

Abstract
Objectives:
The aim of this study was to determine the frequency of seborrheic dermatitis (SD) by months and seasons in Istanbul, Turkey, and to examine the relationships between SD frequency and meteorological data, such as average temperature (°C), average humidity (%), average sunshine duration, and solar radiation per months.
Methods:
The study was conducted at Dermatology Department of Haseki Training and Research Hospital. The data of all adult patients who applied to the dermatology outpatient clinic between June 2018 and May 2020 were obtained. Monthly average climate data values of Istanbul between the same period were requested from the Turkish Ministry of Agriculture and Forestry, General Directorate of Meteorology.
Results:
During the study period, SD was diagnosed in 5316 patients (5.9% of the outpatient clinic). Among these, 2721 (51.2%) were male, 2595 (48.8%) were female, and mean age was 35.9±15.1 years-old. With respect to monthly distributions, SD frequency was 7.3% in December, 7.1% in February, 6.7% in November, and 6.6% in January; whereas June (3.8%) and July (3.9%) represented the lowest proportion of patients. Frequency of SD was similar in the autumn and winter seasons, despite considerable difference in average temperature. The frequency of SD was found to be strongly and inversely correlated with temperature values (r=–0,646, p<0.001) and monthly maximum humidity value (r=–0.609, p=0.001), while it was also moderately correlated with solar radiation levels (r=–0.442, p=0.027). Minimum or average humidity values and sunshine durations (daily and monthly) were not associated with frequency of SD. Spearman’s Rho correlation was calculated to assess the directional relationships between continuous variables.
Conclusion:
Our study shows that environmental factors such as low temperature, low ultraviolet index, and low humidity are critical factors that increase the likelihood of SD development. These data support previous studies in terms of indicating that SD frequency might be increased in climate conditions favoring the growth of Malassezia species.
Keywords: Climate, Humidity, Seborrheic dermatitis, Temperature
Seborrheic dermatitis (SD), also called seborrheic eczema, is a chronic skin condition seen in all ages which causes patches of scaly, flaking lesions localized on the scalp, face, and oily regions of the body.[1] Dandruff is a characteristic outcome of SD of the scalp and may be the only symptom when SD is minimal and limited to this region.[2] SD is usually identified as a red scaly rash covering the sebaceous regions of the forehead, scalp, upper chest, and back; but the appearance can differ, particularly in infants (cradle cap) and with respect to individual skin properties.[2] Although severe SD frequency is relatively low, SD and dandruff are estimated to affect half of the adult population;[3] however, its etiology is not well described.[1]
In addition to patient-related features, such as age and gender, geographical differences have some influence on the clinical profile of the disease. Relatively recent evidence suggests that Malassezia species may be closely related to the development of SD, since these microorganisms are favored by the increased lipid levels in skin with seborrheic glands.[4] Previously identified factors associated with SD prevalence are stress, smoking, hypertension, HIV, Parkinson’s disease, obesity, immunosuppression, and environmental properties especially climate factors such as humidity and temperature.[5]
Some studies have been carried out to ascertain the relationship between seasonal factors and various skin diseases.[6] It is well-established that SD severity may vary over time,[7] and a recent study found that SD appeared to demonstrate an increasing frequency in light-skin populations during the winter. The authors concluded that the symptoms show an increase in winter due to xerosis, diminished barrier activity and the absence of protective effects of ultraviolet (UV) rays.[5] However, data are limited concerning the effects of seasonal variables on the frequency of SD.[5]
In this study, we aim to determine the frequency of SD by months and seasons in a Turkish population, and to examine the relationship between SD frequency and meteorological data such as average temperature (°C), average humidity (%), average sunshine duration per day, and maximum global solar radiation per months.
