

Abstract
Background
EDTA is an intravenous chelating agent with high affinity to divalent cations (lead, cadmium, and calcium) that may be beneficial in the treatment of cardiovascular disease (CVD). Although a large randomized clinical trial showed benefit, smaller studies were inconsistent. We conducted a systematic review of published studies to examine the effect of repeated EDTA on clinical outcomes in adults with CVD.
Methods and Results
We searched 3 databases (MEDLINE, Embase, and Cochrane) from database inception to October 2021 to identify all studies involving EDTA treatment in patients with CVD. Predetermined outcomes included mortality, disease severity, plasma biomarkers of disease chronicity, and quality of life. Twenty‐four studies (4 randomized clinical trials, 15 prospective before/after studies, and 5 retrospective case series) assessed the use of repeated EDTA chelation treatment in patients with preexistent CVD. Of these, 17 studies (1 randomized clinical trial) found improvement in their respective outcomes following EDTA treatment. The largest improvements were observed in studies with high prevalence of participants with diabetes and/or severe occlusive arterial disease. A meta‐analysis conducted with 4 studies reporting ankle‐brachial index indicated an improvement of 0.08 (95% CI, 0.06–0.09) from baseline.
Conclusions
Overall, 17 studies suggested improved outcomes, 5 reported no statistically significant effect of treatment, and 2 reported no qualitative benefit. Repeated EDTA for CVD treatment may provide more benefit to patients with diabetes and severe peripheral arterial disease. Differences across infusion regimens, including dosage, solution components, and number of infusions, limit comparisons across studies. Additional research is necessary to confirm these findings and to evaluate the potential mediating role of metals.
Registration
URL: https://www.crd.york.ac.uk/; Unique identifier: CRD42020166505.
Keywords: cardiovascular disease, diabetes, EDTA, systematic review
Subject Categories: Treatment, Coronary Artery Disease, Peripheral Vascular Disease, Vascular Disease, Meta Analysis
Nonstandard Abbreviations and Acronyms
- Na2EDTA
disodium EDTA
- PATCH
Program to Assess Treatment Strategies to Achieve Cardiac Health
- TACT
Trial to Assess Chelation Therapy
Clinical Perspective
What Is New?
This systematic review summarizes the literature examining the possible clinical benefits of EDTA chelation therapy in patients with preexistent cardiovascular disease.
This is the largest review to date, including 4 clinical trials, 15 prospective before/after studies, and 5 retrospective case series assessing mortality, disease severity, plasma biomarkers of disease chronicity, and/or quality of life.
We also evaluated the effect of EDTA on metal elimination and whether the clinical effects of EDTA were more pronounced in patients with diabetes and peripheral artery disease.
What Are the Clinical Implications?
There is a signal of benefit for EDTA in patients with atherosclerotic vascular disease.
Patients with diabetes and peripheral artery disease may benefit more from EDTA therapy than other patient populations.
EDTA may eliminate toxic metals associated with atherosclerotic and oxidative vascular damage.
Chelation removes select cations from tissues by forming a chelator‐chelate complex subsequently excreted by the kidneys or liver. 1 EDTA is a synthetic amino acid and polydentate chelator with high affinity for divalent cations, such as lead, cadmium, and calcium. 2 The US Food and Drug Administration has approved its calcium salt (edetate calcium disodium) to treat lead poisoning and, in the past, as an emergent treatment for hypercalcemia. 3 Since 1956, some medical professionals have administered EDTA to treat cardiovascular disease (CVD). 1 Early practitioners proposed decalcification of atherosclerotic plaque as a possible mechanism for EDTA benefit. Although EDTA benefit in atherosclerotic disease is not standard of care, more recent investigations suggest that benefits of chelation may stem from removal of established cardiotoxic metals, such as lead or cadmium. 1 , 4
Initial studies of multiple EDTA infusions to treat CVD showed mixed results. Studies were too small, both individually and in aggregate, to exclude a small to moderate benefit or harm of chelation. 5 , 6 , 7 , 8 , 9 , 10 , 11 In 2013, the TACT (Trial to Assess Chelation Therapy) generated renewed interest on the potential cardiovascular benefits of EDTA‐based chelation. 11 TACT, a National Institutes of Health–funded randomized clinical trial (RCT), examined the effects of 40 infusions of an EDTA‐based mixture in patients with a history of myocardial infarction. The study found a reduction in the primary composite cardiovascular end point, with the greatest benefit among patients with diabetes. 11 , 12 A recent small, open‐label, pilot study of EDTA in patients with diabetes and critical limb‐threatening ischemia showed complete wound healing and improvement in quality of life in those patients completing a 40 infusion regimen. 13 These studies suggest that the potential therapeutic use of EDTA in CVD merits further investigation. Although several reviews are available on metal chelation and CVD, the totality of evidence on the health benefits of EDTA treatment in patients with CVD is still mixed. 1 , 8 , 10 , 14 , 15 To gain clarity on the state of the evidence and perhaps guide future investigations, our team performed a systematic review of published studies reporting clinical outcomes in adults with atherosclerotic CVD treated with EDTA.
METHODS
We reviewed all prior studies up to 2021 that used EDTA as the primary treatment method in patients with existing CVD. Various health outcomes were predetermined, including mortality, disease severity, plasma biomarkers of disease chronicity, and quality of life. Study population characteristics, including diabetes, were also examined to determine if certain high‐risk subpopulations might demonstrate different effect sizes. This study was conducted according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses guidelines. 16 The protocol for this systematic review was registered on PROSPERO (International prospective register of systematic reviews) and can be accessed at https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020166505. 17 The authors declare that all supporting data are available within the article and its online supplemental files.
Search Strategy
A comprehensive search strategy was designed by all authors and executed by R.P. in the MEDLINE, Embase, and Cochrane CENTRAL databases to identify all human studies reporting on chelation therapy with EDTA for patients with CVD published from each database inception through October 27, 2021 (Figure 1). The search query used an exhaustive list of subject headings and keywords. No language or other search limiters were used. Animal studies were excluded using the method recommended in the Cochrane Handbook of Systematic Reviews of Interventions. 18 The full electronic search strategy for all databases is reported in Data S1. In addition, the bibliographies of review articles were hand searched to identify additional eligible studies.
Figure 1. Flow diagram of study selection process.
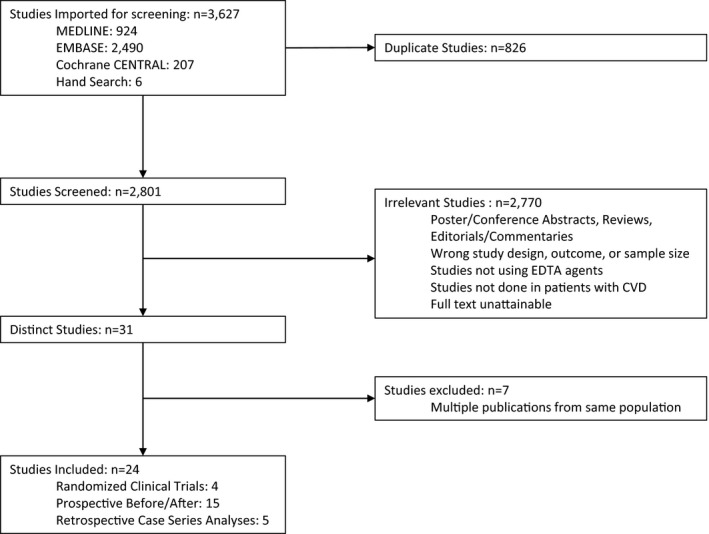
Databases: Cochrane Central (https://www.cochranelibrary.com/central), EMBASE (http://www.embase.com/), and MEDLINE (www.pubmed.gov). CVD indicates cardiovascular disease.
Study Selection and Eligibility Criteria
All studies identified by the electronic searches were imported into the Covidence online review software tool and deduplicated. Results were independently screened by 2 reviewers (X.V.P. and F.R.) in 2 successive rounds, the first on the basis of the title/abstract and the second on the basis of full text. In the case of disagreement between the 2 reviewers, a third author (A.N.‐A.) was consulted.
Studies with the following prespecified patients, intervention, comparison, and outcomes criteria were included: The study population of interest comprised adults with CVD, including coronary disease, cerebrovascular disease, and peripheral artery disease (PAD). Interventions consisted of treatment with chelation therapy with any salt of EDTA and were compared with placebo, standard treatment for CVD, or pre‐post intervention comparison. Outcomes of interest included all‐cause mortality, clinical cardiovascular outcomes, ankle‐brachial index (ABI), vascular structure and function, quality of life, and other outcomes, such as blood pressure, heart rate, and creatinine clearance. Randomized trials, nonrandomized trials, and case series of patients receiving chelation therapy for CVD under controlled (standardized treatment for each patient) or noncontrolled conditions were eligible for inclusion. All outcomes within the inclusion criteria were included, without regard to primary or secondary outcome status in original article. Abstracts, conference posters, and other studies not published in full were excluded. Prospective before/after studies were defined as studies with standardized, comparable treatment regimens and study protocols for all patients. Retrospective case series were defined as retrospective analysis of EDTA treatment outcomes or studies having varied protocols. Studies were subsequently categorized as RCTs, studies with quantitative outcomes (reporting continuous outcomes), or studies with qualitative outcomes (reporting noncontinuous outcomes). One study reporting continuous outcomes in ABI and walking distance was categorized as qualitative because of limitations in study protocol, including changing of placebo intervention to chelation intervention halfway through the study. 19 In addition, a further study reported most of its outcomes as noncontinuous and therefore was categorized as a qualitative study; however, the study also measured quality of life data on a continuous scale. 13
Statistical Analysis
Measures of association and CIs were extracted or derived from the eligible studies. For all studies, except Lamas et al and Green et al, the total mean change was selected as the measure of association for comparison in continuous outcomes. 6 , 9 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 This measure was calculated by taking the difference between the presented outcome values at last reported follow‐up and baseline. For the 4 studies not reporting aggregate findings but reporting results for individual patients, we calculated the mean change by calculating each individual’s mean change and estimating the mean and SD values across all patients. 20 , 21 , 27 , 31 In studies reporting ABI for individual limbs, an average of both limbs was taken if possible 26 , 27 and, if not available, the average of the worse limbs was used. 6 For Lamas et al, the hazard ratio (HR) for time to event outcomes was reported. For Green et al, the resting forearm blood flow after treatment was reported as no baseline data were available.
