
Figure 3.
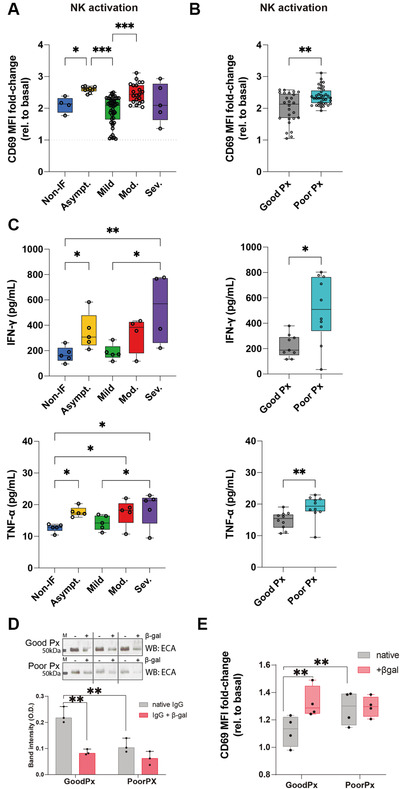
Loss of IgG galactosylation in patients with poor prognosis leads to increased NK cell activation. (A) NK cell activation quantified by the fold change of CD69 expression (compared to basal NK cells) after culture with coated IgGs from COVID‐19 patients with different severities (asymptomatic n = 9; mild n = 46; moderate n = 21; severe n = 5) and (B) prognosis (good prognosis n = 26; poor prognosis n = 39). (C) Quantification of pro‐inflammatory cytokine, IFN‐γ and TNF‐α, production by IgG‐activated NK cells. (D) ECA lectin (recognizing terminal galactose) blot and band intensity quantification of different patients’ IgGs (each patient is exhibited in paired lanes) upon β1‐4‐galactosidase S digestion (+βgal) or not (‐βgal, native), n = 8. (E) NK cell activation quantified by the fold change of CD69 expression (compared to basal NK cells) after culture with coated IgGs digested with β‐galactosidase S (+βgal) or not (native) from COVID‐19 patients. Results shown from at least two independent experiments. Each data point represents data from a single patient/subject. Mann–Whitney t‐test *p‐value < 0.05; **p‐value < 0.005.