Methods
The study was conducted at the Dermatology Department of Haseki Training and Research Hospital. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Clinical Studies Ethical Committee of Haseki Training and Research Hospital (No: 200, Date: 04.06.2020). The data of all patients who applied to the dermatology outpatient clinic (≥18 years-old) between June 2018 and May 2020 were obtained and reviewed from electronic health record systems retrospectively. Frequency was calculated per months as the ratio of the number of patients with SD to the total number of patients admitted to the outpatient clinic in the specified 2-years period.
SD was diagnosed with the presence of oily scaling and erythema in the typical distribution regions of SD – skin rich in sebaceous glands by the Dermatologist in our outpatient-clinic. The diagnosis of SD was excluded in patients identified to have findings conclusive for any other dermatologic disease and those with skin manifestations of other diseases resembling SD.
The climate dataset was obtained by requesting the monthly climate data records between June 2018 and May 2020 from the Turkish Ministry of Agriculture and Forestry, General Directorate of Meteorology. All data provided were specific to the Istanbul region. The parameters assessed and evaluated in the current study included the following: monthly minimum temperature (°C), monthly maximum temperature (°C), monthly average temperature (°C), monthly minimum humidity (%), monthly maximum humidity (%), monthly average humidity (%), total hours of sunshine per month (hours), average hours of sunshine per day (hours), and monthly max sphering solar radiation (UV index, Kilowatt/m2).
Statistical Analysis
For descriptive statistical analyses, mean±standard deviation values were provided for continuous variables. Categorical variables were presented as count (n) with percentage (%). Spearman's Rho correlation was calculated to assess the directional relationships between continuous variables. Any p<0.05 was considered statistically significant. Statistical analyses were performed using the SPSS version 15.0 statistics software (SPSS Inc., Chicago, IL, USA).
Results
A total of 90805 patients who were admitted to the dermatology out-patient clinic throughout the study period were assessed. SD was diagnosed in 5316 patients (5.9%) (Mean age: 35.9±15.1 years (range 18–92) of whom 2721 (51.2%) were male and 2595 (48.8%) were female.
The distribution of SD diagnoses by months is presented in Table 1. The highest frequency for SD was in December with 670 diagnoses (7.3%), followed by February (608, 7.1%), November (659, 6.7%), and January (596, 6.6%). Months with the lowest SD frequency were June (199, 3.8%) and July (259, 3.9%). According to the seasons, the distribution of SD cases was as follows: 35.3% were identified in the winter, 32.9% in the autumn, 18.3% in the spring, and 13.5% in the summer (Fig. 1). The frequency of SD with respect to climate data, including temperature (°C), humidity (%), average sunshine duration (hours/day), average UV index (watts/m2) by months, and the frequency of SD by months with respect to climate database findings are presented in Table 1. The frequency of SD was negatively correlated with temperature values (minimum, maximum, and average), maximum humidity, and UV index. The parameters that had the strongest correlations with SD frequency were: minimum temperature (r=–0.648, p<0.001), average temperature (r=–0.646, p<0.001), and maximum humidity (r=–0.609, p=0.001). Correlations were insignificant for minimum and average humidity values and sunshine durations (Table 2).
Figure 1.
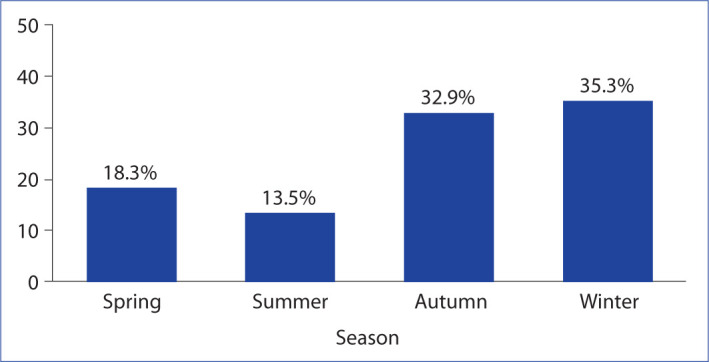
Distribution of seborrheic dermatitis with respect to seasons.
Table 1.
