Birth Initiative. The collection of Panel Study of Income Dynamics data used in this study was partly supported by the National Institutes of Health (grant number R01 HD069609 & R01 AG040213), and the National Science Foundation (award numbers SES 1157698 & 1623684).
Footnotes
DECLARATION OF INTEREST STATEMENT
The authors have no conflict of interest.
REFERENCES
- Alegría M, Pérez DJ, & Williams S (2003). The Role Of Public Policies In Reducing Mental Health Status Disparities For People Of Color. Health Affairs, 22(5), 51–64. 10.1377/hlthaff.22.5.51 [DOI] [PubMed] [Google Scholar]
- Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, & Bassett MT (2017). Structural racism and health inequities in the USA: evidence and interventions. The Lancet, 389(10077), 1453–1463. 10.1016/S0140-6736(17)30569-X [DOI] [PubMed] [Google Scholar]
- Barker DJ (1995). Fetal origins of coronary heart disease. BMJ, 311(6998), 171–174. 10.1136/bmj.311.6998.171 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bartley M, Power C, Blane D, Smith GD, & Shipley M (1994). Birth weight and later socioeconomic disadvantage: evidence from the 1958 British cohort study. BMJ, 309(6967), 1475–1478. 10.1136/bmj.309.6967.1475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baughman RA (2012). The Effects of State EITC Expansion on Children’s Health 48). C. Institute. [Google Scholar]
- Black SE, Devereux PJ, & Salvanes K (2005). From the Cradle to the Labor Market? The Effect of Birth Weight on Adult Outcomes. National Bureau of Economic Research Working Paper Series, No. 11796. 10.3386/w11796 [DOI] [Google Scholar]
- Blumenshine P, Egerter S, Barclay CJ, Cubbin C, & Braveman PA (2010). Socioeconomic Disparities in Adverse Birth Outcomes: A Systematic Review. American Journal of Preventive Medicine, 39(3), 263–272. https://doi.org/ 10.1016/j.amepre.2010.05.012 [DOI] [PubMed] [Google Scholar]
- Boyd-Swan C, Herbst CM, Ifcher J, & Zarghamee H (2016). The earned income tax credit, mental health, and happiness. Journal of Economic Behavior & Organization, 126, 18–38. https://doi.org/ 10.1016/j.jebo.2015.11.004 [DOI] [Google Scholar]
- Braveman P, & Barclay C (2009). Health Disparities Beginning in Childhood: A Life-Course Perspective. Pediatrics, 124(Supplement 3), S163. 10.1542/peds.2009-1100D [DOI] [PubMed] [Google Scholar]
- Braveman PA, Heck K, Egerter S, Marchi KS, Dominguez TP, Cubbin C, … Curtis M (2015). The role of socioeconomic factors in Black-White disparities in preterm birth. American journal of public health, 105(4), 694–702. 10.2105/AJPH.2014.302008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruckner TA, Rehkopf DH, & Catalano RA (2013). Income Gains and Very Low-Weight Birth among Low-Income Black Mothers in California. Biodemography and social biology, 59(2), 141–156. [DOI] [PubMed] [Google Scholar]
- Chetty R, Friedman JN, & Saez E (2013). Using Differences in Knowledge across Neighborhoods to Uncover the Impacts of the EITC on Earnings. American Economic Review, 103(7), 2683–2721. 10.1257/aer.103.7.2683 [DOI] [Google Scholar]
- Dahl GB, & Lochner L (2012). The Impact of Family Income on Child Achievement: Evidence from the Earned Income Tax Credit. The American Economic Review, 102(5), 1927–1956. [Google Scholar]
- Dahl M, Deleire T, & Schwabish J (2009). Stepping Stone or Dead End? The Effect of the EITC on Earnings Growth. National Tax Journal, 62. 10.17310/ntj.2009.2.06 [DOI] [Google Scholar]
- Dow WH, Godøy A, Lowenstein CA, & Reich M (2019). Can Economic Policies Reduce Deaths of Despair? National Bureau of Economic Research Working Paper Series, No. 25787. 10.3386/w25787 [DOI] [Google Scholar]
- Eissa N, & Hoynes HW (2006). Behavioral Responses to Taxes: Lessons from the EITC and Labor Supply. Tax Policy and the Economy, 20, 73–110. 10.1086/tpe.20.20061905 [DOI] [Google Scholar]
