

Abstract
Background
Adequate knowledge of root canal morphology and possible variations is essential to achieve perfect root canal treatment and overcome treatment failure. Appropriate knowledge on root and canal morphology, communication, and documentation amongst dentists will be challenging from a diagnostic and successful treatment point of view.
Methods
A total of 3420 samples were included in this study from 285 cone-beam computed tomography images of the Saudi residents, including 171 males and 114 females aged 15 to 68 years from retrospective data dated from January 2018 to April 2021. The images were examined in sagittal, axial and coronal views using a 3D version software 1.0.10.6388. The number of canal and canal morphology was recorded using Vertucci and the new classification system. The SPSS 26 was used to conduct the statistical analysis as descriptive statistics such as mean; standard deviation and frequency were calculated. The Chi-square test analysed the data with the significance level set at 0.05.
Results
A total of 285 subjects participated in the study. Majority of the participants were Saudi nationals (80.7%), followed by Indian (7.4%), Pakistani (4.2%) and other nationalities. According to Vertucci and the new classification system, Type I and 1TN1 were the most common types, followed by Type III and Type IV, and then 1TN1-2-1 and 1TN1-2 in mandibular anteriors. The prevalence of canal variations in mandibular canine was higher in females than in males (P = 0.002). Maxillary laterals and mandibular anteriors showed the significant difference in the prevalence of root canal variation in relation to the ethnicity (P = 0.001) and age of the patients. Younger patients showed more variations than the older patients (P = 0.012, P = 0.023, P = 0.001, P = 0.001) in terms of maxillary laterals, mandibular central, laterals and canines, respectively.
Conclusion
Mandibular permanent anteriors showed a wide range of canal variations and canal complexity. Males and females did not demonstrate a wide range of variation in the root canal morphology except for the canines in relation to the gender of the patients.
Keywords: Root canal, Morphology, Classification, Dental anatomy, Endodontics, Dental Pulp
Background
Most root canal treatment failures and inadequacies in endodontics are due to the limited acquaintance of the diverse anatomy of roots and variations in canal morphology [1]. Locating, disinfecting with appropriate canal preparation, and further sealing all the available canals will ultimately ensure the tooth’s good prognosis and health. Practitioners today are savvy about the conventional canal anatomy of teeth. Although the obturation and filling of the other canals are perfect, adequate knowledge of root and root canal morphological characteristics and possible variations is required to achieve perfect endodontic treatment and overcome treatment failure [1–3]. The permanent mandibular anterior teeth have reported extra roots or root canal variations compared with the maxillary anteriors. We can expect differences in canal morphologies in maxillary teeth with anomalies, such as palato–gingival groove and dens invaginatus [4].
Literature showed that the morphology in the maxillary anterior teeth was commonly present with single root and single canal, whereas mandibular anterior teeth revealed double canals [5, 6]. In addition, populations of diverse ethnic backgrounds play a role in the variation in canal morphology [4]. The morphological diversities in mandibular incisors (central and lateral) were revealed by the study conducted by Perlea et al. [7]; they stated that out of the mandibular incisors teeth, 81% had a single canal, and the other 19% had two canals, mostly varying from Weine’s class 1 to 4 [7]. Furthermore, literature shows higher prevalence of two canals in mandibular incisors [5, 8], which vary according to ethnicity, gender and age [9, 10]. Recently conducted study amongst Malaysian population revealed that mandibular anteriors showed a wide range of canal variations, and the canal complexity is significantly affected by sex, ethnicity and age [4]. Different populations also influence the complexity of the root canal morphology of anterior teeth and several studies conducted amongst Turkish, Chinese, Iranian, Jordanian and American populations revealed variations in root canal morphology of permanent anterior teeth [11–16].
To assess the morphology of the root and canal, various methods have been used, such as staining, sectioning, decalcification and clearing technique and conventional radiographs [17–20]. Furthermore, the radiographic technique with 3D images has been utilised, such as micro-computed tomography (MicroCT) and cone-beam computed tomography (CBCT). The method utilised in the current study for root and canal evaluation was CBCT to account for a non-invasive and meticulous study of the morphology. It does not interfere with the morphology of the tooth structure in any way and allows us to determine the minute anatomy of the canal structure. CBCT, different from 2D radiography, permits a 3D visualisation of the root and canal morphologies [4].
The classification introduced by Vertucci and the new classification system are used for classifying the root and canal morphology proposed by Ahmed et al. [21–23]. This new classification accounts for the various intercanal complexities that the original Vertucci’s classification, and its supplementation method might not be clarified in detail. According to several studies, the classification of the internal anatomy of several tooth types has discrepancies; for example, maxillary premolar teeth with three canals. Vertucci, Seelig [24] classified this variation as type VIII and defined it as three separate, distinct root canals extending from the pulp chamber to the apex. However, no information is provided in the classification to describe whether these canals are encased in single- or multi-rooted teeth. As a result, in most studies, three-canalled single-/double-/three-rooted maxillary premolars were still referred to as type VIII configuration [22, 25, 26]. Clearly, in terms of clinical management of teeth undergoing root canal treatment, defining the number of roots, rather than only canals, is critical, because it has implications for accessing cavity preparation, mechanical instrumentation and root canal filling procedures [27].
The current study used CBCT scan to examine root canal morphology of maxillary and mandibular anterior teeth of the Saudi subpopulation according to Vertucci’s classification and the new classification system for classifying the root canal morphology. The inclusion of maxillary and mandibular anterior teeth in the current study is important because both teeth have some anatomical differences in root canal morphology, resulting in difficulties in radiographic interpretation of their apical third, as well as a doubtful prognosis after the completion of root canal treatment. The current study aims to evaluate the root and the canal morphology in the permanent anterior teeth amongst Saudi sab population using CBCT. Furthermore, the variation in the root canal morphology in relation to the gender, age and the ethnicity of the patients was analysed.