Seborrheic dermatitis frequency by months with respect to climate database findings
| Months | Frequency | Monthly min | Monthly max | Monthly mean | Monthly min | Monthly max | Monthly mean | Total hours of | Average hours | Monthly max |
|---|---|---|---|---|---|---|---|---|---|---|
| temperature | temperature | temperature | humidity | humidity | humidity | sunshine per | of sunshine | sphering solar | ||
| (°C) | (°C) | (°C) | (%) | (%) | (%) | month | per day | radiation (KW/m2) | ||
| January | 6.6 | –0.4 | 16.2 | 7.3 | 32.0 | 99.5 | 80.9 | 110.7 | 3.6 | 165.3 |
| February | 7.1 | –0.7 | 21.0 | 8.0 | 25.5 | 99.5 | 80.3 | 157.3 | 5.5 | 251.7 |
| March | 6.4 | 1.3 | 23.8 | 10.4 | 18.0 | 99.5 | 74.9 | 225.2 | 7.3 | 338.9 |
| April | 5.6 | 4.7 | 27.0 | 12.4 | 11.0 | 99.5 | 70.0 | 256.5 | 8.6 | 444.9 |
| May | 5.9 | 9.7 | 32.5 | 18.8 | 13.3 | 99.7 | 69.5 | 305.4 | 9.9 | 491.3 |
| June | 3.8 | 15.6 | 33.6 | 23.7 | 12.7 | 99.7 | 72.9 | 235.1 | 7.8 | 469.4 |
| July | 3.9 | 18.0 | 33.9 | 25.1 | 14.5 | 100 | 59.4 | 329.4 | 10.7 | 477.6 |
| August | 4. | 19.1 | 33.0 | 25.7 | 16.0 | 100 | 69.6 | 297.9 | 9.6 | 434.8 |
| September | 5. | 12.7 | 32.3 | 22.1 | 18.0 | 100 | 69.4 | 244.2 | 8.2 | 354.9 |
| October | 5.8 | 9.9 | 29.5 | 18.1 | 30.0 | 99.5 | 82.0 | 200.7 | 6.5 | 282.9 |
| November | 6.7 | 6.4 | 24.8 | 14.9 | 37.5 | 99.5 | 82.3 | 140.8 | 4.7 | 194.7 |
| December | 7.3 | 1.4 | 18.3 | 9.1 | 39.5 | 99.5 | 83.4 | 89.3 | 2.9 | 138.6 |
| Total (within 2-year period) | 5.9 | 8.5 | 27.6 | 16.7 | 21.6 | 99.7 | 74.3 | 216.8 | 7.1 | 342.4 |
Table 2.
Correlations between SD frequency and climate data
|
Frequency Total
|
||
|---|---|---|
| R | p | |
| Monthly minimum temperature (°C) | –0.648 | <0.001 |
| Monthly maximum temperature (°C) | –0.597 | 0.001 |
| Monthly average temperature (°C) | –0.646 | <0.001 |
| Monthly minimum humidity (%) | 0.088 | 0.668 |
| Monthly maximum humidity (%) | –0.609 | 0.001 |
| Monthly average humidity (%) | 0.252 | 0.215 |
| Total hours of sunshine per month | –0.259 | 0.212 |
| Average hours of sunshine per day | –0.257 | 0.214 |
| Monthly max sphering solar radiation, UV index (KW/m2) | –0.442 | 0.027 |
SD: Seborrheic dermatitis; UV: Ultraviolet.
Discussion
This study demonstrated an increase in the frequency of SD during the autumn and winter seasons in Istanbul, Turkey. When assessed with respect to climate data, we found that temperature values and monthly maximum humidity had strong relationships with SD frequency. Interestingly, minimum humidity and average humidity were not correlated with SD frequency, but this is most likely in relation with the fact that limit humidity values were usually consistent throughout the year. These data are in agreement with prior studies indicating that seasonal characteristics can trigger SD, with worsening findings in the winter and milder manifestations in the summer, particularly in the presence of a temperate climate–similar to Istanbul.[6] Our data has indicated negative correlations between SD frequency and both temperature and maximum humidity.