In studies not reporting CIs or SDs of the mean change, we calculated the missing mean change SD using the correlation coefficients for individual outcomes, as proposed by Higgins et al, 18 which we calculated (range, 0.35–0.87) for studies reporting data for individual patients 27 , 31 or mean change SD 9 and imputed to other studies with the same outcomes. 6 , 24 , 26 , 28 , 32 For studies for which correlation coefficients could not be determined, the median correlation coefficient among all other outcomes (0.67) was used. 6 , 22 , 23 , 25 , 28 , 29 , 33 To determine if 0.67 was influential, we conducted a sensitivity analysis using a correlation coefficient of 0.50, 0.80, 0.90, and 0.95, which showed consistent results. The 95% CIs were subsequently constructed for the mean change±1.96×SE.
A priori, we decided that if at least 3 studies reported similar outcomes and comparison groups, a meta‐analysis would be conducted. Following study extraction, 5 studies with comparable study populations reported mean difference in ABI from baseline following repeated chelation treatment, which met the criteria for inclusion in a meta‐analysis. Of these studies, 1 failed to report variability for ABI outcome, resulting in 4 studies being included in the final analysis. A fixed‐effects meta‐analysis was run solely for descriptive purposes to examine patterns in studies with identical outcomes. The meta‐analysis was conducted using the “meta” package version 5.1‐1 in R version 4.0.2. 34 , 35
Risk of Bias Assessment
For each study fulfilling the inclusion criteria, an assessment of methodological quality was performed by 2 authors (X.V.P. and F.R.). Issues that were unresolved in the assessment were passed to a third reviewer (A.N.‐A.). Discrepancies were discussed until a consensus was reached. For RCTs, the risk of bias was assessed using the Cochrane risk of bias tool for RCTs 2.0. 36 The risk of bias tool assesses different domains for risk of bias, which include the following: the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selective reporting. Risk of bias outcomes are shown in Figure S1. Nonrandomized trials were assessed as “high risk for bias.”
RESULTS
A total of 24 studies, extending from 1957 to 2019, met the inclusion criteria, including 6 studies found by hand search. Of these, 4 RCTs (Table 1), 6 , 9 , 11 , 28 15 prospective before/after studies,* and 5 retrospective case series 4 , 5 , 40 , 41 , 42 were included (Tables 2 and 3). The sample size of the RCTs ranged from 32, in a single‐center study conducted in New Zealand, to 1708, in the TACT, a multicenter clinical trial conducted across the United States and Canada. The sample size of prospective before/after studies ranged from 8 in an Australian study conducted in patients with coronary artery disease (CAD) to 132 in a study conducted in patients with angina pectoris, intermittent claudication, or some form of cerebrovascular disease. The sample size of the retrospective case series studies ranged from 4, in a qualitative study of patients with end‐stage occlusive PAD, to 2870, in a retrospective study of patients at a private clinic in Brazil. Five additional publications reporting different results from the same study population as the initial publication were also summarized in the tables, 3 of them related to the TACT 12 , 32 , 43 and 2 related to other studies. 24 , 29 On the basis of the inclusion criteria, all studies followed up patients with a history of CVD. Ten studies reported the prevalence of diabetes in the study population with an average of 34.2% (range, 0%–100%) across these studies. The number of repeated infusions ranged from 11 to 88 (median, 23).
Table 1.
Randomized Clinical Trials of Chelation Treatment and Health Outcomes in Patients With Prior Cardiovascular Disease
| Author, year | Country | Sample size | Study population | Patient Characteristics | Intervention/comparison | Infusion components | Outcomes | Measure of association | ||
|---|---|---|---|---|---|---|---|---|---|---|
|
Mean age (SD) |
% Female | % Diabetes | ||||||||
| Guldager et al, 1992 28 | Denmark | 159 | Patients 40+ y with stable intermittent claudication ≥ 12 mo, pain free walking distance of 50 to 200 m, and ABI <0.8 in worse leg | 65.0 (9.0) | 35% | 0% |
EDTA vs. saline Number of infusions: ≤20 Vitamin oral supplements: yes |
Intervention: 3 g Na2EDTA, 8.4 g sodium chloride in sterile water diluted to 1000 mL Comparison: 1000 mL isotonic saline |
ABI Chelation Placebo Pain‐free walking distance (m) Chelation Placebo |
Mean (95% CI) Change: +0.06 (0.04 to 0.08) +0.02 (0.0 to 0.04) Mean (95% CI) Change: +23 (13 to 33) +37 (18 to 56) |
| Van Rij et al, 1994 6 | New Zealand | 32 | Patients 45+ y with prior PAD, with no diabetes and no significant renal disease | 67.3 (7.0) | 12% | 0% |
EDTA vs. Saline Number of infusions: ≤20 Vitamin oral supplements: yes |
Intervention: 500 mL infusion consisting of 3 g Na2EDTA, 0.76 g magnesium chloride, 0.84 g sodium bicarbonate, Parentrovite Comparison: 500 mL normal saline, Parentrovite |
ABI Chelation Placebo Pain‐free walking distance (m) Chelation Placebo |
Mean (95% CI) Change: +0.03 (−0.01 to 0.06) −0.03 (−0.06 to 0.00) Mean (95% CI) Change: +12 (−14 to 38) +25 (−13 to 63) |
|
Knudtson et al, 2002 9 (PATCH study) |
Canada | 84 | Patients 21+ y with CAD, prior MI, or stable angina on medical therapy | 65.5 (9.1) | 16% | 15% |
EDTA vs. Non‐chelating infusion Number of Infusions: ≤33 Vitamin oral supplements: yes |
Intervention: 500 mL infusion consisting of 5% dextrose in water, weight adjusted (40 mg/kg, max dose of 3 g) Na2EDTA, 750 mg magnesium sulfate, 5 g ascorbic acid, 5 g sodium bicarbonate Comparison: 500 mL infusion consisting of 5% dextrose in water, 20 mL 0.9% sodium chloride, 750 mg magnesium sulfate, 5 g ascorbic acid, 5 g sodium bicarbonate |
Time to ischemia (s) Chelation Placebo Time to anaerobic threshold (s) Chelation Placebo VO2 Max (mL/min) Chelation Placebo Brachial artery diameter(mm) ‡ Chelation Placebo QOL (DASI) Chelation Placebo SF‐36 Mental Component Chelation Placebo SF‐36 Physical Component Chelation Placebo |
Mean (95% CI) Change: +63 (29 to 95)* +54 (23 to 84)* Mean (95% CI) Change: +31 (−11 to 72) +16 (−27 to 59) Mean (95% CI) Change: +84 (10 to 159) +40 (−53 to 134) Mean (95% CI) Change: +0.00 (−0.26 to 0.26) +0.00 (−0.21 to 0.21) Mean (95% CI) Change: −0.2 (−3.2 to 2.7) 1.9 (−0.6 to 4.5) Mean (95% CI) Change: 2.1 (−0.4 to 4.6) 2.1 (−0.4 to 4.5) Mean (95% CI) Change: 2.2 (−0.5 to 4.9) 5.0 (2.7 to 7.3) |
|
Lamas et al, 2013 11 (TACT Study) |
USA, Canada | 1708 | Patients 50+ y with MI 6 wk or more prior to enrollment | Median: 65 (IQR, 59 to 72) | 18% | 31% |
EDTA (with/without high dose oral vitamin‐minerals) vs. non‐chelating solution (with/without oral vitamin‐mineral) 2×2 trial Number of infusions: ≤40 Vitamin oral supplements: yes |
Intervention: 500 mL infusion consisting of up to 3 g Na2EDTA (adjusted downward based on estimated glomerular filtration rate, 7 g ascorbic acid, 2 g magnesium chloride, 100 mg procaine hydrochloride, 2500 U unfractionated heparin, 2 mEq potassium chloride, 840 mg sodium bicarbonate, 250 mg pantothenic acid, 100 mg thiamine, 100 mg pyridoxine, sterile water) Comparison: 500 mL normal saline, 2.5 g 1.2% dextrose |
Primary composite endpoint † Myocardial infarction Stroke Coronary revascularization Hospitalization for angina Primary composite endpoint † For Patients with Diabetes (Escolar et al, 2014) Primary composite endpoint † For patients with diabetes & PAD (Ujueta et al, 2019) QOL DASI (Mark et al, 2014) Chelation Placebo |
Hazard ratio (95% CI): 0.82 (0.69 to 0.99)* 0.77 (0.54 to 1.11) 0.77 (0.34 to 1.76) 0.81 (0.64 to 1.02) 0.72 (0.35 to 1.47) 0.59 (0.44 to 0.79)* 0.52 (0.30 to 0.92)* Mean (95% CI) Change: +2.5 (1.4 to 3.6) +1.6 (0.6 to 2.6) |
ABI indicates Ankle‐Brachial Index; CAD, coronary artery disease; CI, confidence interval; DASI, Duke Activity Status Index; EDTA, ethylenediaminetetraacetic acid; IQR, interquartile range; MI, myocardial infarction; Na2EDTA, disodium ethylenediaminetetraacetic acid; PAD, peripheral artery disease; QOL, quality of life; SD, standard deviation; SF‐36, Short‐Form 36 Survey; and VO2 Max, maximum oxygen consumption.
P<0.05.
Endpoint is composite of total mortality, recurrent MI, stroke, coronary revascularization, or hospitalization from angina.
Anderson et al (2003). 29
Table 2.