Methods
The Local Committee of Bioethics for Research provided ethical clearance for this study with the Ethical Approval No 09-04/41. Informed consent was waived by the Committee of Bioethics for Research, College of Dentistry, Jouf University, Sakaka, Saudi Arabia, due to the retrospective nature of the study. In addition, the patients sign a general consent before any treatment or investigation is rendered, including consent to use the findings in future retrospective studies without any personal identification. The sample size of 183 scans was determined using the G power 3.1.9.4 software with x2 test, goodness-of-fit test was statistical test, and the type of power analysis was A priori. The required sample size was computed given α, power and effect size. The present study includes 3420 permanent maxillary and mandibular anterior teeth from 285 CBCT images of the patients, including 171 males and 114 females aged 15 to 68 years from retrospective data dated from January 2018 to April 2021. The patient’s records were accessed with prior permission from the dean and the hospital director, and the patients’ age, gender and ethnicity were recorded. The CBCT images were accessed through the radiology department of dental school, and the images were obtained for purposes other than this study. The patients’ name and personal data were not recorded to ensure the protection of any identifiable data on the CBCT scans that could interfere with ethical responsibilities towards patient’s data; access to the recorded data was only for the research team.
The study required CBCT images of the mandibular and maxillary anterior teeth (central, lateral incisors and canines) to be included. Images with the mandibular and maxillary anterior healthy teeth, with only minor caries or restorations in the crown, having fully developed root apex, and images without the radiographic defects were included in the study. The current study excluded root canal-treated teeth, teeth with post and core, crowns, fractured maxillary and mandibular anteriors, teeth with resorption defects, calcification, and teeth with crown and root anomalies.
The images were obtained with 90 kV and 10 mA as standardized operating specifications on the CBCT machine 3Dx SCANORA (Tuusula, Finland, Nahkelantie 160), and the data were collected. Both jaws were scanned with FOV = 80–100 (medium field of view), and a voxel size of 0.25 mm (standard resolution mode) was selected. The total scan time was 20 s; it included a 360° rotation of the X-ray–a receptor that surrounds the immobile patient. The images were inspected and interpreted at a workstation equipped with On-demand 3D version software 1.0.10.6388 (Daejeon, Korea, Yuseong-gu). The images are displayed on a 27-in. TFT monitor with 1280 1024 pixels of screen resolution and measured in three planes: coronal, axial and sagittal. The morphology of the root canals was determined and recorded (Fig. 1).
Fig. 1.

CBCT axial view of mandibular anteriors
An expert endodontist and an observer performed the study’s calibration. In the pilot study, the observer was trained and calibrated to read the CBCT images with a sample size of 50. The observer evaluated the CBCT images using sagittal, axial and coronal views to identify the root and root canal morphology, and each tooth received a single score. Disagreements were discussed, and a consensus was reached after much deliberation.
The obtained images were divided based on the patient’s age into groups (10–20, 21–30, 31– 40, 41–50, 51–60 and 61 years above). Depending on gender, the patients were divided as male or female and based on ethnicity (Saudi, Indian, Pakistani, Egyptian, Syrian and Philippines). The root canal morphology was classified using Vertucci’s classification system and the new classification system introduced by Ahmed et al. (Fig. 2), and the difference concerning age, gender and ethnicity was recorded [21, 22].
Fig. 2.
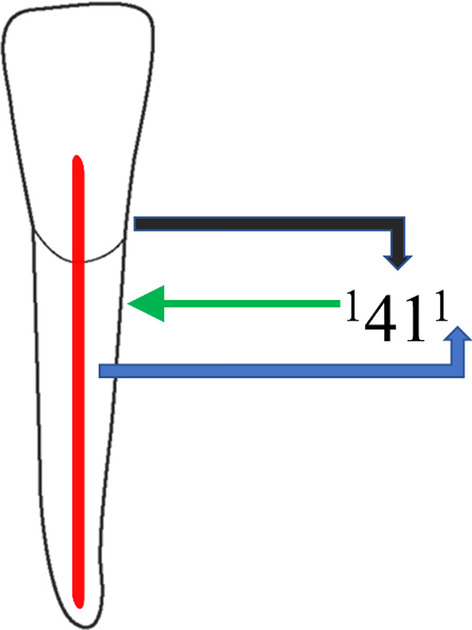
New classification system for root canal morphology of mandibular right central incisor classified using the new classification system, described as code 1411. The code consists of three components, the tooth number—black color arrow, number of roots—green color arrow and the root canal configuration—blue color arrow. The number of roots is added as a superscript before the tooth number, so it is single root and tooth number (41). Description of root canal configuration is written as superscript after the tooth number on the course of the root canal starting from the orifices [O], passing through the canal [C], ending by the foramen [F], so it is single canal
Statistical analysis
The SPSS software 26th version (Armonk, NY, USA, IBM SPSS Statistics) was used to conduct the statistical analysis as descriptive statistics, such as mean, standard deviation and frequency, were calculated. The Chi-square test was used to compare the root canal morphology in mandibular and maxillary anterior teeth and its relationship with gender, age and ethnicity of the patients; the significance level was set at 5% (p = 0.05).
Results
The characteristics of all included CBCT images are illustrated in Fig. 3. A total of 285 CBCT images of the patient were accessed through the retrospective data. The majority of samples were of Saudi nationals, and the samples consisted of 60% males and 40% females. The highest age group participating in the study was 31–40 years. According to Vertucci and the new classification systems, Table 1 shows the distribution of permanent maxillary and mandibular anterior teeth.
