
Figure 1.
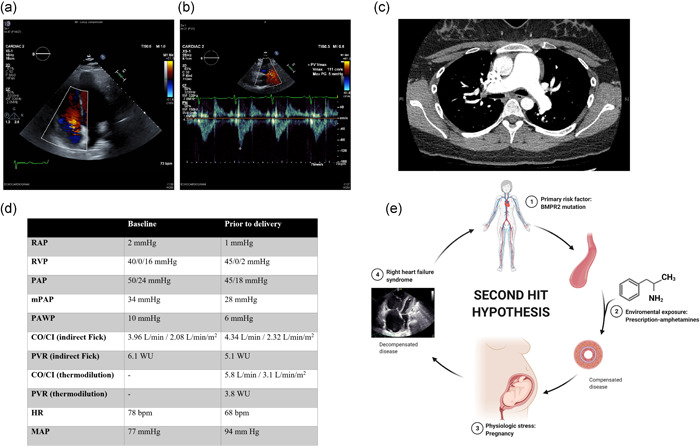
Imaging studies, hemodynamic values, and second hit hypothesis. (a) A two‐dimensional echocardiogram reveals right ventricular dilation and moderate tricuspid regurgitation. (b) Echocardiogram also reveals “notching” of the RVOT tract flow velocity doppler envelope, suggesting increased pulmonary vascular resistance. (c) CT angiogram of the chest reveals enlargement of the pulmonary artery, but no evidence of vascular filling defects. (d) Hemodynamic values at diagnosis (baseline) and after IV treprostinil titration (before delivery). (e) “Second hit” hypothesis. Susceptible individuals for pulmonary vascular disease, such as BMPR2 mutation carriers, could develop pulmonary arterial hypertension if exposed to an additional injury or second hit, such as exposure to amphetamine products like anorexigens or methamphetamines. Pregnancy imposes further physiological stress, with the potential worsening of the disease. We wonder if prescription amphetamines could be considered a second hit in individuals at increased risk. Abbreviations: BMPR2, bone morphogenetic protein receptor type II; CI, cardiac index; CO, cardiac output; CT, computed tomography; HR, heart rate; MAP, mean arterial pressure; mPAP, mean pulmonary arterial pressure; PAP, pulmonary artery pressure; PAWP, pulmonary artery wedge pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure; RVP, right ventricular pressure; RVOT, right ventricular outflow tract. Created with BioRender.com