Studies With Quantitative Outcomes of Chelation Therapy and Health Outcomes in Patients With Prior Cardiovascular Disease
|
Author, year Study type |
Country | Sample size | Study population | Patient Characteristics | Intervention/comparison | Infusion components | Outcomes | Measure of association | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean age (SD) | % Female | % Diabetes | ||||||||
|
Casdorph, 1981 20 Prospective before/after |
USA | 15 | Patients had various diagnoses including: 1 patient with Schizophrenia, 1 patient with Alzheimer’s Disease and cerebral atrophy, 3 patients with cerebral atrophy, 10 patients with cardiovascular disease and/or cerebrovascular accident | 68.4 (10.6) | NR | 7% |
EDTA Number of infusions: ≤20 Vitamin oral supplements: yes |
Intervention: 3 g Na2EDTA in 250 mL or 500 mL of Ringer’s lactate solution | Cerebral B Wave Elevation (measure of brain blood flow curve) |
Mean (95% CI) Change: +2.28 (1.76 to 2.79)* |
|
Casdorph, 1981 21 Prospective before/after |
USA | 18 | Patients with CAD heart disease | 60.3 (9.1) | 56% | NR |
EDTA Number of infusions: ≤20 Vitamin oral supplements: yes |
Intervention: 3 g Na2EDTA in 250 mL of Ringer’s lactate solution |
Left ventricle ejection fraction (%) |
Mean (95% CI) Change: +5.77 (3.39 to 8.15)* |
|
McDonagh et al, 1983 22 Prospective before/after |
USA | 80 | Patients with chronic degenerative disorders, primarily occlusive arterial disease | 63.8 (9.2) | 43% | NR |
EDTA Number of infusions: ≤30 Vitamin oral supplements: yes |
Intervention: 3 g Na2EDTA in 1000 mL of carrier solutions |
Blood urea nitrogen (mg/dL) |
Mean (95% CI) Change: −1.07 (−2.22 to 0.08)* |
|
Cheraskin et al, 1984 23 Prospective before/after |
USA | 50 | Patients with history of cardiac problems or considered cardiac‐prone based on family history, elevated BP, and/or obesity | 60.1 (9.3) | NR | NR |
EDTA only vs EDTA+exercise Mean (SD) Number of infusions: 32.9 (12.6) Vitamin oral supplements: yes |
Intervention: NR |
Heart Rate After Stage I Bruce Test (beats per minute) EDTA only EDTA+exercise SBP After Stage I Bruce Test † (mm Hg) EDTA only EDTA+exercise |
Mean (95% CI) Change: −6.0 (−10.45 to −1.5)* −8.5 (−13.74 to −3.3)* −13.4 (−21.3 to −5.6)* −13.2 (−21.9 to −4.5)* |
|
Sehnert et al, 1984 25 Prospective before/after |
USA | 13 | Patients with CAD, arteriosclerosis and with poor creatinine clearance | NR | NR | NR |
EDTA Number of infusions: ≤20 Vitamin oral supplements: yes |
Intervention: NR |
Creatinine clearance (mL/min per 1.73 cm) |
Mean (95% CI) Change: |
|
McDonagh et al, 1985 26 Prospective before/after |
USA | 77 | Patients with vascular stenosis | 63.4 (9.9) | 47% | NR |
EDTA Mean (SD) Number of infusions: 26.2 (8.1) Vitamin oral supplements: yes |
Intervention: 3 g EDTA |
ABI |
Mean (95% CI) Change: +0.17 (0.13 to 0.21)* |
|
Godfrey, 1990 27 Prospective before/after |
New Zealand | 27 | Patients with PAD in one or both legs with intermittent claudication, pain and/or coldness in feet | 68.6 (8.8) | 41% | NR |
EDTA Number of infusions: ≤23 Vitamin oral supplements: NR |
Intervention: NR |
ABI |
Mean (95% CI) Change: +0.17 (0.12 to 0.21) |
|
Green et al, 1999 39 Prospective before/after |
Australia | 8 | Patients with CAD and presented to general physician for chelation therapy | 59.0 (3.0) | 38% | 0% |
EDTA vs EDTA+vitamins vs saline Number of infusions: ≤11 § Vitamin oral supplements: NR |
EDTA only: 1.5 g Na2EDTA in 500 mL physiological saline EDTA + Vitamins: 1.5 g Na2EDTA, 20 mEq magnesium, 100 mg nicotinamide, 20 mg decapantothenol, 10 mg thiamine, 5 mg riboflavin, 50 mg pyridoxine, 1 mg cyanocobalamin in 500 mL physiological saline Saline: 500 mL physiological saline |
Absolute resting forearm blood flow post treatment (mL/100 mL forearm per min) EDTA EDTA+vitamins Saline only |
Mean (SEM) 2.70 (0.37) 2.54 (0.33) 2.76 (0.35) |
|
Öckerman, 2011 30 Prospective before/after |
Sweden | 82 | Patients ≤85 y and nonsmokers with MI, angina, stroke, or PAD | Range 50 to 81 | 66% | NR |
EDTA Number of infusions: ≤30 Vitamin oral supplements: yes |
Intervention: 1.5 g Na2EDTA, with corresponding amount of magnesium and bicarbonate in 250 mL 5% glucose |
Brachial artery stiffness index ‖ Pulse wave velocity ‖ (m/s) Pulse wave velocity biological age ‖ (y) Augmentation index ‖ (AIX) Erythrocyte fragility test |
Mean Change: −104.6* −1.5* −21.3* −12.65* −11.3* (negative value reflects benefit) |
|
Born et al, 2013 31 Prospective before/after |
USA | 33 | Patients with CVD | 67.6 (8.6) | 36% | NR |
EDTA Number of infusions: ≤20 Vitamin oral supplements: NR |
Intervention: 250 mL solution consisting of 1.5 g Na2EDTA, 1.2 g magnesium chloride, 0.5 g vitamin C, smaller quantiles of pyridoxine, dexpanthenol, B‐complex, sodium bicarbonate, potassium chloride, procaine, sterile water |
SBP (mm Hg) DBP (mm Hg) |
Mean (95% CI) Change: −14.61 (−2.79 to −8.42) −2.58 (−5.51 to 0.36) |
|
Lin et al, 2017 33 Prospective before/after |
Taiwan | 30 | Patients with CAD | 64.9 (6.1) | 3% | NR |
EDTA Number of infusions: >25 Vitamin oral supplements: Yes |
Intervention: 500 mL 5% dextrose in water, 1 g CaNa2EDTA, 750 mg magnesium sulfate, 5 g ascorbic acid, 5 g sodium bicarbonate |
Blood urea nitrogen (mg/dL) Serum creatinine (mg/dL) Brachial diameter (mm) Baseline peak blood flow (mL/s) |
Mean (95% CI) Change: +0.40 (−1.58 to 2.38) −0.02 (−0.23 to 0.19) +0.11 (−0.05 to 0.27) +0.31 (−2.17 to 2.79) |
ABI indicates Ankle‐Brachial Index; BP, blood pressure; CAD, coronary artery disease; CaNa2EDTA, calcium disodium ethylenediaminetetraacetic acid; CI, confidence interval; CVD, cardiovascular disease; DBP, diastolic blood pressure; EDTA, ethylenediaminetetraacetic acid; MI, myocardial infarction; Na2EDTA, disodium ethylenediaminetetraacetic acid; NR, not reported; PAD, peripheral artery disease; SBP, systolic blood pressure; SD, standard deviation; and SEM, standard error of means.
Reported as statistically significant.
McDonagh et al (1984). 24
Baseline mean (SD): 62.5 (14.8) mL/min per 1.73 cm.
Each subject underwent each treatment arm. Number of infusions is number per treatment arm.
Subset of total sample size used in analysis.
Table 3.
Studies With Qualitative Outcomes of Chelation Therapy and Health Outcomes of in Patients With Prior Cardiovascular Disease
|
Author, year Study type |
Country | Sample size | Study population | Patient characteristics | Comparison/intervention | Infusion components | Main findings | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) Age | % Female | % Diabetes | |||||||
|
Boyle et al, 1957 40 Retrospective case series |
USA | 7 | All patients had angina pectoris, 2 patients also had coronary occlusion and 1 patient had prior MI | 55.2 (4.6) | 0% | NR |
EDTA Number of Infusions: ≤40 Vitamin oral supplements: NR |
Intervention: 5 g Na2EDTA in 500 mL of glucose | All patients indicated relief of angina symptoms and had improvement in exercise ability through increased pain‐free walking distance. Patients remained symptom‐free after long‐term follow‐up (3+ mo) |
|
Clarke et al, 1960 37 Prospective before/after |
USA | 132 | 76 patients with angina pectoris, 31 patients with intermittent claudication, and 25 patients with some form of cerebrovascular disease | 66.0 | NR | NR |
EDTA Number of infusions: ≤30 Vitamin oral supplements: NR |
Intervention: 3 g Na2EDTA in 500 mL of 5% glucose or normal saline |
87% of patients with angina pectoris were symptomatically improved and 2‐y mortality was 13.0%. Symptom recurrence after 2 y was reported as 20% Patients with intermittent claudication showed improvement with relief from rest pain and improved pain‐free walking distances. Amputations occurred in 2 patients and 4 patients had pain recurrence after 22 mo. 5‐y mortality was reported as 10% Patients with cerebrovascular disease and had severe vertigo or dizziness showed large improvements and patients with senility showed improved mental faculties EDTA was also found to reduce serum cholesterol levels and levels remained lower after end of treatment |
|
Kitchell et al, 1963 38 Prospective Before/After |
USA |
38 |
Patients with severe angina due to CAD | NR | NR | NR |
EDTA Number of infusions: ≤20 Vitamin oral supplements: NR |
Intervention: 3–4 g Na2EDTA in 500 mL of glucose or normal saline | 15 patients showed clinical improvement of angina symptoms, including improvement in EKG, exercise ability, and reduced nitroglycerine use, while 12 patients died to original disease at time of reporting (18–48 mo post treatment). Clinical improvements were only noted 6–8 wk post‐treatment and only a limited number of patients had lasting effects |
|
Lamar, 1964 5 Retrospective case series |
USA | 7 | Patients with diabetes and/or occlusive arterial disease (CAD and PAD) | 61.4 (8.1) | 43% | 100% |
EDTA Number of infusions: ≤88 Vitamin oral supplements: yes |
Intervention: 3 g Na2EDTA, 500 mL normal saline or 5% dextrose solution | Patients had improved brain function (improved speech, reduced amnesia, improved coordination, fewer depressive episodes), lowering of BP (systolic/diastolic), ulcer healing, reduction in insulin dependence, and vision improvement from diabetic retinopathy. Three patients died post treatment, but postmortem examinations in two patients indicted the normal appearance of the islands of Langerhans despite severe diabetes prognosis before EDTA treatment. Severe calcification in vessels may have been unimproved, resulting in death |
|
Migliau et al, 1964 41 Retrospective case series |