Dermatitis is a frequent condition in temperate countries during harsh winter months due to the disruption of skin barrier function caused by low temperature coupled with low humidity.[8] In addition, Araya et al. have shown that, in warm and moist climates, the summer season may also cause an increase in SD cases due to conditions favoring fungal propagation in the skin (e.g., high humidity).[9] The effects of climate are not limited to temperature and humidity, but also include sunlight exposure. For instance, exposure to sunlight has been demonstrated to suppress Mallassezia species and Langerhans cells, thereby possibly reducing the likelihood of SD.[10] In addition, consistent high humidity throughout the year may also favor the growth of pathogenic bacteria species, especially during the relatively mild autumn season of Istanbul which demonstrates significant variation in temperature from the day to night, possibly leading to a potentiating effect for SD development. This may explain our study’s finding of similar frequency of SD in the winter and autumn in Istanbul.
Today, it is well established that seasonal changes affect the typical structure of the epidermis, which can lead to the triggering of SD,[11,12] and various studies have demonstrated higher frequency of SD in the winter and lower in the summer, similar to our findings.[6,13] When looking at SD frequency distribution by months, it was evident that frequency was highest in December and February which represented 7.3% and 7.1% of all cases, respectively, while the months with the lowest distribution were June (3.8%) and July (3.9%). Three main mechanisms are held responsible for SD pathogenesis: Increased sebaceous gland activity, Malassezia species and host predisposition. It has been speculated that seasonal changes increase sebaceous gland activity; however, there is controversy regarding the direction of these relationships. In a study conducted in Korea, oily skin was more common in the summer, whereas another study in China found that oily skin was more frequent in the autumn.[14,15] Malassezia species, which are lipid-dependent fungi naturally present on the human skin, increase the density of free fatty acids and fatty peroxidase metabolites in the environment through lipase activity, thereby disrupting skin barrier and increasing inflammatory cytokines in the environment which predisposes the skin to SD development.[16,17] Wan et al. have detected a positive correlation between humidity and skin lubrication.[13] In addition, similar to the findings in our study, Kutlu et al. found that high temperature resulted in lower frequency of SD.[18] Considering that Malassezia species propagate at an increased rate in high humidity, it is possible that the inter-relationships between climate characteristics and Malassezia growth may lead to a vicious cycle in environmentally-favoring conditions. Metabolites such as oleic acid, arachidonic acid and indol-3-carbaldehyde lead to skin irritation, keratinocyte proliferation, and inflammation as a result of the lipase activity of Malassezia species.[19] Vijaya Chandra et al. determined that dandruff develops with oleic acid application and Malassezia growth, thereby revealing a direct relationship between Malassezia and the pathogenesis of SD.[20] However, it remains unclear whether different strains of this fungus lead to varying effects in terms of SD development, especially among individuals without any other risk factors.[21] A study conducted in China, which investigated the relationship between biophysical measures of the skin and environmental factors, found that, in addition to moisture, UV radiation and air temperature (average temperature), other factors such as skin pH and transepidermal water loss were effective on seborrheic characteristics.[14] In relation with these findings, a study have shown that changes such as epidermal dysfunction in the host may alter the skin microbiome, lead to the proliferation of Malassezia species,[22] and many studies have assessed the relationships between environmental factors and growth of Malassezia on the skin, with temperature, humidity, and UV light suggested to be significantly influential.[23] Although our study only focused on the correlations between climate characteristics and SD frequency, the results appear to be in support of these hypothesis when the high frequency of SD in the autumn season is considered.
