
Fig. 7. TNNT2-4Fpolycistronic-NIL maintained improvement in cardiac function for four months.
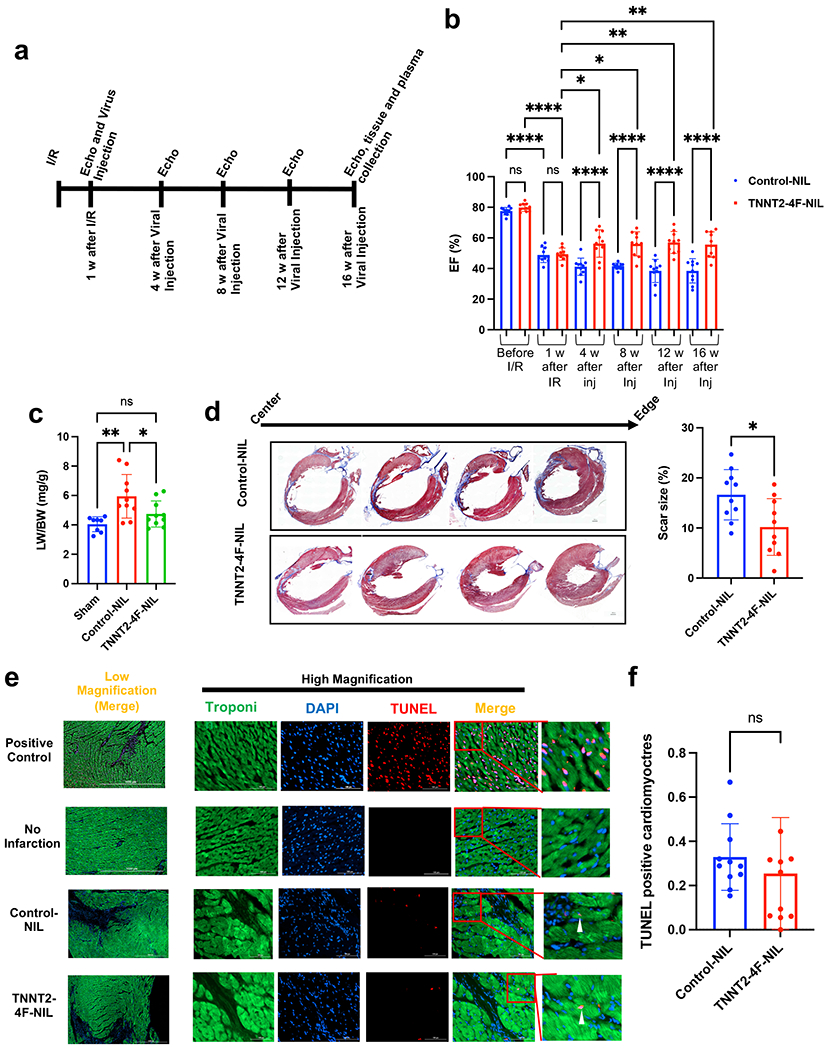
(a) schematic diagram of the experimental design. (b) Ejection fraction (EF), as assessed by echocardiography before ischemia/reperfusion (I/R), one week after I/R (before viral treatment), and every four weeks after viral treatment up to 16 weeks. (n=10 rats per group, *p<0.05, **p<0.01, ****p<0.0001, compared to GFP-NIL control group, error bars indicate the S.D.). (c) Quantification of the lung weight/body weight (LW/BW) (n=8-10 rats per group, *p<0.05, compared to GFP-NIL control group). (d) Representative images of rat hearts were stained with Masson’s trichrome stain (left panel) (healthy myocardium stains red and fibrotic tissue stains blue) at the end of the experiment (scale bar=2mm). The right panel shows scar size quantification as a percentage of total heart tissue (n=10 rats per group, 20-25 heart sections per animal, **p<0.01 compared to the control group, error bars indicate S.D.). (e) Representative images of rat hearts at the border zone stained for apoptotic nuclei using TUNEL assay (red), Troponin-T (green), and nuclear DAPI (blue) (scale bar=1000 µm in the low magnification images and 100 µm in the high magnification images). Positive control was carried out by treating the non-infarct heart section with the DNase-I enzyme. (f) Quantification of the percentage of TUNEL positive cardiomyocytes (n=10 heart sections per animal and 10 animals in each group, error bars indicate S.D.).