Fig. 3.

Descriptive analysis of sociodemographic characters (n = 285)
Table 1.
Distribution of maxillary and mandibular anterior teeth according to Vertucci and the new classification system (NC = Non-classifiable)
| Teeth position (n = 570) | Vertucci classification | New classification system | ||||||
|---|---|---|---|---|---|---|---|---|
| Type I | Type III | Type IV | NC | 1TN1 | 1TN1-2-1 | 1TN1-2 | 1TN1-2-1-2-1 | |
| Maxillary | ||||||||
| Central incisors | 558 | 12 | 558 | 12 | ||||
| Lateral incisors | 557 | 13 | 557 | 13 | ||||
| Canines | 559 | 11 | 559 | 11 | ||||
| Mandibular | ||||||||
| Central incisors | 489 | 74 | 7 | 489 | 74 | 7 | ||
| Lateral incisors | 391 | 144 | 35 | 391 | 144 | 35 | ||
| Canines | 515 | 40 | 14 | 1 | 515 | 40 | 14 | 1 |
The majority of anterior maxillary teeth was Type I of Vertucci classification and code 1TN1 of the new classification system of root canal morphology (Fig. 4). In the mandibular anterior teeth, most teeth were Type I followed by Type III and Type IV of Vertucci classification and 1TN1 followed by 1TN1-2-1 and 1TN1-2 of Ahmed classification of root canal morphology (Figs. 5, 6). A nonclassifiable type using Vertucci classification was revealed in mandibular canine; it was classified by applying the latest classification system introduced by Ahmed et al., 1TN1-2-1-2-1 (Fig. 7).
Fig. 4.

The maxillary anteriors with code 1TN1 (CBCT sagittal view)
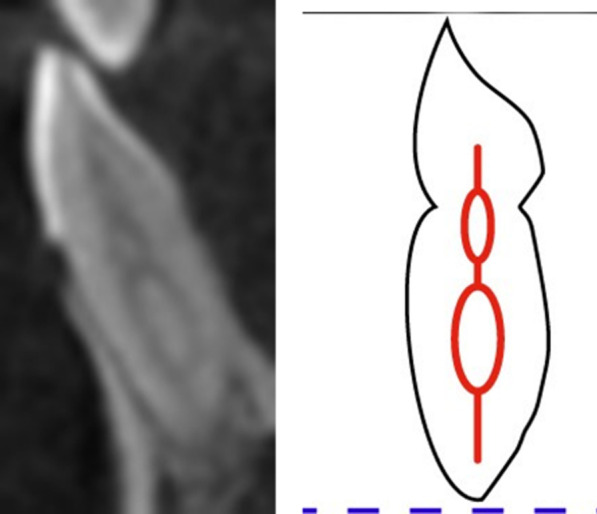
Fig. 5.

The mandibular anteriors with code 1TN1-2-1 (CBCT sagittal view)
Fig. 6.

The mandibular anteriors with code 1TN1-2 (CBCT sagittal view)
Fig. 7.
The mandibular canine with code 1TN1-2-1-2
According to Vertucci classification (Table 2) and the latest classification system provided by Ahmed et al., Table 3 reveals no statistically significant difference in permanent anterior teeth except the mandibular canine, which showed a significant difference with a p-value < 0.05 in the relationship with gender of the patients.
Table 2.
The root canal morphology in mandibular and maxillary anterior teeth and its relationship with gender according to Vertucci classification
| Teeth position | Gender (n = 570) | Vertucci classification | Chi square value | (d) | p-value | |||
|---|---|---|---|---|---|---|---|---|
| Type I | Type III | Type IV | NC | |||||
| Maxillary | ||||||||
| Central incisors | M | 336 | 6 | 0.522 | 1 | 0.470 | ||
| F | 222 | 6 | ||||||
| Lateral incisors | M | 335 | 7 | 0.024 | 1 | 0.876 | ||
| F | 222 | 6 | ||||||
| Canines | M | 337 | 6 | 0.772 | 1 | 0.380 | ||
| F | 222 | 5 | ||||||
| Mandibular | ||||||||
| Central incisors | M | 296 | 44 | 4 | 0.865 | 2 | 0.649 | |
| F | 193 | 30 | 3 | |||||
| Lateral incisors | M | 253 | 74 | 19 | 4.977 | 2 | 0.083 | |
| F | 138 | 70 | 16 | |||||
| Canines | M | 320 | 8 | 10 | 1 | 12.74 | 2 | 0.002* |
| F | 195 | 32 | 4 | |||||
Significant value < 0.05; Cross Tab, Chi Square Test
M, male; F, female; d, difference; NC, Non classifiable
Table 3.
The root canal morphology in mandibular and maxillary anterior teeth and its relationship with gender according to Ahmed classification
| Teeth position | Gender (n = 570) | Ahmed classification | Chi-square value | (d) | p-value | |||
|---|---|---|---|---|---|---|---|---|
| 1TN1 | 1TN1-2-1 | 1TN1−2 | 1TN1-2-1-2-1 | |||||
| Maxillary | ||||||||
| Central incisors | M | 336 | 6 | 1.000 f | 1 | 0.635 | ||
| F | 222 | 6 | ||||||
| Lateral incisors | M | 335 | 7 | 0.024 | 1 | 0.876 | ||
| F | 222 | 6 | ||||||
| Canines | M | 337 | 6 | 1.000 f | 1 | 0.635 | ||
| F | 222 | 5 | ||||||
| Mandibular | ||||||||
| Central incisors | M | 296 | 44 | 4 | 0.850 | 2 | 0.654 | |
| F | 193 | 30 | 3 | |||||
| Lateral incisors | M | 253 | 74 | 19 | 4.977 | 2 | 0.083 | |
| F | 138 | 70 | 16 | |||||
| Canines | M | 320 | 8 | 10 | 1 | 12.74 | 2 | 0.002* |
| F | 195 | 32 | 4 | |||||
Significant value < 0.05; Cross Tab, Chi Square Test
M, male; F, female; TN, tooth number; f, fisher exact test; d, difference
According to the classification provided by Vertucci (Table 4) and the latest classification system provided by Ahmed et al., Table 5 revealed no significant difference concerning maxillary central incisors and canines. However, a statistically significant difference was reported in maxillary lateral incisors and mandibular anterior teeth with a p-value < 0.05 in the relationship between ethnicity and permanent anterior teeth root canal morphology.