Italy | 7 | Patients had prior dyspnea, edema in extremities of inferior arteries, hypertension, diabetes, and all patients had complete AV block on EKG | 57.4 (18.8) | NR | 14% |
EDTA Number of infusions: ≤12 Vitamin oral supplements: NR |
Intervention: 3 g Na2EDTA in 500 mL physiological saline | 4 patients with complete AV block showed improvement in EKG and restoration of normal sinus rhythm. 3 patients showed no improvement following treatment |
|
Casdorph & Farr, 1983 4 Retrospective case series |
USA | 4 | Patients with end‐stage occlusive PAD and referred for surgical amputation of limbs | 67.0 (7.9) | 0% | 75% |
EDTA Number of infusions: ≤45 Vitamin oral supplements: NR |
Intervention: 1.5–3 g EDTA in 500 mL of Ringer’s lactate or 2.5–5% glucose in saline | EDTA reversed natural cause of disease with healing of ulcers and gangrene avoiding complete amputation. 1 patient underwent amputation of second, third, and fourth toes of affected foot but showed complete absence of necrosis and ischemia at 1 mo follow‐up. All patients were free of pain and able to walk without limitations |
|
Olszewer & Carter, 1988 42 Retrospective case series |
Brazil | 2870 | Patients with PAD, CAD, cerebrovascular and degenerative CNS disease, scleroderma, or other geriatric vascular disease | NR | 54% | NR |
EDTA Number of infusions: ≤40 Vitamin oral supplements: yes |
Intervention: 50 mg EDTA per kg of body weight, vitamin C, vitamin B complex, magnesium | 91% of PAD subgroup had “marked improvement”. † 77% of CAD patients showed “marked improvement”. ‡ 24% of cerebrovascular disease subgroup showed “marked improvement” § |
|
Olszewer et al, 1990 19 Prospective before/after |
Brazil | 10 | Patients with PAD (intermittent claudication but no at rest pain or gangrene) due to diabetes or arteriosclerosis | 47 (range: 41–53) | 0% | NR |
EDTA Number of infusions: ≤20 Vitamin oral supplements: NR |
Intervention: 10 mL infusion consisting of 1.5 g Na2EDTA, 2 g vitamin C, 2 mL B complex, 500 IU heparin, 1 g magnesium sulfate Comparison: 10 infusions of placebo consisting of distilled water, 1 g magnesium sulfate, 2 mL B complex, 2 g vitamin C in Ringer’s lactate followed by 10 infusions of intervention solution |
EDTA treatment showed significant improvement in both ABI and walking distance. Placebo subgroup was switched to EDTA treatment following 10 infusions to significant improvement seen in treatment subgroup. After initial 10 infusions, treatment group walking distance improved by 2.65 times baseline distance, compared to 1.1 times baseline distance in placebo group. ABI at rest improved by 0.23 after 10 infusions, compared to 0.01 in placebo group. After final infusion, walking distance in original treatment group was three times the baseline distance, compared to two times the baseline distance in placebo group. ABI at rest improved on average by 0.29 for treatment group after final infusion, compared to 0.24 in placebo group (No SD provided) |
|
Arenas et al, 2019 13 Prospective before/after |
USA | 10 | Patients 50+ y with a diagnosis of moderate or severe PAD (infra‐popliteal chronic critical limb ischemia) | 75.3 (8.3) | 40% | 100% |
EDTA Number of infusions: ≤50 Vitamin oral supplements: yes |
Intervention: 500 mL infusion consisting of up to 3 g Na2EDTA (adjusted downward based on estimated glomerular filtration rate, 7 g ascorbic acid, 2 g magnesium chloride, 100 mg procaine hydrochloride, 2500 U unfractionated heparin, 2 mEq potassium chloride, 840 mg sodium bicarbonate, 250 mg pantothenic acid, 100 mg thiamine, 100 mg pyridoxine) | No amputations in 7 patients that completed over 20 infusions. In 5 of 7 patients who completed all 40 infusions ulcers and dry gangrene completely resolved with no new active wound infections during infusion phase. Amputation occurred in 3 subjects who failed to complete full infusion regimen |
ABI indicates Ankle‐Brachial Index; AV, atrioventricular; BP, blood pressure; CAD, coronary artery disease; CNS, central nervous system; EDTA, ethylenediaminetetraacetic acid; EKG, electrocardiogram; MI, myocardial infarction; Na2EDTA, disodium ethylenediaminetetraacetic acid; NR, not reported; PAD, peripheral artery disease; and SD, standard deviation.
Retrospective analysis of treatment results of patients with chronic degenerative and age‐associated diseases treated with EDTA chelation between May 1983 and September 1985 at private clinic in Sao Paulo, Brazil.
Peripheral group: Marked improvement defined as: patient could walk 5× distance at baseline and not develop intermittent claudication, and had normal clinical appearance of lower extremities and normal doppler ultrasound.
Coronary heart disease group: Marked improvement defined as: Patient with previous positive stress test that become negative and who was previously symptomatic and became asymptomatic and off all drugs, following EDTA treatment.
No improvement criteria reported for cerebrovascular disease subgroup.
Overall, 17 suggested improved outcomes,† 5 reported no statistically significant effect of EDTA treatment, 6 , 9 , 28 , 33 , 39 and 2 reported no qualitative benefit. 38 , 41 Of the 10 studies reporting prevalence of diabetes, all 4 studies with prevalence of ≥25% suggested improved outcomes. Seventeen studies used disodium EDTA (Na2EDTA) as the chelating agent,‡ 1 used calcium Na2EDTA, 33 and 6 did not specify the EDTA salt used. 4 , 23 , 25 , 26 , 27 , 42 A total of 11 of 17 of the studies using Na2EDTA indicated improved outcomes. The dose for the chelating agent ranged from 1 to 5 g. All RCTs used up to 3 g of Na2EDTA as the chelating agent, and 2 of 4 RCTs used a normal saline solution as the placebo. 6 , 28
Three studies analyzed urinary metal levels at baseline and posttreatment for lead. In 2 studies, lead was measured pretreatment and during follow‐up. Both studies indicated significant decreases in urinary lead from baseline to last point of follow‐up, with mean decreases of 8.40 μg/L (SD, 4.29 μg/L) (74.40% decrease) 33 and 9.76 μg/g creatinine (SD, 13.48 μg/g creatinine) (58.04% decrease). 31 In addition, one study also reported significant decrease in urinary cadmium following treatment, with a mean decrease of 0.34 μg/L (SD, 0.39 μg/L) (22.67% decrease). 33 A third study measured urinary lead and cadmium immediately pretreatment and posttreatment at baseline and after the final infusion. After the first infusion, both urinary lead and cadmium significantly increased by 22.4 μg/g creatinine (SD, 15.17 μg/g creatinine) and 3.0 μg/g creatinine (SD, 1.59 μg/g creatinine), respectively. The corresponding increases following the last infusion were 7.2 μg/g creatinine (SD, 5.69 μg/g creatinine) for lead and 3.4 μg/g creatinine (SD, 1.94 μg/g creatinine) for cadmium. 13
Mortality and Clinical CVD Outcomes
The TACT reported a significant reduction in the primary composite end point in the active treatment arm compared with placebo (HR, 0.82; 95% CI, 0.69–0.99) (Table 1). 11 There was no statistically significant hazard reduction for total mortality (HR, 0.93; 95% CI, 0.70–1.25), but this study was not powered to measure this effect. The HRs for the primary composite end point were markedly stronger in the subset of patients (n=633) with diabetes (HR, 0.59; 95% CI, 0.44–0.79) 12 and in patients (n=162) with both diabetes and PAD (HR, 0.52; 95% CI, 0.30–0.92). 43 A case study examining mortality following EDTA treatment found a 2‐year cumulative mortality of 13% in patients with angina pectoris, compared with a cumulative mortality of 23.6% in a comparison group receiving medical treatment without EDTA. 37 Two case studies included data on mortality (31.58% cumulative mortality 38 and 42.86% cumulative mortality) 5 but lacked any comparison group. No other study reported all‐cause mortality data.
Studies in Patients With PAD
Eleven studies (3 RCTs) 6 , 11 , 28 reported on patients with PAD or related outcomes, including ABI and pain‐free walking distance (Table 4). Two RCTs conducted in patients experiencing intermittent claudication 28 and in patients with PAD 6 excluded all patients with diabetes at recruitment and found no significant difference in both ABI and pain‐free walking distance comparing repeated EDTA treatment versus placebo. Two prospective before/after studies conducted in patients with vascular stenosis and patients with arteriosclerosis in one or both legs found improvements in ABI following EDTA treatment (Table 2). 26 , 27 These studies did not report diabetes prevalence.
Table 4.
Detailed Outcomes in Studies Reporting Ankle/Brachial Index & Walking Distance
| Study name | ||||||
|---|---|---|---|---|---|---|
| Godfrey (1990) 27 | Guldager et al (1992) 28 , * | McDonagh et al (1985) 26 | Van Rij et al (1994) 6 | |||
| Chelation | Chelation | Placebo | Chelation | Chelation | Placebo | |
| ABI | ||||||
| Baseline | 0.71 (0.27) | 0.50 (0.15) | 0.51 (0.13) | 0.77 (0.22) | 0.59 (0.13) | 0.61 (0.11) |
| Post treatment | 0.88 (0.33) | 0.52 (0.14) | 0.52 (0.14) | 0.94 (0.27) | 0.70 (0.36) | 0.60 (0.15) |
| 3‐mo follow up | NR | 0.54 (0.14) | 0.53 (0.14) | NR | 0.62 (0.15) | 0.58 (0.13) |
| 6‐mo follow up | NR | 0.56 (0.13) | 0.53 (0.14) | NR | NR | NR |
| Pain‐free walking distance (m) | ||||||
| Baseline | NR | 74 (25) | 82 (36) | NR | 92 (64) | 98 (67) |
| Post treatment | NR | 93 (41) | 109 (56) | NR | 101 (50) | 121 (89) |
| 3‐mo follow up | NR | 95 (48) | 102 (42) | NR | 104 (62) | 123 (108) |
| 6‐mo follow up | NR | 97 (47) | 119 (93) | NR | NR | NR |
Results are reported as: value (SD). ABI indicates Ankle‐Brachial Index; and NR, not reported.