While the findings of the present study are important in showing the frequency of SD and its relationship with climate parameters in Istanbul, the limitations of the research should also be considered. This research is restricted by its retrospective nature, limited sample size with respect to the population of Istanbul, and the fact that the majority of individuals were Caucasian, which are properties that prevent the generalization of the findings. Moreover, no definite statements can be taken regarding causal relationships because of the cross-sectional nature. Despite these limitations, the results of this study highlight the distinct mediating effects of temperature and average humidity in the development of SD in this Turkish population. It is also important to reiterate that the incidence of SD was similar in the winter and autumn seasons, even though the daytime temperatures (maximum temperature) of these two seasons demonstrate a significant difference. Although no data pertaining to fungi growth was obtained in this study, when the temperature and humidity characteristics are evaluated together, it seems reasonable to suggest that the autumn season in Istanbul may be predisposing to Malassezia growth, thereby increasing the frequency of SD to the levels observed in winter.
Conclusion
Our study shows that environmental factors such as low temperature, low UV index, and high humidity are critical factors that increase the likelihood of SD development in a temperate and humid climate. Further research is needed to confirm the impact of climate factors on SD, preferably with the addition of skin analyses of subjects during different seasons and the investigation of Malassezia species in subjects with SD. Ascertaining these data in a single prospectively designed study throughout different centers may provide new perspectives pertaining to the relationship between SD and climatic factors, thereby allowing determination of pathophysiology under different environmental conditions, which could considerably contribute to the management of SD during different seasons.
Disclosures
Ethics Committee Approval: Clinical Studies Ethical Committee of Haseki Training and Research Hospital (No: 200, Date: 04.06.2020).
Peer-review: Externally peer-reviewed.
Conflict of Interest: None declared.
Authorship Contributions: Concept – T.O.A., H.S., T.A.; Design – T.O.A., T.A.; Supervision – T.O.A., T.A.; Materials –T.O.A., H.S.; Data collection &/or processing – T.O.A., H.S., T.A.; Analysis and/or interpretation T.O.A., T.A.; Literature search – T.O.A., H.S.; Writing – T.O.A., T.A.; Critical review – T.O.A., H.S., T.A.
References
- 1.Clark GW, Pope SM, Jaboori KA. Diagnosis and treatment of seborrheic dermatitis. Am Fam Physician. 2015;91:185–90. [PubMed] [Google Scholar]
- 2.Borda LJ, Wikramanayake TC. Seborrheic dermatitis and dandruff: a comprehensive review. J Clin Investig Dermatol. 2015:3. doi: 10.13188/2373-1044.1000019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Berk T, Scheinfeld N. Seborrheic dermatitis. P T. 2010;35:348–52. [PMC free article] [PubMed] [Google Scholar]
- 4.Gupta AK, Bluhm R, Cooper EA, Summerbell RC, Batra R. Seborrheic dermatitis. Dermatol Clin. 2003;21:401–12. doi: 10.1016/s0733-8635(03)00028-7. [DOI] [PubMed] [Google Scholar]
- 5.Dessinioti C, Katsambas A. Seborrheic dermatitis: etiology, risk factors, and treatments: facts and controversies. Clin Dermatol. 2013;31:343–51. doi: 10.1016/j.clindermatol.2013.01.001. [DOI] [PubMed] [Google Scholar]
- 6.Hancox JG, Sheridan SC, Feldman SR, Fleischer AB Jr. Seasonal variation of dermatologic disease in the USA: a study of office visits from 1990 to 1998. Int J Dermatol. 2004;43:6–11. doi: 10.1111/j.1365-4632.2004.01828.x. [DOI] [PubMed] [Google Scholar]