- Evans WN, & Garthwaite CL (2010). Giving Mom a Break: The Impact of Higher EITC Payments on Maternal Health. National Bureau of Economic Research Working Paper Series, No. 16296. 10.3386/w16296 [DOI] [Google Scholar]
- Feenberg D, & Coutts E (1993). An Introduction to the TAXSIM Model. Journal of Policy Analysis and Management, 12(1), 189–194. [Google Scholar]
- Hamad R, Collin DF, & Rehkopf DH (2018). Estimating the Short-Term Effects of the Earned Income Tax Credit on Child Health. American journal of epidemiology, 187(12), 2633–2641. 10.1093/aje/kwy179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamad R, & Niedzwiecki MJ (2019). The short-term effects of the earned income tax credit on health care expenditures among US adults. Health Services Research, 54(6), 1295–1304. 10.1111/1475-6773.13204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamad R, & Rehkopf DH (2015). Poverty, Pregnancy, and Birth Outcomes: A Study of the Earned Income Tax Credit. Paediatric and Perinatal Epidemiology, 29(5), 444–452. 10.1111/ppe.12211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamad R, & Rehkopf DH (2016). Poverty and Child Development: A Longitudinal Study of the Impact of the Earned Income Tax Credit. American journal of epidemiology, 183(9), 775–784. 10.1093/aje/kwv317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horton NJ, & Lipsitz SR (2001). Multiple Imputation in Practice. The American Statistician, 55(3), 244–254. 10.1198/000313001317098266 [DOI] [Google Scholar]
- Hoynes H, Miller D, & Simon D (2015). Income, the Earned Income Tax Credit, and Infant Health. American Economic Journal: Economic Policy, 7(1), 172–211. 10.1257/pol.20120179 [DOI] [Google Scholar]
- IRS. (2017). EITC Participation Rate by States ∣ EITC & Other Refundable Credits [Google Scholar]
- IRS. (2019). EITC Fast Facts ∣ EITC & Other Refundable Credits [Google Scholar]
- Jones MR (2013). Changes in EITC eligibility and participation, 2005-2009. Tax Administration at the Centennial: An IRS-TPC Research Conference, Washington, D.C. [Google Scholar]
- KFF. (2018). Poverty Rate by Race/Ethnicity [Google Scholar]
- Komro KA, Markowitz S, Livingston MD, & Wagenaar AC (2019). Effects of State-Level Earned Income Tax Credit Laws on Birth Outcomes by Race and Ethnicity. Health equity, 3(1), 61–67. 10.1089/heq.2018.0061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lobel M, Cannella DL, Graham JE, DeVincent C, Schneider J, & Meyer BA (2008). Pregnancy-specific stress, prenatal health behaviors, and birth outcomes. Health Psychology, 27(5), 604–615. 10.1037/a0013242 [DOI] [PubMed] [Google Scholar]
- Lu MC, & Chen B (2004). Racial and ethnic disparities in preterm birth: The role of stressful life events. American Journal of Obstetrics and Gynecology, 191(3), 691–699. https://doi.org/ 10.1016/j.ajog.2004.04.018 [DOI] [PubMed] [Google Scholar]
- Maag E (2005). Disparities in knowledge of the EITC. [Google Scholar]
- Maag E (2020). HEROES Act Would Expand The EITC For Childless Workers And Help Fight Recession. https://www.taxpolicycenter.org/taxvox/heroes-act-would-expand-eitc-childless-workers-and-help-fight-recession [Google Scholar]
- Malat J, Oh HJ, & Hamilton MA (2005). Poverty experience, race, and child health. Public health reports, 120(4), 442–447. 10.1177/003335490512000411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, & Drake P (2018). Births: Final data for 2016 (National Vital Statistics Reports, Issue. https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_01.pdf [PubMed] [Google Scholar]