Number of subjects changed at each follow‐up.
Six studies reported qualitative results in patients with PAD through retrospective case series analysis or prospective before/after studies of patients receiving repeated EDTA infusions (Table 3). 4 , 5 , 13 , 19 , 37 , 42 A qualitative study of patients with diabetes and PAD or retinopathy reported ulcer healing, vision improvement, and reductions in insulin dependence in patients. 5 A qualitative study conducted in patients with intermittent claudication indicated that patients had relief from rest pain and improved pain‐free walking distance. 37 Two qualitative retrospective case series studies in patients with moderate to severe PAD (diabetes prevalence, 75% 4 and 100% 13 ) reported that repeated EDTA reversed the natural cause of PAD in patients with end‐stage occlusive PAD through complete healing of ulcers and gangrene, avoiding limb amputation in most cases. 4 , 13 A double‐blind prospective case series study indicated that patients with PAD treated with EDTA had significantly improved ABI and walking distance compared with placebo, resulting in the authors to switch the placebo group to receive treatment infusions following half of the infusion regimen. 19 A retrospective analysis in a single practitioner chelation practice in Brazil, of patients with chronic vascular and nonspecific “degenerative diseases,” such as cardiac disease, PAD, and other geriatric vascular diseases, treated with EDTA indicated that 91% of patients with PAD had a “marked improvement” (patient could walk 5× distance at baseline with no intermittent claudication, and had normal clinical appearance of lower extremities and normal Doppler ultrasound). 42 A descriptive meta‐analysis of ABI outcomes in active treatment arm across 4 studies with comparable data 6 , 26 , 27 , 28 showed a mean difference of 0.08 (95% CI, 0.06–0.09) of the ABI at follow‐up compared with baseline (Figure 2).
Figure 2. Meta‐analysis for studies reporting ankle‐brachial index (ABI) outcome.
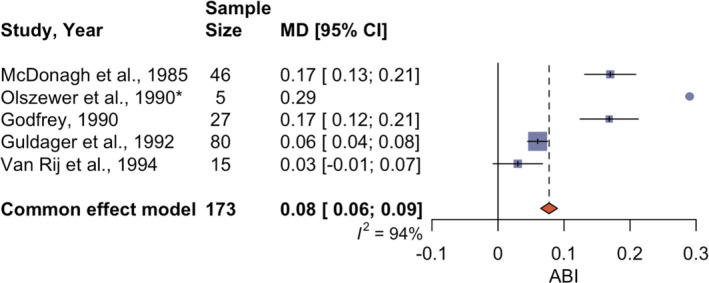
All studies measured the ABI at baseline and at the end of repeated chelation treatment with EDTA infusions. One study (*) did not report the SD or any other measure that would allow to estimate the SD and was not included in the meta‐analysis. In Guldager et al 28 and Van Rij et al 6 , only the active treatment arm was included in the analysis. A fixed‐effects meta‐analysis to estimate the common effect in ABI comparing follow‐up with baseline was conducted using the “meta” package version 5.1‐1 in R version 4.0.2. 34 , 35 Because of differences in the compared studies, this meta‐analysis was done for descriptive purposes only, and no clear conclusions should be drawn from it. Square indicates size of weight; tick mark/circle, effect size; black horizontal line, CI; red diamond, common effect estimate and CI; and dashed vertical line, common effect estimate. MD indicates mean difference.
Brachial Artery Diameter and Blood Flow
Five studies reported outcomes associated with changes in vascular structure and function, including pulse wave velocity, left ventricular ejection fraction, and brachial artery diameter. One RCT, the multicenter PATCH (Program to Assess Treatment Strategies to Achieve Cardiac Health) study conducted in Alberta, Canada (n=84; diabetes prevalence, 15%), found no differences between chelation and placebo for any measured outcome, including time to ischemia, time to anaerobic threshold, and maximal oxygen consumption (Table 1). 9 The PATCH study did not report clinical outcomes. A study examining change in absolute resting forearm blood flow in patients with CAD found no significant differences between EDTA and saline in resting forearm blood flow. 39 Another prospective before/after study conducted in patients with CAD also found no significant differences in baseline peak blood flow from pretreatment level. 33 Two studies measured brachial artery diameter after chelation treatment and found no significant difference in diameter between baseline and follow‐up (Table 5). 29 , 33 A subset of the PATCH study also found no difference in brachial artery diameter between chelation or placebo treatment. 29 Of the studies that found no improvement following repeated EDTA treatment, only 2 reported prevalence of diabetes and both had ≤15% patients with diabetes. 9 , 39 One prospective before/after study in patients with CAD saw significant improvements in left ventricular ejection fraction. 21 Another before/after study conducted in Sweden, examining arterial stiffness, found a significant decrease in brachial artery stiffness, pulse wave velocity, augmentation index, and erythrocyte fragility following repeated EDTA treatment compared with baseline. 30 These 2 studies did not report diabetes prevalence.
Table 5.
Detailed Outcomes in Studies Reporting Brachial Artery Diameter
| Study name | |||
|---|---|---|---|
| Anderson et al (2003) 29 , * | Lin et al (2017) 33 | ||
| Chelation | Placebo | Chelation | |
| Brachial artery diameter, mm | |||
| Baseline | 4.0 (0.8) | 4.1 (0.7) | 3.45 (0.55) |
| 3‐mo follow up | NR | NR | 3.37 (0.57) |
| 6‐mo follow up | 4.0 (0.8) | 4.1 (0.5) | 3.56 (0.54) |
Results are reported as: value (SD).
PATCH Study.
Quality of Life
Three studies evaluated quality of life with the 36‐Item Short Form Health Survey and/or the Duke Activity Status Index (Table 6). 9 , 13 , 32 The PATCH study RCT (n=84; diabetes prevalence, 15%) reported only small increases in both 36‐Item Short Form Health Survey and Duke Activity Status Index scores, with no difference between placebo and chelation groups for either metric. 9 In a randomly selected subset of the TACT (n=911; diabetes prevalence, 33%), a slight improvement for the EDTA group was noted in the Duke Activity Status Index score without reaching statistical significance; however, the baseline score of TACT was lower than the PATCH study in both conditions. 32 Both TACT and PATCH study found no significant difference in quality of life scores between chelation and placebo groups. An open‐label pilot study conducted in 10 patients with moderate‐to‐severe PAD (n=10; diabetes prevalence, 100%) found a significant improvement in the 36‐Item Short Form Health Survey scores, including gains of 30 and 35 points, from a baseline of 45, in the physical and mental score medians, respectively. 13
Table 6.
Detailed Outcomes in Studies Reporting Quality of Life
| Study name | |||||
|---|---|---|---|---|---|
| Mark et al (2014) 32 , * | Knudtson et al (2002) 9 , † | Arenas et al (2019) 13 | |||
| Chelation | Placebo | Chelation | Placebo | Chelation (median, IQR) | |
| DASI | |||||
| Baseline | 24.6 (17.8) | 23.5 (17.5) | 42.2 (12.5) | 37.4 (13.4) | NR |
| 6‐mo follow up | 29.1 (17.4) | 27.0 (18.0) | 41.9 (14.2) | 39. 3 (14.5) | NR |
| 12‐mo follow up | 29.4 (17.1) | 26.3 (18.1) | NR | NR | NR |
| SF‐36 Physical Score | |||||
| Baseline | NR | NR | 42.9 (10.1) | 39.9 (11) | 45 (28.8–60) |
| Post‐treatment | NR | NR | NR | NR | 75 (57–80) |
| 6‐mo follow up | NR | NR | 45.1 (10.0) | 44.9 (10.7) | NR |
| SF‐36 Mental Score | |||||
| Baseline | NR | NR | 52.6 (7.6) | 48.3 (10.4) | 45 (32.5–88) |
| Post‐treatment | NR | NR | NR | NR | 80 (55–93.5) |
| 6‐mo follow up | NR | NR | 54.6 (6.7) | 50.4 (9.2) | NR |
Results are reported as: value (SD) unless noted otherwise. DASI indicates Duke Activity Status Index; IQR, interquartile range; NR, not reported; and SF‐36, Short‐Form 36.
TACT Study.
PATCH Study.
Other Outcomes
Additional quantitative prospective before/after studies reported significant improvements following EDTA treatment in different outcomes, including decreased heart rate and systolic blood pressure 23 , 31 (Table 2). In 3 studies of patients with angina pectoris, 2 reported lasting symptom improvement and increased exercise ability, 37 , 40 whereas the third indicated that treatment provided only temporary symptom improvement in some patients. 38 In a study of 7 patients with complete atrioventricular block, 4 of them showed restoration of normal sinus rhythm following treatment, whereas 3 patients showed no improvements (Table 3). 41
DISCUSSION
Summary
The overview of the heterogenous data available in high‐risk patients with CVD suggests a signal of benefit for repeated infusions of EDTA chelation, especially in patients with diabetes or severe PAD. Given EDTA’s known role as an effective chelator of 2 atherogenic divalent toxic cations, lead and cadmium, there is a possible, cautiously interpreted, mechanistic‐based inference of a causal relationship. However, limitations in the available studies, including the small number of RCTs, the lack of reported clinical outcomes in many studies, differing infusion regimens, limited sample sizes, and limited follow‐up data, make accurate estimation of the true effect size of repeated EDTA in patients with CVD difficult to calculate. Confounding variables may also have biased possible improvements indicated in some studies. In addition, studies conducted in private chelation clinics may introduce surveillance and even financial bias in reporting outcomes, potentially making results unreliable. 42
Only 1 RCT, the TACT, was sufficiently large and followed up participants long enough to have clinical outcomes as the primary end point. TACT showed reduced hazard in its primary composite cardiovascular end point for EDTA therapy compared with placebo, with a particularly strong effect size in patients with diabetes. In reports with comparable intermediate outcomes (Tables 2, 3, 4), no consistent improvement was observed across studies. A meta‐analysis conducted in 4 studies reporting ABI suggested a small but significant increase in ABI (Figure 2); however, our analysis was for descriptive purposes only, and no clear conclusions should be drawn because of the differences in studies. Mortality data were reported in the TACT and some case series. Case series, however, lacked a comparison group, impeding the evaluation of the effect of EDTA on overall mortality. Moreover, only a few studies reported diabetes prevalence and stratified analyses by diabetes status. Diabetes may be a relevant subgroup for benefit.