- 7.Balato N, Megna M, Ayala F, Balato A, Napolitano M, Patruno C. Effects of climate changes on skin diseases. Expert Rev Anti Infect Ther. 2014;12:171–81. doi: 10.1586/14787210.2014.875855. [DOI] [PubMed] [Google Scholar]
- 8.Engebretsen KA, Johansen JD, Kezic S, Linneberg A, Thyssen JP. The effect of environmental humidity and temperature on skin barrier function and dermatitis. J Eur Acad Dermatol Venereol. 2016;30:223–49. doi: 10.1111/jdv.13301. [DOI] [PubMed] [Google Scholar]
- 9.Araya M, Kulthanan K, Jiamton S. Clinical characteristics and quality of life of seborrheic dermatitis patients in a tropical country. Indian J Dermatol. 2015;60:519. doi: 10.4103/0019-5154.164410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rubenstein RM, Malerich SA. Malassezia (pityrosporum) folliculitis. J Clin Aesthet Dermatol. 2014;7:37–41. [PMC free article] [PubMed] [Google Scholar]
- 11.Sauer GC. Lippincott; 1973. Manual of skin diseases. [Google Scholar]
- 12.Weiss SC, Rowell R, Krochmal L. Impact of seasonality on conducting clinical studies in dermatology. Clin Dermatol. 2008;26:565–9. doi: 10.1016/j.clindermatol.2008.01.016. [DOI] [PubMed] [Google Scholar]
- 13.Wan MJ, Su XY, Zheng Y, Gong ZJ, Yi JL, Zhao Y, et al. Seasonal variability in the biophysical properties of forehead skin in women in Guangzhou City, China. Int J Dermatol. 2015;54:1319–24. doi: 10.1111/ijd.12741. [DOI] [PubMed] [Google Scholar]
- 14.Youn SW, Na JI, Choi SY, Huh CH, Park KC. Regional and seasonal variations in facial sebum secretions: a proposal for the definition of combination skin type. Skin Res Technol. 2005;11:189–95. doi: 10.1111/j.1600-0846.2005.00119.x. [DOI] [PubMed] [Google Scholar]
- 15.Qiu H, Long X, Ye JC, Hou J, Senee J, Laurent A, et al. Influence of season on some skin properties: winter vs. summer, as experienced by 354 Shanghaiese women of various ages. Int J Cosmet Sci. 2011;33:377–83. doi: 10.1111/j.1468-2494.2011.00639.x. [DOI] [PubMed] [Google Scholar]
- 16.Juntachai W, Oura T, Murayama SY, Kajiwara S. The lipolytic enzymes activities of Malassezia species. Med Mycol. 2009;47:477–84. doi: 10.1080/13693780802314825. [DOI] [PubMed] [Google Scholar]
- 17.Kim GK. Seborrheic dermatitis and malassezia species: how are they related? J Clin Aesthet Dermatol. 2009;2:14–7. [PMC free article] [PubMed] [Google Scholar]
- 18.Kutlu O. JMIR Dermatology Preprints; 2019. Relationship between seborrheic dermatitis and climate change: observational study. [Google Scholar]
- 19.Triana S, de Cock H, Ohm RA, Danies G, Wösten HAB, Restrepo S, et al. Lipid metabolic versatility in Malassezia spp. yeasts studied through metabolic modeling. Front Microbiol. 2017;8:1772. doi: 10.3389/fmicb.2017.01772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Vijaya Chandra SH, Srinivas R, Dawson TL Jr, Common JE. Cutaneous Malassezia: commensal, pathogen, or protector? Front Cell Infect Microbiol. 2021;10:614446. doi: 10.3389/fcimb.2020.614446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hay RJ. Malassezia, dandruff and seborrhoeic dermatitis: an overview. Br J Dermatol. 2011;165(Suppl 2):2–8. doi: 10.1111/j.1365-2133.2011.10570.x. [DOI] [PubMed] [Google Scholar]
- 22.Wikramanayake TC, Borda LJ, Miteva M, Paus R. Seborrheic dermatitis-looking beyond Malassezia. Exp Dermatol. 2019;28:991–1001. doi: 10.1111/exd.14006. [DOI] [PubMed] [Google Scholar]
- 23.Wikler JR, Janssen N, Bruynzeel DP, Nieboer C. The effect of UV-light on pityrosporum yeasts: ultrastructural changes and inhibition of growth. Acta Derm Venereol. 1990;70:69–71. [PubMed] [Google Scholar]