Table 4.
The root canal morphology in mandibular and maxillary anterior teeth and its relationship with ethnicity according to Vertucci classification
| Teeth position | Ethnicity (n = 570) | Vertucci classification | Chi square value | (d) | p-value | |||
|---|---|---|---|---|---|---|---|---|
| Type I | Type III | Type IV | NC | |||||
| Maxillary | ||||||||
| Central incisors | Saudi | 452 | 9 | |||||
| Indian | 40 | 2 | ||||||
| Pakistani | 22 | 1 | 2.993 | 5 | 0.701 | |||
| Egyptian | 16 | 0 | ||||||
| Syrian | 16 | 0 | ||||||
| Philippines | 12 | 0 | ||||||
| Lateral incisors | Saudi | 454 | 8 | |||||
| Indian | 42 | 3 | ||||||
| Pakistani | 17 | 2 | 50.111 | 5 | 0.001* | |||
| Egyptian | 16 | 0 | ||||||
| Syrian | 16 | 0 | ||||||
| Philippines | 12 | 0 | ||||||
| Canines | Saudi | 452 | 9 | |||||
| Indian | 41 | 1 | ||||||
| Pakistani | 22 | 1 | 1.578 | 5 | 0.904 | |||
| Egyptian | 16 | 0 | ||||||
| Syrian | 16 | 0 | ||||||
| Philippines | 12 | 0 | ||||||
| Mandibular | ||||||||
| Central incisors | Saudi | 366 | 40 | 5 | ||||
| Indian | 60 | 14 | 1 | |||||
| Pakistani | 25 | 10 | 1 | 34.695 | 10 | 0.001* | ||
| Egyptian | 16 | 4 | 0 | |||||
| Syrian | 14 | 4 | 0 | |||||
| Philippines | 8 | 2 | 0 | |||||
| Lateral incisors | Saudi | 330 | 116 | 18 | ||||
| Indian | 17 | 16 | 10 | |||||
| Pakistani | 16 | 8 | 7 | 45.047 | 10 | 0.001* | ||
| Egyptian | 12 | 4 | 0 | |||||
| Syrian | 8 | 0 | 0 | |||||
| Philippines | 8 | 0 | 0 | |||||
| Canines | Saudi | 424 | 22 | 10 | 1 | |||
| Indian | 37 | 8 | 2 | |||||
| Pakistani | 20 | 4 | 2 | 29.981 | 10 | 0.001* | ||
| Egyptian | 12 | 2 | 0 | |||||
| Syrian | 14 | 2 | 0 | |||||
| Philippines | 8 | 2 | 0 | |||||
Significant value < 0.05; Cross Tab, Chi Square Test
d, difference
Table 5.
The root canal morphology in mandibular and maxillary anterior teeth and its relationship with ethnicity according to Ahmed classification
| Teeth position | Ethnicity (n = 570) | New classification system | Chi-square value | (d) | p-value | |||
|---|---|---|---|---|---|---|---|---|
| 1TN1 | 1TN1-2-1 | 1TN1-2 | 1TN1-2-1-2-1 | |||||
| Maxillary | ||||||||
| Central incisors | Saudi | 452 | 9 | |||||
| Indian | 40 | 2 | ||||||
| Pakistani | 22 | 1 | 4.016 | 5 | 0.547 | |||
| Egyptian | 16 | 0 | ||||||
| Syrian | 16 | 0 | ||||||
| Philippines | 12 | 0 | ||||||
| Lateral incisors | Saudi | 454 | 8 | |||||
| Indian | 42 | 3 | ||||||
| Pakistani | 17 | 2 | 50.110 | 5 | 0.001* | |||
| Egyptian | 16 | 0 | ||||||
| Syrian | 16 | 0 | ||||||
| Philippines | 12 | 0 | ||||||
| Canines | Saudi | 452 | 9 | |||||
| Indian | 41 | 1 | ||||||
| Pakistani | 22 | 1 | 4.016 | 5 | 0.547 | |||
| Egyptian | 16 | 0 | ||||||
| Syrian | 16 | 0 | ||||||
| Philippines | 12 | 0 | ||||||
| Mandibular | ||||||||
| Central incisors | Saudi | 366 | 40 | 5 | ||||
| Indian | 60 | 14 | 1 | |||||
| Pakistani | 25 | 10 | 1 | 35.354 | 10 | 0.001* | ||
| Egyptian | 16 | 4 | 0 | |||||
| Syrian | 14 | 4 | 0 | |||||
| Philippines | 8 | 2 | 0 | |||||
| Lateral incisors | Saudi | 330 | 116 | 18 | ||||
| Indian | 17 | 16 | 10 | |||||
| Pakistani | 16 | 8 | 7 | 45.047 | 10 | 0.001* | ||
| Egyptian | 12 | 4 | 0 | |||||
| Syrian | 8 | 0 | 0 | |||||
| Philippines | 8 | 0 | 0 | |||||
| Canines | Saudi | 424 | 22 | 10 | 1 | |||
| Indian | 37 | 8 | 2 | |||||
| Pakistani | 20 | 4 | 2 | 29.981 | 10 | 0.001* | ||
| Egyptian | 12 | 2 | 0 | |||||
| Syrian | 14 | 2 | 0 | |||||
| Philippines | 8 | 2 | 0 | |||||
Significant value < 0.05; Cross Tab, Chi Square Test
TN, tooth number; d-difference
According to Vertucci classification (Table 6) and the latest classification system provided by Ahmed et al., Table 7 demonstrates no significant difference concerning maxillary central incisors and canines. However, a statistically significant difference was reported in maxillary lateral incisors and mandibular anterior teeth with a p-value < 0.05 in the relationship with age; younger patients showed more root canal variations when compared with the older patients.