EDTA Mechanism and Regimen
EDTA targets divalent cations, such as metal ions, in plasma, soft tissues, and potentially bone and removes them from circulation following renal excretion. 1 EDTA binds metal ions with differing affinity because of differences in the binding constants of EDTA for different metals, with lead and zinc excreted in a greater amount than cadmium and calcium. 44 We identified 3 studies in this review that showed a decline in urine lead and cadmium levels following treatment with EDTA, although statistical significance was only tested and confirmed in 2 studies. 13 , 31 , 33 Furthermore, one study conducting urine sample collection immediately following the infusion showed a major relative increase in lead (3600% increase) and cadmium (566% increase) levels, suggesting that EDTA can facilitate renal excretion of metals. 13 An additional study (n=14), not included in this review as it did not include any health outcome, also found significant decrease in lead urine levels in patients with coronary artery disease comparing postedetate level after first and final infusions, with no significant differences found for cadmium. 45 In the treatment of CVD, EDTA has been suggested to lower vessel calcification through calcium removal and reduction in metal burden, although these hypotheses have not been confirmed. Because of its high affinity for calcium, EDTA may cause symptomatic hypocalcemia, and therefore lengthy infusion periods (3–4 hours) are used. 46 In the TACT, no difference in allergic reactions, renal function, or heart failure exacerbations was observed between the treatment and placebo groups. Furthermore, only 1 of >27 000 EDTA infusions resulted in symptomatic hypocalcemia requiring an emergency department visit. 11 , 46
EDTA chelation for the treatment of CVD generally follows a multidose regimen of intravenous infusions in combination with oral multivitamins and minerals. 10 Given the prolonged timespan during which the extracted studies were conducted, numerous EDTA infusion regimens were used. Each infusion regimen used different minerals, EDTA salt, and EDTA dosage, resulting in a potential source of confounding for comparison between studies. Most studies (n=17) reported using Na2EDTA as the chelating agent, with only one study using calcium Na2EDTA. Similarly, dosage varied across studies, as some reported using a fixed EDTA dose for all patients, whereas others adjusted chelating agent dose based on body weight or glomerular filtration rate. No clear pattern emerged between EDTA dosage and patient improvement. Choice of minerals and amount of water present in the infusion may also have had a confounding effect. In studies examining renal function, a high amount of saline in the solution may have helped improve dehydrated patients, rather than EDTA chelation. Two studies that reported improved renal function did not indicate the solution components, but the improvement may have been related to the volume of crystalloid infused. 22 , 25 Although creatinine clearance improvement has not been observed during the TACT or subsequent studies, one previous study reported improved renal function following repeated EDTA chelation therapy. 47 Future research will be necessary to understand the role of chelation on renal function.
The 4 RCTs all used up to 3 g of Na2EDTA as the chelating agent and dose. The remaining nutrients in the infusion, however, varied greatly. For instance, the TACT used 10 different components in the treatment infusion, including 7 g of ascorbic acid, whereas Guldager et al used only EDTA, sodium chloride, and water. Differences in the infusion components add a significant source of confounding. Similarly, the placebo solution for each RCT differed, with 2 studies using normal saline as the comparison, whereas the remaining RCTs used nonchelating infusion of glucose in saline. 9 , 11 Consequently, accurate comparison between studies is difficult and further research is necessary to confirm the effect of infusion components and EDTA dosage.
Effect of EDTA on Patients With Vascular Disease and Diabetes
Our analyses suggest that EDTA chelation may be particularly beneficial for patients with diabetes and CVD. Among the studies that reported diabetes prevalence, those with ≥25% patients with diabetes reported improvements in their respective outcomes. 4 , 5 , 11 , 13 As an example, the TACT reported the largest effect size on the primary end point of combined cardiovascular events (HR, 0.59; P=0.0002) in patients with diabetes (Figure 3). 12 TACT also suggested, in a nonprespecified analysis, that post–myocardial infarction patients with PAD as well as underlying diabetes improved significantly (HR, 0.52; P=0.0069). 43 Other studies in patients with end‐stage PAD also found significant improvement, including the resolution of lower extremity gangrene and ulcers, increased pain‐free walking ability, improvement in quality of life, and the avoidance of lower extremity amputations (Figure 4). 4 , 13 , 48 Many of the studies with end‐stage PAD also included patients with diabetes. In 2 of the reported RCTs, patients with diabetes were excluded, and these studies found no significant improvement in their respective outcomes. 6 , 28 It is possible that the exclusion of patients with diabetes might explain the lack of improvement from EDTA chelation in those studies.
Figure 3. Kaplan‐Meier estimates of primary composite end point in patients with diabetes (n=633) (A) and without diabetes (n=1075) (B) following EDTA treatment in the TACT (Trial to Assess Chelation Therapy).
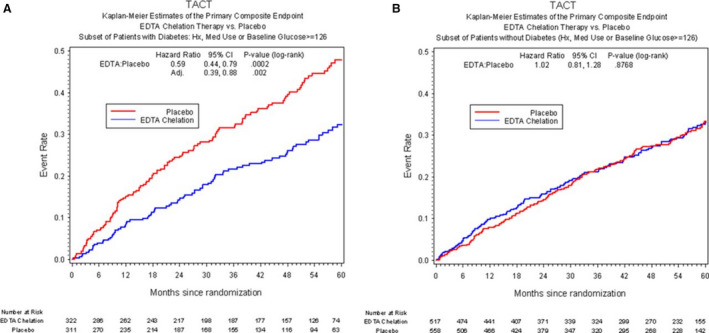
Adapted with permission from Escolar et al. 12 ©2013, Wolters Kluwer Health, Inc. Med indicates medication.
Figure 4. Evolution of gangrene wound appearance at baseline (top) and following final EDTA infusion treatment (bottom). 48 .

Possible Role of EDTA in the Emerging Field of Environmental Cardiology
Numerous studies have linked metal exposure to CVD development. 49 , 50 , 51 On entering the body, heavy metals, including lead and cadmium, affect multiple cellular and molecular mechanisms and result in downstream vascular changes. For example, elevated lead levels may cause a reduction in antioxidant effects, such as reduced glutathione activity, paraoxonase inactivation, and impaired calcium signaling, resulting in decreased ability of the cell to clear reactive oxygen species and free radicals as well as elevated expression of inflammatory markers. 46 , 52 , 53 , 54 Similarly, cadmium has also been associated with reduced glutathione activity, cadmium‐induced cell death through apoptotic pathway activation, and DNA methylation, resulting in increased oxidative stress, inflammation, and endothelial cell death. 46 , 55 , 56 , 57 Increased oxidative stress and endothelial dysfunction have been previously associated with CVD. 49 , 52 , 58 , 59 , 60 Epidemiological studies examining the role of heavy metals have also found that low‐level metal exposure is associated with adverse cardiovascular effects. 46 , 50 , 61 , 62 , 63 , 64 , 65 EDTA chelation of heavy metals may therefore benefit patients with CVD through antioxidant effects by reducing toxic metal burden. Only 3 of the extracted studies measured metal levels following chelation. 13 , 31 , 33 These 3 studies found decreases in lead levels, with 2 of the studies also reporting patient improvement following EDTA chelation. 13 , 31
In patients with diabetes, metal exposure can facilitate the worsening of vascular function. Numerous metals, including lead, cadmium, and arsenic, have been associated with a higher risk of diabetes onset because of their contribution to oxidative stress. 49 , 66 , 67 , 68 The added benefit for patients with diabetes identified in this systematic review may stem from metal catalyzed oxygen chemistry promoting the formation of advanced glycation end products. Advanced glycation end products are oxidized, cross‐linked glucose molecules that interact with endothelial cells, contributing to increased inflammatory cytokine expression. 1 , 46 , 49 , 68 These effects can subsequently contribute to subclinical changes, such as atherogenesis and hypertension, leading to clinical CVD effects. 49 It is possible that EDTA reduces toxic metal burden and formation of oxidation products, thus improving patient outcomes more significantly among patients with diabetes. 1 , 67 , 68 All of these hypotheses, however, must be taken cautiously, as they have not been demonstrated in patients.
Although recent evidence for the benefit of EDTA treatment has been mixed, few studies have evaluated differences in diabetes prevalence as a source of heterogeneity. One recent meta‐analysis found no evidence of a difference between EDTA chelation and placebo for CVD treatment; however, only one study had a diabetes prevalence of >30%. 15 It is possible that the review failed to fully capture the patient population who stands to benefit most significantly from chelation treatment.
EDTA chelation therapy for stable ischemic heart disease was classified as a IIB treatment with level B evidence in the 2014 American College of Cardiology/American Heart Association/American Association for Thoracic Surgery/Preventative Cardiovascular Nurses Association/Society for Cardiovascular Angiography and Interventions/Society of Thoracic Surgeons Focused Update of the Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, suggesting that although treatment may outweigh risk, further investigation is necessary to recommend routine use. 69 Currently, to the best of our knowledge, at least 2 ongoing studies are examining EDTA treatment in post–myocardial infarction patients with diabetes (TACT2) and patients with chronic limb‐threatening ischemia and diabetes (TACT3a). Furthermore, evidence on EDTA treatment cost remains limited. A preliminary cost analysis in 7 patients with critical limb ischemia found EDTA therapy to significantly lower cost of treatment compared with the average cost of standard treatment for critical limb ischemia, although the study failed to include the cost of EDTA infusions, which are variable by community. 70 Cost‐benefit analyses have also been planned as part of the TACT2.
Interest in EDTA chelation as treatment for CAD, especially in patients with diabetes, has grown because of the results of the TACT. This present systematic review of past studies suggests a signal of benefit in patients with atherosclerotic disease, particularly in those with diabetes. In vitro and epidemiologic evidence suggests that reduction of toxic metal burden may be causal for clinical benefit, a hypothesis that fits well with the emerging field of environmental cardiology. Future clinical research on EDTA chelation on patients with diabetes and PAD must include a mechanistic component, as is being done with the ongoing 1000‐patient National Institutes of Health–sponsored TACT2, which may help clarify if chelation therapy truly represents a significant benefit for this population subgroup, contributing to precision environmental medicine.
