
Fig. 2.
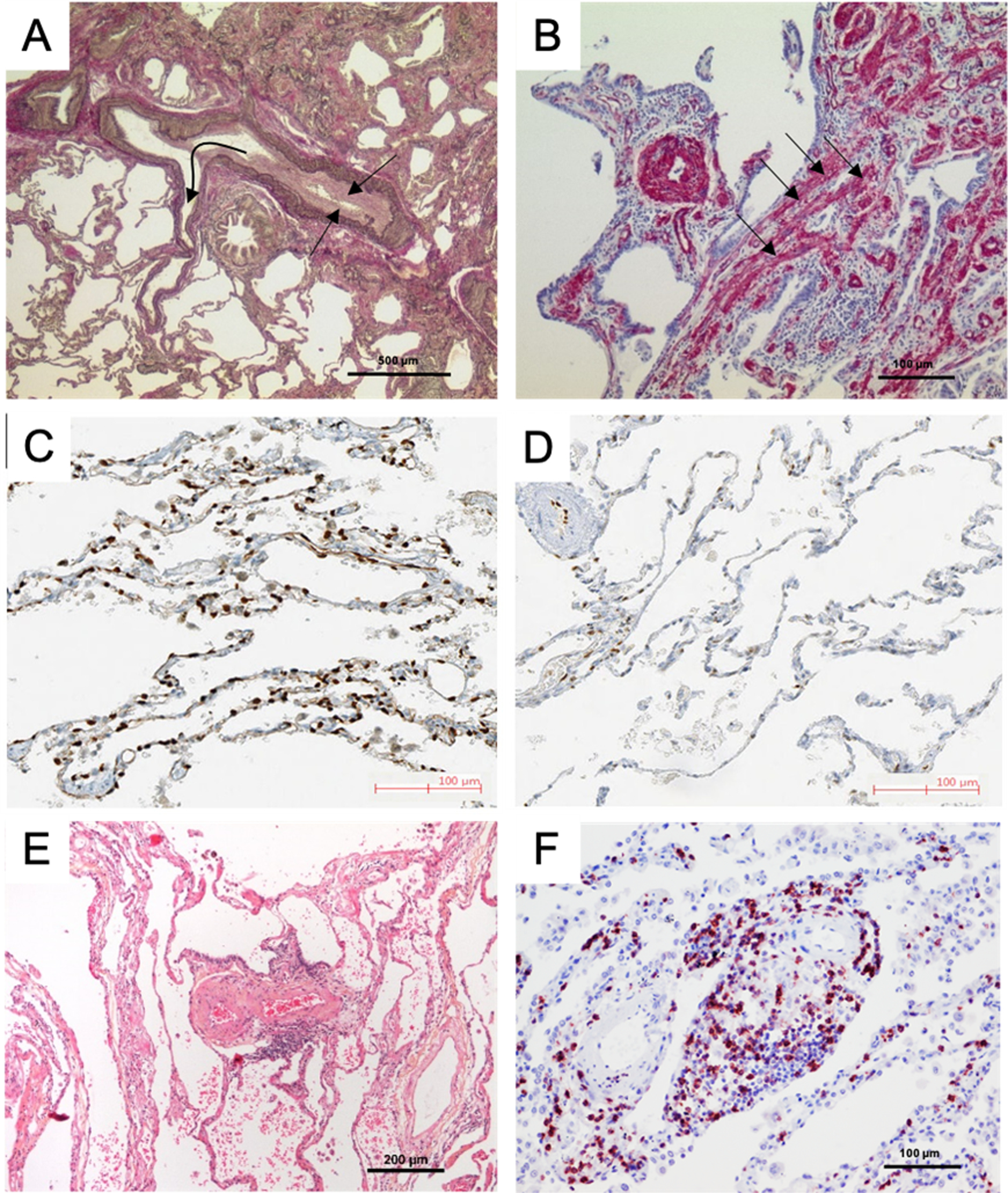
Pulmonary vascular changes in patients with lung disease and Group 3 pulmonary hypertension (PH). A. Pulmonary artery (PA) and its adjacent airway in a patient with idiopathic pulmonary fibrosis (IPF) and PH; note the constrictive intimal fibrosis of the vessel (straight arrows) within the fibrosing area (upper part) and the slender walls of the PA branching out of this area into preserved lung areas (flexuous arrow) with near-normal architecture (lower part). B. Smooth muscle cell hyperplasia within the interstitium (arrows) and within the wall of a small PA, in a patient with IPF-PH; smooth muscle actin-staining. C and D: Capillary density of a patient with chronic obstructive pulmonary disease (COPD) displaying moderate PH (C) and a patient with COPD and severe PH (D): note the loss of ERG-stained endothelial cells within the alveolar septa, corresponding to a decrease of vascular density; photos reprinted with regard to the STM permission guidelines 2022 from Bunel et al. CHEST. 201972. E. PA in a patient with COPD-PH, with severe intimal fibrosis; note the perivascular lymphocytic infiltrate (small blue dots, center). F. Remodeled arterioles in a COPD-PH patient with dense CD5-positive peri-vascular lymphocytic infiltrate (red dots), a feature that can also be observed in pulmonary arterial hypertension.