Table 6.
The root canal morphology in mandibular and maxillary anterior teeth and its relationship with age according to Vertucci classification
| Teeth position | Age (years) (n = 570) | Vertucci classification | Chi square value | (d) | p-value | |||
|---|---|---|---|---|---|---|---|---|
| Type I | Type III | Type IV | NC | |||||
| Maxillary | ||||||||
| Central incisors | 10–20 | 36 | 2 | |||||
| 21–30 | 104 | 2 | ||||||
| 31–40 | 178 | 4 | 7.831 | 5 | 0.166 | |||
| 41–50 | 118 | 2 | ||||||
| 51–60 | 90 | 2 | ||||||
| 60 above | 32 | 0 | ||||||
| Lateral incisors | 10–20 | 38 | 2 | |||||
| 21–30 | 105 | 2 | ||||||
| 31–40 | 174 | 5 | 14.582 | 5 | 0.012* | |||
| 41–50 | 116 | 2 | ||||||
| 51–60 | 92 | 2 | ||||||
| 60 above | 32 | 0 | ||||||
| Canines | 10–20 | 36 | 2 | |||||
| 21–30 | 104 | 2 | ||||||
| 31–40 | 180 | 4 | 8.106 | 5 | 0.150 | |||
| 41–50 | 116 | 2 | ||||||
| 51–60 | 91 | 1 | ||||||
| 60 above | 32 | 0 | ||||||
| Mandibular | ||||||||
| Central incisors | 10–20 | 34 | 12 | 0 | ||||
| 21–30 | 92 | 24 | 2 | |||||
| 31–40 | 160 | 22 | 2 | 20.780 | 10 | 0.023* | ||
| 41–50 | 91 | 8 | 2 | |||||
| 51–60 | 84 | 8 | 1 | |||||
| 60 above | 28 | 0 | 0 | |||||
| Lateral incisors | 10–20 | 33 | 4 | 4 | ||||
| 21–30 | 52 | 52 | 2 | |||||
| 31–40 | 112 | 52 | 24 | 45.065 | 10 | 0.001* | ||
| 41–50 | 104 | 12 | 1 | |||||
| 51–60 | 62 | 20 | 4 | |||||
| 60 above | 28 | 4 | 0 | |||||
| Canines | 10–20 | 26 | 12 | 2 | ||||
| 21–30 | 88 | 4 | 6 | |||||
| 31–40 | 173 | 12 | 2 | 1 | 43.472 | 5 | 0.001* | |
| 41–50 | 108 | 8 | 2 | |||||
| 51–60 | 92 | 4 | 2 | |||||
| 60 above | 28 | 0 | 0 | |||||
Significant value < 0.05; Cross Tab, Chi Square Test
Yrs, years; d, difference
Table 7.
The root canal morphology in mandibular and maxillary anterior teeth and its relationship with age according to Ahmed classification
| Teeth position | Age (n = 570) | Ahmed classification | Chi-square value | (d) | p-value | |||
|---|---|---|---|---|---|---|---|---|
| 1TN1 | 1TN1-2-1 | 1TN1−2 | 1TN1-2-1-2-1 | |||||
| Maxillary | ||||||||
| Central incisors | 10–20 | 36 | 2 | |||||
| 21–30 | 104 | 2 | ||||||
| 31–40 | 178 | 4 | 10.419 | 5 | 0.064 | |||
| 41–50 | 118 | 2 | ||||||
| 51–60 | 90 | 2 | ||||||
| 60 above | 32 | 0 | ||||||
| Lateral incisors | 10–20 | 38 | 2 | |||||
| 21–30 | 105 | 2 | ||||||
| 31–40 | 174 | 5 | 14.582 | 5 | 0.012* | |||
| 41–50 | 116 | 2 | ||||||
| 51–60 | 92 | 2 | ||||||
| 60 above | 32 | 0 | ||||||
| Canines | 10–20 | 36 | 2 | |||||
| 21–30 | 104 | 2 | ||||||
| 31–40 | 180 | 4 | 10.419 | 5 | 0.064 | |||
| 41–50 | 116 | 2 | ||||||
| 51–60 | 91 | 1 | ||||||
| 60 above | 32 | 0 | ||||||
| Mandibular | ||||||||
| Central incisors | 10–20 | 34 | 12 | 0 | ||||
| 21–30 | 92 | 24 | 2 | |||||
| 31–40 | 160 | 22 | 2 | 20.627 | 10 | 0.024* | ||
| 41–50 | 91 | 8 | 2 | |||||
| 51–60 | 84 | 8 | 1 | |||||
| 60 above | 28 | 0 | 0 | |||||
| Lateral incisors | 10–20 | 33 | 4 | 4 | ||||
| 21–30 | 52 | 52 | 2 | |||||
| 31–40 | 112 | 52 | 24 | 45.065 | 10 | 0.001* | ||
| 41–50 | 104 | 12 | 1 | |||||
| 51–60 | 60 | 20 | 4 | |||||
| 60 above | 28 | 4 | 0 | |||||
| Canines | 10–20 | 26 | 12 | 2 | ||||
| 21–30 | 88 | 4 | 6 | |||||
| 31–40 | 173 | 12 | 2 | 1 | 43.472 | 10 | 0.001* | |
| 41–50 | 108 | 8 | 2 | |||||
| 51–60 | 92 | 4 | 2 | |||||
| 60 above | 28 | 0 | 0 | |||||
Significant value < 0.05; Cross Tab, Chi Square Test
yrs, years; TN, tooth number; d, difference
Discussion
This study was conducted amongst Saudi subpopulations, where majority of participants were males (60%) and Saudi nationals (80.7%) with age group 31–40 (33%). According to Vertucci and the new classification systems, our study results revealed that the prevalence of root canal variation in relation to ethnicity and age of the patients was significantly different in the maxillary laterals and mandibular anteriors, with younger patients showing more variations than older patients. The mandibular permanent anterior teeth exhibit a wide range of morphological differences in the root canal.