Sources of Funding
Dr Navas‐Acien and F. Ravalli were supported in part by the following National Institutes of Health grants: P42ES010349, P30ES009089, and R01ES028758.
Disclosures
None.
Supporting information
Data S1
Figure S1
Acknowledgments
We would like to thank the Columbia University Mailman School of Public Health and the Icahn School of Medicine at Mount Sinai for providing access to databases and the abstract screening tool Covidence.
Supplemental Material is available at https://www.ahajournals.org/doi/suppl/10.1161/JAHA.121.024648
For Sources of Funding and Disclosures, see page 21.
Footnotes
Contributor Information
Filippo Ravalli, Email: fr2420@cumc.columbia.edu.
Ana Navas‐Acien, Email: an2737@cumc.columbia.edu.
References
- 1. Lamas GA, Navas‐Acien A, Mark DB, Lee KL. Heavy metals, cardiovascular disease, and the unexpected benefits of edetate disodium chelation therapy. J Am Coll Cardiol. 2016;67:2411–2418. doi: 10.1016/j.jacc.2016.02.066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Lamas GA, Hussein SJ. EDTA chelation therapy meets evidence‐based medicine. Complement Ther Clin Pract. 2006;12:213–215. doi: 10.1016/j.ctcp.2006.04.002 [DOI] [PubMed] [Google Scholar]
- 3. Wax PM. Current use of chelation in American health care. J Med Toxicol. 2013;9:303–307. doi: 10.1007/s13181-013-0347-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Casdorph HR, Farr CH. EDTA chelation therapy III: treatment of peripheral arterial occlusion, an alternative to amputation. J Holist Med. 1983;5:3–15. [Google Scholar]
- 5. Lamar CP. Chelation therapy of occlusive arteriosclerosis in diabetic patients. Angiology. 1964;15:379–395. doi: 10.1177/000331976401500902 [DOI] [PubMed] [Google Scholar]
- 6. van Rij AM, Solomon C, Packer SG, Hopkins WG. Chelation therapy for intermittent claudication: a double‐blind, randomized, controlled trial. Circulation. 1994;90:1194–1199. doi: 10.1161/01.CIR.90.3.1194 [DOI] [PubMed] [Google Scholar]
- 7. Ernst E. Chelation therapy for peripheral arterial occlusive disease. Circulation. 1997;96:1031–1033. doi: 10.1161/01.CIR.96.3.1031 [DOI] [PubMed] [Google Scholar]
- 8. Ernst E. Chelation therapy for coronary heart disease: an overview of all clinical investigations. Am Heart J. 2000;140:139–141. doi: 10.1067/mhj.2000.107548 [DOI] [PubMed] [Google Scholar]
- 9. Knudtson ML, Wyse DG, Galbraith PD, Brant R, Hildebrand K, Paterson D, Richardson D, Burkart C, Burgess E; Program to Assess Alternative Treatment Strategies to Achieve Cardiac Health (PATCH) Investigators . Chelation therapy for ischemic heart disease: a randomized controlled trial. JAMA. 2002;287:481–486. doi: 10.1001/jama.287.4.481 [DOI] [PubMed] [Google Scholar]
- 10. Seely DMR, Wu P, Mills EJ. EDTA chelation therapy for cardiovascular disease: a systematic review. BMC Cardiovasc Disord. 2005;5:32. doi: 10.1186/1471-2261-5-32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Lamas GA, Goertz C, Boineau R, Mark DB, Rozema T, Nahin RL, Lindblad L, Lewis EF, Drisko J, Lee KL, et al. Effect of disodium EDTA chelation regimen on cardiovascular events in patients with previous myocardial infarction: the TACT randomized trial. JAMA. 2013;309:1241–1250. doi: 10.1001/jama.2013.2107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Escolar E, Lamas GA, Mark DB, Boineau R, Goertz C, Rosenberg Y, Nahin RL, Ouyang P, Rozema T, Magaziner A, et al. The effect of an EDTA‐based chelation regimen on patients with diabetes and prior myocardial infarction in TACT. Circ Cardiovasc Qual Outcomes. 2014;7:15–24. doi: 10.1161/CIRCOUTCOMES.113.000663 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Arenas I, Ujueta F, Diaz D, Yates T, Olivieri B, Beasley R, Lamas G. Limb preservation using edetate disodium‐based chelation in patients with diabetes and critical limb ischemia: an open‐label pilot study. Cureus. 2019;11:e6477. doi: 10.7759/cureus.6477 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Chappell LT, Janson M. EDTA chelation therapy in the treatment of vascular disease. J Cardiovasc Nurs. 1996;10:78–86. doi: 10.1097/00005082-199604000-00008 [DOI] [PubMed] [Google Scholar]
- 15. Villarruz‐Sulit MV, Forster R, Dans AL, Tan FN, Sulit DV. Chelation therapy for atherosclerotic cardiovascular disease. Cochrane Database Syst Rev. 2020;5:Cd002785. doi: 10.1002/14651858.CD002785.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group . Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. Ann Intern Med. 2009;151:264–269, W264. doi: 10.7326/0003-4819-151-4-200908180-00135 [DOI] [PubMed] [Google Scholar]
- 17. Ravalli F, Navas‐Acien A, Ujueta F, Vela Parada XF. Chelation therapy in patients with cardiovascular disease: a systematic review. PROSPERO: International prospective register of systematic reviews. 2020. CRD42020166505. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020166505. Accessed April 28, 2020.
- 18. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane; 2021. [Google Scholar]
- 19. Olszewer E, Sabbag FC, Carter JP. A pilot double‐blind study of sodium‐magnesium EDTA in peripheral vascular disease. J Natl Med Assoc. 1990;82:173–177. [PMC free article] [PubMed] [Google Scholar]
- 20. Casdorph HR. EDTA chelation therapy II, efficacy in brain disorders. J Holist Med. 1981;3:101–117. [Google Scholar]
- 21. Casdorph HR. EDTA chelation therapy, efficacy in arteriosclerotic heart disease. J Holist Med. 1981;3:53–59. [Google Scholar]
- 22. McDonagh EW, Rudolph CJ, Chearaskin E. The effect of EDTA chelation therapy plus supportive multivitamin‐trace mineral supplementation upon renal function: a study in blood urea nitrogen (BUN). J Holist Med. 1983;5:163–171. [Google Scholar]
- 23. Cheraskin E, Wussow DG, McDonagh EW, Rudolph CJ. Effect of EDTA chelation and supportive multivitamin/trace mineral supplementation with and without physical activity on the heart rate. J Int Acad Prev Med. 1984;8:5–9. [Google Scholar]
- 24. McDonagh EW, Rudolph CJ, Cheraskin E, Wussow DG. Effect of EDTA chelation and supportive multivitamin/trace mineral supplementation with and without physical activity upon systolic blood pressure. J Orthomol Psychiatry. 1984;13:1–9. [Google Scholar]
- 25. Sehnert KW, Clague AF, Cheraskin E. The improvement in renal function following EDTA chelation and multi‐vitamin‐trace mineral therapy: a study in creatinine clearance. Med Hypotheses. 1984;15:301–304. doi: 10.1016/0306-9877(84)90020-3 [DOI] [PubMed] [Google Scholar]
- 26. McDonagh EW, Rudolph CJ, Chearaskin E. Effect of EDTA chelation therapy plus multivitamin trace mineral supplementation upon vascular dynamics: ankle/brachial Doppler systolic blood pressure ratio. J Holist Med. 1985;7:16–22. [Google Scholar]
- 27. Godfrey ME. EDTA chelation as a treatment of arteriosclerosis. N Z Med J. 1990;103:162–163. [PubMed] [Google Scholar]
- 28. Guldager B, Jelnes R, Jørgensen SJ, Nielsen JS, Klaerke A, Mogensen K, Larsen KE, Reimer E, Holm J, Ottesen S. EDTA treatment of intermittent claudication—a double‐blind, placebo‐controlled study. J Intern Med. 1992;231:261–267. doi: 10.1111/j.1365-2796.1992.tb00533.x [DOI] [PubMed] [Google Scholar]
- 29. Anderson TJ, Hubacek J, Wyse DG, Knudtson ML. Effect of chelation therapy on endothelial function in patients with coronary artery disease: PATCH substudy. J Am Coll Cardiol. 2003;41:420–425. doi: 10.1016/S0735-1097(02)02770-5 [DOI] [PubMed] [Google Scholar]
- 30. Öckerman PA. Improvement of arterial stiffness by EDTA‐chelation in combination with vitamin, mineral, trace element and antioxidant supplements. J Orthomol Med. 2011;26:5. doi: 10.1016/j.amjhyper.2006.09.021 [DOI] [Google Scholar]
- 31. Born T, Kontoghiorghe CN, Spyrou A, Kolnagou A, Kontoghiorghes GJ. EDTA chelation reappraisal following new clinical trials and regular use in millions of patients: review of preliminary findings and risk/benefit assessment. Toxicol Mech Methods. 2013;23:11–17. doi: 10.3109/15376516.2012.730562 [DOI] [PubMed] [Google Scholar]
- 32. Mark DB, Anstrom KJ, Clapp‐Channing NE, Knight JD, Boineau R, Goertz C, Rozema TC, Liu DM, Nahin RL, Rosenberg Y, et al. Quality of life outcomes with a disodium EDTA chelation regimen for coronary disease: results from the TACT randomized trial. Circ Cardiovasc Qual Outcomes. 2014;7:508–516. doi: 10.1161/CIRCOUTCOMES.114.000977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Lin S‐L, Liu T‐Y, Hung Y‐M, Huang W‐C, Wu M‐L, Chen J‐W, Kuo H‐W. Effects of antioxidant and chelation therapy in coronary artery disease patients with elevated lead or cadmium levels. Int J Clin Exp Med. 2017;10:11123–11132. [Google Scholar]
- 34. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta‐analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22:153–160. doi: 10.1136/ebmental-2019-300117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. R Core Team . R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; 2021. https://www.R‐project.org/. Accessed January 13, 2022. [Google Scholar]
