
Figure 1. Overview of the potential mechanisms through which evidence based treatments influence renal function in HFrEF.
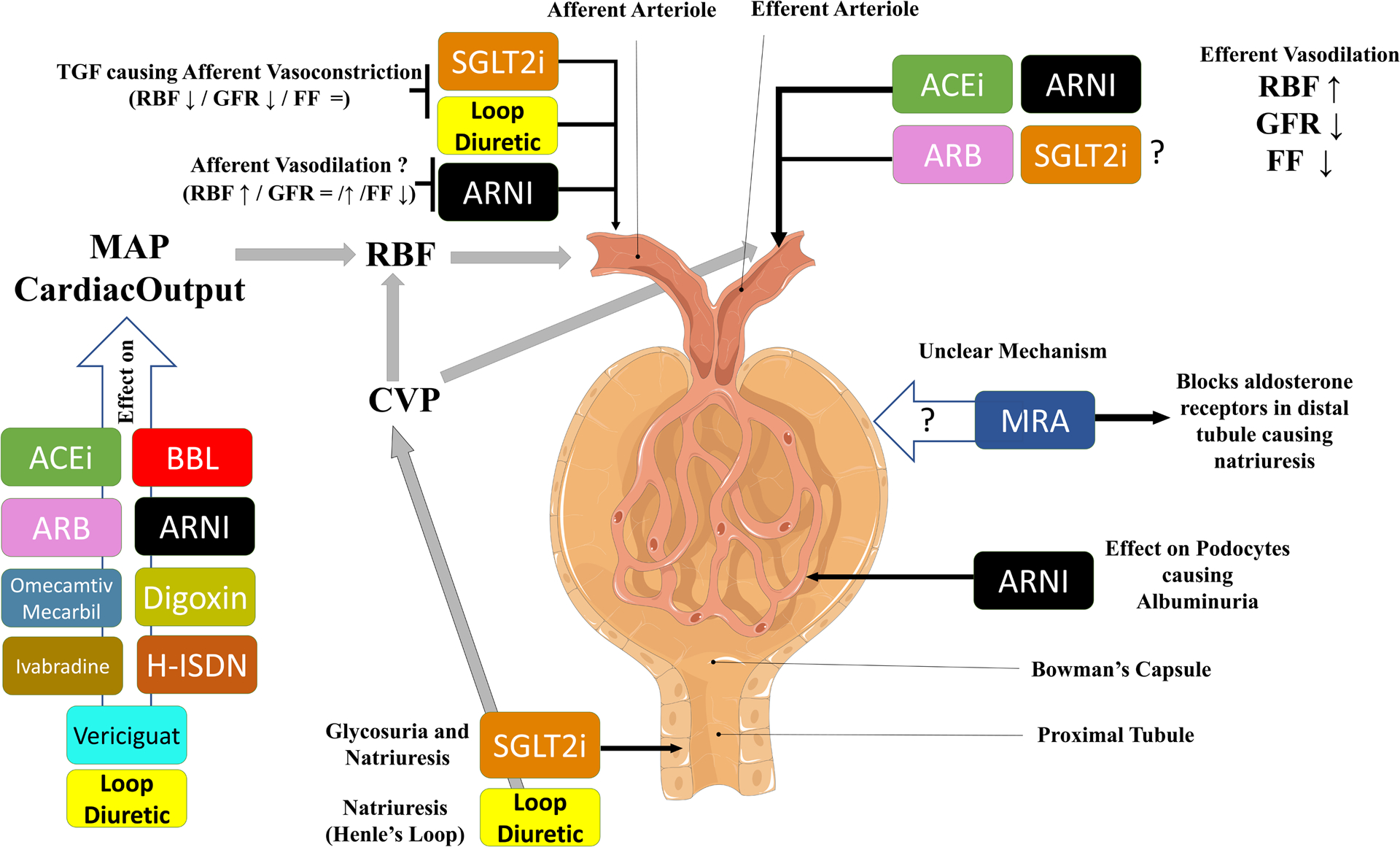
This schematic gives an overview of the potential mechanisms via which evidence based treatments impact renal function in HFrEF. Renin angiotensin system inhibitors (and probably SGLT2i) cause efferent vasodilation, leading to higher RBF, lower GFR and lower FF. It is postulated that SGLT2i have effects on afferent arteriolar tone, causing lower RBF, lower GFR and stable FF. ARNIs may vasodilate the afferent arteriole causing slightly increased RBF and possibly more preserved GFR (as compared with ACEi/ARB alone). ARNIs also influence podocyte function which may be a factor in the modest albuminuria associated with these drugs. It is unclear how MRA influence GFR. Finally, many therapies influence blood pressure, improve contractility and have direct cardiac effects, all of which influence mean arterial pressure and cardiac output/congestion, thereby influencing renal hemodynamics.
Abbreviations: ACEi: Angiotensin Converting Enzyme Inhibitor, ARB: Angiotensin II Receptor Blocker, ARNI: Angiotensin Blocker Neprilysin Inhibitor, BBL: Beta Blocker, CVP, central venous pressure; FF, filtration fraction; GFR, glomerular filtration rate; H-ISDN: Hydralazine-Isosorbidedinitrate, HFrEF, heart failure with reduced ejection fraction; MAP, mean arterial pressure; MRA: Mineralocorticoid Receptor Antagonist, RBF, renal blood flow; SGLT2i: Sodium-glucose co-transporter-2 inhibitor; TGF, tubuloglomerular feedback.