The motive of this study by including two different classification systems was to clarify the aberrations in question and the specific region of occurrence. The classification system by Vertucci, though being a universal one and widely known, might not provide exhaustive information about the tooth and its anomaly. Furthermore, Vertucci’s classification system does not classify the number of roots [23]. In comparison, the new classification system by Ahmed et al. provides a single code that classifies the particular tooth with the number of roots and the canal morphology [21]. In addition, it helps us understand complex intercanal communications in teeth [2].
The radiographic tool used for this study was CBCT. It possesses an array of qualities that are crucial for analysis. It is non-invasive and provides intricate external and internal details of the tooth and nearby structures [28–30]. It has a comparatively low radiation dose and is more economical than a CT scan. Moreover, we can expect almost accurate measurements given that CBCT voxels are isotropic [31, 32]. Previous studies have shown that CBCT is very reliable for demonstrating the root canal morphology and used for cross-sectional surveys, where the analysis involves a large sample size [33, 34].
The permanent anterior teeth have complex roots and canals, especially mandibular anteriors. Generally they are single-rooted; thus, we can also expect double roots or canals, apical ramification, a lateral branch of a root canal or apical furcation. These variabilities can complicate RCT for practitioners. The most regular type of configuration of root canal was Type I, followed by Type III from the Vertucci Classification, which corresponds to similar findings from other studies [4, 35]. Studies conducted among other populations, such as Israeli (89.7%), Brazilian (90.5%) and Iranian (97.6%), have reported similar findings [36–38]. All permanent anteriors under consideration had single roots, corresponding with findings from other studies [39].
Most mandibular anterior teeth configurations were Type I, followed by Type III and Type V of Vertucci classification. This finding is partly consistent with the study conducted amongst the Saudi Arabia and Indian subpopulation [40, 41]. The authors revealed the frequency of Vertucci’s Type I in mandibular laterals as most common, followed by Type III and least of all Type V. Another study showed that more than half of the mandibular centrals and laterals analysed had Type I [42, 43]. On the contrary, a study conducted by Mashyakhy showed that most mandibular incisors were Type III [44]. At the same time, studies conducted on Belgium, Iran and Chile populations showed less than 20% frequency [45–47].
Studies conducted to locate differences between root canal morphologies across different genders have shown significant differences, and similar findings were reported in this study. More variations were found in males than the samples obtained from the female population. This finding corresponds to findings obtained from similar studies conducted in Turkish and Indian populations [13, 48]. No significant difference was identified concerning maxillary canines and incisors in terms of age. However, a statistically significant difference was reported in upper lateral incisors and lower anterior teeth. A study by Lin et al. showed the insignificant difference between the age factor of the patients and the frequency of two root canals amongst the sample size [39]. Vertucci is widely applied to classify the morphology of root canal, but it has also been shown to have several deficiencies [13]. Therefore, the new system for classification by Ahmed et al. is more accurate because it offers a better demonstration of the number of roots and their canal morphology. Practitioners ought to be equipped with current advances in classification systems, the appropriate diagnostic tools and the possibilities in different anatomical aberrations. If conducted tactfully, with such skill, successful endodontic treatment can be achieved without surgical intervention.
Limitations
The root canal morphology is capable of alteration over time. With age, secondary dentin deposition is found, thereby explaining that the results are a more significant part of the sample size above the age of 30 years. The present study investigated the root canal morphology of permanent anterior teeth in a Saudi subpopulation that used a voxel size of 0.25 mm, which is a limiting factor; it might have also been influenced by limitations of resolution as the canals become calcified and narrower. However, using a high-resolution imaging modality improves visualisation of morphology of root canal in anterior single-rooted teeth. One of the major flaws of Vertucci classification is that it does not consider the number of total roots present. Any tooth found to have more than one root is classified directly as Type IV or Type V, which is inaccurate because it would have direct implications on the endodontic procedure or placement of posts if required.
Conclusions
Mandibular permanent anterior teeth demonstrate an extensive series of morphological difference in the root canal. Males and females did not demonstrate a wide range of variation in the morphology of root canal except for the canines. Maxillary laterals and mandibular anteriors showed the significant difference in prevalence of root canal variation in relation to the ethnicity and age of the patients. Younger patients showed more variations when compared with the older patients.
Acknowledgements
The authors want to thank Mr Ali Mussa for his assistance in editing 3D figures preparation.