- 36. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng H‐Y, Corbett MS, Eldridge SM, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi: 10.1136/bmj.l4898 [DOI] [PubMed] [Google Scholar]
- 37. Clarke NE, Mosher RE. Treatment of occlusive vascular disease with disodium ethylene diamine tetraacetic acid (EDTA). J Med Sci. 1960;239:732–744. [DOI] [PubMed] [Google Scholar]
- 38. Kitchell JR, Palmon F, Aytan N, Meltzer LE. The treatment of coronary artery disease with disodium EDTA: a reappraisal. Am J Cardiol. 1963;11:501–506. doi: 10.1016/0002-9149(63)90011-0 [DOI] [PubMed] [Google Scholar]
- 39. Green DJ, O’Driscoll JG, Maiorana A, Scrimgeour NB, Weerasooriya R, Taylor RR. Effects of chelation with EDTA and vitamin B therapy on nitric oxide‐related endothelial vasodilator function. Clin Exp Pharmacol Physiol. 1999;26:853–856. doi: 10.1046/j.1440-1681.1999.03156.x [DOI] [PubMed] [Google Scholar]
- 40. Boyle AJ, Jasper JJ, McCormick H, Kosai M, McCann D, Goodwin J, Clarke NE, Mosher RE. Studies in human and induced atherosclerosis employing ethylenediaminetetraacetic acid. Bull Schweiz Akad Med Wiss. 1957;13:408–425. [PubMed] [Google Scholar]
- 41. Migliau G, Liotta S, Rengo F. Ethylene diamineotetraacetic acid in complete atrioventricular dissociation. Prog Med (Napoli). 1964;20:491–501. [PubMed] [Google Scholar]
- 42. Olszewer E, Carter JP. EDTA chelation therapy in chronic degenerative disease. Med Hypotheses. 1988;27:41–49. doi: 10.1016/0306-9877(88)90082-5 [DOI] [PubMed] [Google Scholar]
- 43. Ujueta F, Arenas IA, Escolar E, Diaz D, Boineau R, Mark DB, Golden P, Lindblad L, Kim H, Lee KL, et al. The effect of EDTA‐based chelation on patients with diabetes and peripheral artery disease in the Trial to Assess Chelation Therapy (TACT). J Diabetes Complications. 2019;33:490–494. doi: 10.1016/j.jdiacomp.2019.04.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Waters RS, Bryden NA, Patterson KY, Veillon C, Anderson RA. EDTA chelation effects on urinary losses of cadmium, calcium, chromium, cobalt, copper, lead, magnesium, and zinc. Biol Trace Elem Res. 2001;83:207–221. doi: 10.1385/BTER:83:3:207 [DOI] [PubMed] [Google Scholar]
- 45. Alam ZH, Ujueta F, Arenas IA, Nigra AE, Navas‐Acien A, Lamas GA. Urinary metal levels after repeated edetate disodium infusions: preliminary findings. Int J Environ Res Public Health. 2020;17:4684. doi: 10.3390/ijerph17134684 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Ujueta F, Navas‐Acien A, Mann KK, Prashad R, Lamas GA. Low‐level metal contamination and chelation in cardiovascular disease—a ripe area for toxicology research. Toxicol Sci. 2021;181:135–147. doi: 10.1093/toxsci/kfab026 [DOI] [PubMed] [Google Scholar]
- 47. Lin J‐L, Lin‐Tan D‐T, Hsu K‐H, Yu C‐C. Environmental lead exposure and progression of chronic renal diseases in patients without diabetes. N Engl J Med. 2003;348:277–286. doi: 10.1056/NEJMoa021672 [DOI] [PubMed] [Google Scholar]
- 48. Ujueta F, Arenas IA, Yates T, Beasley R, Diaz D, Lamas GA. Edetate disodium‐based treatment in a patient with diabetes and critical limb ischemia after unsuccessful peripheral arterial revascularizations: a case report. Clin Diabetes. 2019;37:294–297. doi: 10.2337/cd18-0059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Cosselman KE, Navas‐Acien A, Kaufman JD. Environmental factors in cardiovascular disease. Nat Rev Cardiol. 2015;12:627–642. doi: 10.1038/nrcardio.2015.152 [DOI] [PubMed] [Google Scholar]
- 50. Chowdhury R, Ramond A, O’Keeffe LM, Shahzad S, Kunutsor SK, Muka T, Gregson J, Willeit P, Warnakula S, Khan H, et al. Environmental toxic metal contaminants and risk of cardiovascular disease: systematic review and meta‐analysis. BMJ. 2018;362:k3310. doi: 10.1136/bmj.k3310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Alissa EM, Ferns GA. Heavy metal poisoning and cardiovascular disease. J Toxicol. 2011;2011:870125. doi: 10.1155/2011/870125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Farah C, Michel LYM, Balligand J‐L. Nitric oxide signalling in cardiovascular health and disease. Nat Rev Cardiol. 2018;15:292–316. doi: 10.1038/nrcardio.2017.224 [DOI] [PubMed] [Google Scholar]
- 53. Mangge H, Becker K, Fuchs D, Gostner JM. Antioxidants, inflammation and cardiovascular disease. World J Cardiol. 2014;6:462–477. doi: 10.4330/wjc.v6.i6.462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Solenkova NV, Newman JD, Berger JS, Thurston G, Hochman JS, Lamas GA. Metal pollutants and cardiovascular disease: mechanisms and consequences of exposure. Am Heart J. 2014;168:812–822. doi: 10.1016/j.ahj.2014.07.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Lamas GA, Ujueta F, Navas‐Acien A. Lead and cadmium as cardiovascular risk factors: the burden of proof has been met. J Am Heart Assoc. 2021;10:e018692. doi: 10.1161/JAHA.120.018692 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Biagioli M, Pifferi S, Ragghianti M, Bucci S, Rizzuto R, Pinton P. Endoplasmic reticulum stress and alteration in calcium homeostasis are involved in cadmium‐induced apoptosis. Cell Calcium. 2008;43:184–195. doi: 10.1016/j.ceca.2007.05.003 [DOI] [PubMed] [Google Scholar]
- 57. Domingo‐Relloso A, Riffo‐Campos AL, Haack K, Rentero‐Garrido P, Ladd‐Acosta C, Fallin DM, Tang WY, Herreros‐Martinez M, Gonzalez JR, Bozack AK, et al. Cadmium, smoking, and human blood DNA methylation profiles in adults from the Strong Heart Study. Environ Health Perspect. 2020;128:067005. doi: 10.1289/EHP6345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Kattoor AJ, Pothineni NVK, Palagiri D, Mehta JL. Oxidative stress in atherosclerosis. Curr Atheroscler Rep. 2017;19:42. doi: 10.1007/s11883-017-0678-6 [DOI] [PubMed] [Google Scholar]
- 59. Baradaran A, Nasri H, Rafieian‐Kopaei M. Oxidative stress and hypertension: possibility of hypertension therapy with antioxidants. J Res Med Sci. 2014;19:358–367. [PMC free article] [PubMed] [Google Scholar]
- 60. Senoner T, Dichtl W. Oxidative stress in cardiovascular diseases: still a therapeutic target? Nutrients. 2019;11:2090. doi: 10.3390/nu11092090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Lustberg M, Silbergeld E. Blood lead levels and mortality. Arch Intern Med. 2002;162:2443–2449. doi: 10.1001/archinte.162.21.2443 [DOI] [PubMed] [Google Scholar]
- 62. Tellez‐Plaza M, Guallar E, Fabsitz RR, Howard BV, Umans JG, Francesconi KA, Goessler W, Devereux RB, Navas‐Acien A. Cadmium exposure and incident peripheral arterial disease. Circ Cardiovasc Qual Outcomes. 2013;6:626–633. doi: 10.1161/CIRCOUTCOMES.112.000134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Ujueta F, Arenas IA, Diaz D, Yates T, Beasley R, Navas‐Acien A, Lamas GA. Cadmium level and severity of peripheral artery disease in patients with coronary artery disease. Eur J Prev Cardiol. 2019;26:1456–1458. doi: 10.1177/2047487318796585 [DOI] [PubMed] [Google Scholar]
- 64. Byun G, Kim S, Kim S‐Y, Park D, Shin M‐J, Oh H, Lee J‐T. Blood lead concentrations and mortality in Korean adults: the Korea National Health and Nutrition Examination Survey with mortality follow‐up. Int J Environ Res Public Health. 2020;17:6898. doi: 10.3390/ijerph17186898 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Jeong J, Yun S‐M, Kim M, Koh YH. Association of blood cadmium with cardiovascular disease in Korea: from the Korea National Health and Nutrition Examination survey 2008–2013 and 2016. Int J Environ Res Public Health. 2020;17:6288. doi: 10.3390/ijerph17176288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Chen YW, Yang CY, Huang CF, Hung DZ, Leung YM, Liu SH. Heavy metals, islet function and diabetes development. Islets. 2009;1:169–176. doi: 10.4161/isl.1.3.9262 [DOI] [PubMed] [Google Scholar]
- 67. Ouyang P, Gottlieb SH, Culotta VL, Navas‐Acien A. EDTA chelation therapy to reduce cardiovascular events in persons with diabetes. Curr Cardiol Rep. 2015;17:96. doi: 10.1007/s11886-015-0656-y [DOI] [PubMed] [Google Scholar]
- 68. Calderon Moreno R, Navas‐Acien A, Escolar E, Nathan DM, Newman J, Schmedtje JF Jr, Diaz D, Lamas GA, Fonseca V. Potential role of metal chelation to prevent the cardiovascular complications of diabetes. J Clin Endocrinol Metab. 2019;104:2931–2941. doi: 10.1210/jc.2018-01484 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Fihn SD, Blankenship JC, Alexander KP, Bittl JA, Byrne JG, Fletcher BJ, Fonarow GC, Lange RA, Levine GN, Maddox TM, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease. Circulation. 2014;130:1749–1767. doi: 10.1161/CIR.0000000000000095 [DOI] [PubMed] [Google Scholar]
- 70. Porudominsky R, Ujueta F, Arenas IA, Lamas GA. Preliminary cost estimates of edetate disodium infusions for critical limb ischemia in patients with diabetes mellitus. Vasc Dis Manag. 2020;17:E137–E141. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1
Figure S1