- McGonagle KA, Schoeni RF, Sastry N, & Freedman VA (2012). The Panel Study of Income Dynamics: Overview, Recent Innovations, and Potential for Life Course Research. Longitudinal and life course studies, 3(2), 188. 10.14301/llcs.v3i2.188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehra R, Boyd LM, & Ickovics JR (2017). Racial residential segregation and adverse birth outcomes: A systematic review and meta-analysis. Social Science & Medicine, 191, 237–250. https://doi.org/ 10.1016/j.socscimed.2017.09.018 [DOI] [PubMed] [Google Scholar]
- Meyer BD (2002). Labor Supply at the Extensive and Intensive Margins: The EITC, Welfare, and Hours Worked. The American Economic Review, 92(2), 373–379. [Google Scholar]
- Muennig PA, Mohit B, Wu J, Jia H, & Rosen Z (2016). Cost Effectiveness of the Earned Income Tax Credit as a Health Policy Investment. American Journal of Preventive Medicine, 51(6), 874–881. 10.1016/j.amepre.2016.07.001 [DOI] [PubMed] [Google Scholar]
- National Academies of Sciences Engineering and Medicine. (2019). A Roadmap to Reducing Child Poverty. The National Academies Press. 10.17226/25246 [DOI] [PubMed] [Google Scholar]
- Noonan MC, Smith SS, & Corcoran ME (2007). Examining the impact of welfare reform, labor market conditions, and the Earned Income Tax Credit on the employment of black and white single mothers. Social Science Research, 36(1), 95–130. https://doi.org/ 10.1016/j.ssresearch.2005.09.004 [DOI] [Google Scholar]
- Paul DA (2002). Missing Data 10.4135/9781412985079 [DOI] [Google Scholar]
- Pearl M, Ahern J, Hubbard A, Laraia B, Shrimali BP, Poon V, & Kharrazi M (2018). Life-course neighbourhood opportunity and racial-ethnic disparities in risk of preterm birth. Paediatric and Perinatal Epidemiology, 32(5), 412–419. 10.1111/ppe.12482 [DOI] [PubMed] [Google Scholar]
- Pilkauskas N, & Michelmore K (2019). The Effect of the Earned Income Tax Credit on Housing and Living Arrangements. Demography, 56(4), 1303–1326. 10.1007/s13524-019-00791-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- PSID. (2017). Panel Study of Income Dynamics, public use dataset. [Google Scholar]
- Rehkopf DH, Strully KW, & Dow WH (2014). The short-term impacts of Earned Income Tax Credit disbursement on health. International journal of epidemiology, 43(6), 1884–1894. 10.1093/ije/dyu172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmeiser MD (2009). Expanding wallets and waistlines: the impact of family income on the BMI of women and men eligible for the Earned Income Tax Credit. Health Economics, 18(11), 1277–1294. 10.1002/hec.1430 [DOI] [PubMed] [Google Scholar]
- Strully KW, Rehkopf DH, & Xuan Z (2010). Effects of Prenatal Poverty on Infant Health: State Earned Income Tax Credits and Birth Weight. American sociological review, 75(4), 534–562. 10.1177/0003122410374086 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strutz KL, Hogan VK, Siega-Riz AM, Suchindran CM, Halpern CT, & Hussey JM (2014). Preconception Stress, Birth Weight, and Birth Weight Disparities Among US Women. American Journal of Public Health, 104(8), e125–e132. 10.2105/AJPH.2014.301904 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Von Hippel PT (2007). Regression with missing Ys: An improved strategy for analyzing multiply imputed data. Sociological Methodology, 37(1), 83–117. [Google Scholar]
- Wadhwa PD, Sandman CA, Porto M, Dunkel-Schetter C, & Garite TJ (1993). The association between prenatal stress and infant birth weight and gestational age at birth: A prospective investigation. American Journal of Obstetrics & Gynecology, 169(4), 858–865. 10.1016/0002-9378(93)90016-C [DOI] [PubMed] [Google Scholar]
- Wallace ME, Mendola P, Liu D, & Grantz KL (2015). Joint Effects of Structural Racism and Income Inequality on Small-for-Gestational-Age Birth. American journal of public health, 105(8), 1681–1688. 10.2105/AJPH.2015.302613 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.