Abbreviations
- CBCT
Cone-beam computed tomography
- MicroCT
Micro-computed tomography
- 2D
Two-dimensional
- 3D
Three-dimensional
Author contributions
Conceptualization: AI, MIK. Methodology: MIK. Formal analysis and investigation: MKA, OK, SMA, HAA and MAA. Writing—original draft preparation: AI, MIK, AHA. Writing—review and editing: TYN, KCS, RI and MIK. All authors read and approved the final manuscript.
Funding
The authors extend their appreciation to the Deanship of Scientific Research at Jouf University for funding this work through research grant no. DSR-(2021-01-0120).
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Local committee of Bioethics for Research, College of Dentistry, Jouf University. Sakaka, Saudi Arabia with the Ethics approval no 09-04/41. Informed consent was waived by the committee of Bioethics for Research, College of Dentistry, Jouf University. Sakaka, Saudi Arabia due to retrospective nature of the study. Additionally, the patients sign a general consent before any treatment or investigation is rendered which includes a consent to use the findings in future retrospective studies without any personal identification.
Consent to published
Not applicable.
Competing interest
The authors declare no conflict of interest.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Azhar Iqbal and Mohmed Isaqali Karobari contributed equally to this work
Contributor Information
Azhar Iqbal, Email: dr.azhar.iqbal@jodent.org.
Mohmed Isaqali Karobari, Email: dr.isaq@gmail.com.
References
- 1.Buchanan GD, et al. Root and canal configurations of maxillary premolars in a South African subpopulation using cone beam computed tomography and two classification systems. J Oral Sci. 2020;62(1):93–97. doi: 10.2334/josnusd.19-0160. [DOI] [PubMed] [Google Scholar]
- 2.Karobari M, et al. Should inter-canal communications be included in the classification of root canal systems? Int Endod J. 2019;52(6):917–919. doi: 10.1111/iej.13106. [DOI] [PubMed] [Google Scholar]
- 3.Al Mheiri E, et al. Evaluation of root and canal morphology of maxillary permanent first molars in an Emirati population; a cone-beam computed tomography study. BMC Oral Health. 2020;20(1):1–9. doi: 10.1186/s12903-020-01269-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Karobari MI, et al. Root and canal morphology of the anterior permanent dentition in Malaysian population using two classification systems: a CBCT clinical study. Australian Endodont J. 2020. [DOI] [PubMed]
- 5.Rankine-Wilson R, Henry P. The bifurcated root canal in lower anterior teeth. J Am Dent Assoc. 1965;70(5):1162–1165. doi: 10.14219/jada.archive.1965.0189. [DOI] [PubMed] [Google Scholar]
- 6.Nogueira Leal da Silva EJ, et al. Evaluation of root canal configuration of maxillary and mandibular anterior teeth using cone beam computed tomography: an in-vivo study. Quintessence Int. 2016;47(1). [DOI] [PubMed]
- 7.Perlea P, et al. Endodontic configuration of the lower incisors in a Romanian population: a radiological study. Rom J Morphol Embryol. 2013;54(3 Suppl):775–778. [PubMed] [Google Scholar]
- 8.Nogueira Leal da Silva EJ, et al. Evaluation of root canal configuration of maxillary and mandibular anterior teeth using cone beam computed tomography: an in-vivo study. Quintessence Int. 2016;47(1):19–24. doi: 10.3290/j.qi.a34807. [DOI] [PubMed] [Google Scholar]
- 9.Cleghorn B, Christie W, Dong C. Anomalous mandibular premolars: a mandibular first premolar with three roots and a mandibular second premolar with a C-shaped canal system. Int Endod J. 2008;41(11):1005–1014. doi: 10.1111/j.1365-2591.2008.01451.x. [DOI] [PubMed] [Google Scholar]
- 10.Zhengyan Y, et al. Cone-beam computed tomography study of the root and canal morphology of mandibular permanent anterior teeth in a Chongqing population. Therapeut Clin Risk Manag. 2016;12(2):19–25. doi: 10.2147/TCRM.S95657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Caliskan MK, et al. Root canal morphology of human permanent teeth in a Turkish population. J Endodontics. 1995;21(4):200–204. doi: 10.1016/S0099-2399(06)80566-2. [DOI] [PubMed] [Google Scholar]
- 12.Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dent Assoc. 1978;97(1):47–50. doi: 10.14219/jada.archive.1978.0443. [DOI] [PubMed] [Google Scholar]
- 13.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endodontics. 2004;30(6):391–398. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 14.Weng X-L, et al. Root canal morphology of permanent maxillary teeth in the Han nationality in Chinese Guanzhong area: a new modified root canal staining technique. J Endodontics. 2009;35(5):651–656. doi: 10.1016/j.joen.2009.02.010. [DOI] [PubMed] [Google Scholar]
- 15.Rahimi S, et al. Prevalence of two root canals in human mandibular anterior teeth in an Iranian population. Indian J Dent Res. 2013;24(2):234–236. doi: 10.4103/0970-9290.116694. [DOI] [PubMed] [Google Scholar]
- 16.Al-Qudah A, Awawdeh L. Root canal morphology of mandibular incisors in a Jordanian population. Int Endod J. 2006;39(11):873–877. doi: 10.1111/j.1365-2591.2006.01159.x. [DOI] [PubMed] [Google Scholar]
- 17.Gupta B, et al. Transparent tooth model: a study of root canal morphology using different reagents. Eur J Gen Dentist. 2014;3(1):66–70. doi: 10.4103/2278-9626.126215. [DOI] [Google Scholar]
- 18.Habib AA, Kalaji MN. Root canal configurations of the first and second mandibular premolars in the population of north Syria. J Taibah Univ Med Sci. 2015;10(4):391–395. [Google Scholar]
- 19.Aminsobhani M, et al. Evaluation of the root and canal morphology of mandibular permanent anterior teeth in an Iranian population by cone-beam computed tomography. J Dentistry (Tehran, Iran) 2013;10(4):358–366. [PMC free article] [PubMed] [Google Scholar]
- 20.Cotton TP, et al. Endodontic applications of cone-beam volumetric tomography. J Endodontics. 2007;33(9):1121–1132. doi: 10.1016/j.joen.2007.06.011. [DOI] [PubMed] [Google Scholar]
- 21.Ahmed H, et al. A new system for classifying root and root canal morphology. Int Endod J. 2017;50(8):761–770. doi: 10.1111/iej.12685. [DOI] [PubMed] [Google Scholar]
- 22.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–599. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 23.Karobari MI, et al. Root and root canal morphology classification systems. Int J Dent. 2021;2021. [DOI] [PMC free article] [PubMed]
- 24.Vertucci F, Seelig A, Gillis R. Root canal morphology of the human maxillary second premolar. Oral Surg Oral Med Oral Pathol. 1974;38(3):456–464. doi: 10.1016/0030-4220(74)90374-0. [DOI] [PubMed] [Google Scholar]
- 25.Velmurugan N, et al. Maxillary second premolar with three roots and three separate root canals. Aust Endod J. 2005;31(2):73–75. doi: 10.1111/j.1747-4477.2005.tb00230.x. [DOI] [PubMed] [Google Scholar]
- 26.Peiris R. Root and canal morphology of human permanent teeth in a Sri Lankan and Japanese population. Anthropol Sci. 2008;116(2):123–133. doi: 10.1537/ase.070723. [DOI] [Google Scholar]
- 27.Ahmed HMA, Cheung G. Accessory roots and root canals in maxillary premolar teeth: a review of a critical endodontic challenge. ENDO Endod Prac Today. 2012;6(1):7–18. [Google Scholar]
- 28.Mozzo P, et al. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol. 1998;8(9):1558–1564. doi: 10.1007/s003300050586. [DOI] [PubMed] [Google Scholar]
- 29.Bornstein MM, et al. Comparison of intraoral radiography and limited cone beam computed tomography for the assessment of root-fractured permanent teeth. Dent Traumatol. 2009;25(6):571–577. doi: 10.1111/j.1600-9657.2009.00833.x. [DOI] [PubMed] [Google Scholar]
- 30.Patel S, Horner K. The use of cone beam computed tomography in endodontics. Int Endod J. 2009;42(9):755–756. doi: 10.1111/j.1365-2591.2009.01607.x. [DOI] [PubMed] [Google Scholar]
- 31.Peters OA, et al. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res. 2000;79(6):1405–1409. doi: 10.1177/00220345000790060901. [DOI] [PubMed] [Google Scholar]
- 32.Kaya S, et al. Cone-beam dental computerized tomography for evaluating changes of aging in the dimensions central superior incisor root canals. Med Oral Patol Oral Cir Bucal. 2011;16(3):e463–e466. doi: 10.4317/medoral.16.e463. [DOI] [PubMed] [Google Scholar]
- 33.Altunsoy M, et al. A cone-beam computed tomography study of the root canal morphology of anterior teeth in a Turkish population. Eur J Dent. 2014;8(03):302–306. doi: 10.4103/1305-7456.137630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Blattner TC, et al. Efficacy of cone-beam computed tomography as a modality to accurately identify the presence of second mesiobuccal canals in maxillary first and second molars: a pilot study. J Endod. 2010;36(5):867–870. doi: 10.1016/j.joen.2009.12.023. [DOI] [PubMed] [Google Scholar]
- 35.Mashyakhy M, Gambarini G. Root and root canal morphology differences between genders: a comprehensive in-vivo CBCT study in a Saudi population. Acta Stomatol Croat. 2019;53(3):213. doi: 10.15644/asc53/3/5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Haghanifar S, et al. Morphologic assessment of mandibular anterior teeth root canal using CBCT. Acta Medica Academica. 2017;46(2). [DOI] [PubMed]
- 37.Shemesh A, et al. Root anatomy and root canal morphology of mandibular canines in Israeli population. Refu'at ha-peh veha-shinayim (1993) 2016;33(1):19–23. [PubMed] [Google Scholar]
- 38.Silva EJNL, et al. Evaluation of root canal configuration of maxillary molars in a Brazilian population using cone-beam computed tomographic imaging: an in vivo study. J Endod. 2014;40(2):173–176. doi: 10.1016/j.joen.2013.10.002. [DOI] [PubMed] [Google Scholar]
- 39.Lin Z, et al. Use of CBCT to investigate the root canal morphology of mandibular incisors. Surg Radiol Anat. 2014;36(9):877–882. doi: 10.1007/s00276-014-1267-9. [DOI] [PubMed] [Google Scholar]
- 40.Ghabbani HM, Marghalani AA, Alabiri HR. Assessment of root canal morphology of mandibular incisors using cone-beam computed tomography among residents of Al-Madinah Al-Munawara Region, Saudi Arabia. Eur J Gen Dent. 2020;9(1):40. doi: 10.4103/ejgd.ejgd_141_19. [DOI] [Google Scholar]
- 41.Verma GR, et al. Cone beam computed tomography study of root canal morphology of permanent mandibular incisors in Indian subpopulation. Pol J Radiol. 2017;82:371. doi: 10.12659/PJR.901840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Saati S, et al. Root morphology and number of canals in mandibular central and lateral incisors using cone beam computed tomography. Braz Dent J. 2018;29:239–244. doi: 10.1590/0103-6440201801925. [DOI] [PubMed] [Google Scholar]
- 43.Shemesh A, et al. Root canal morphology evaluation of central and lateral mandibular incisors using cone-beam computed tomography in an Israeli population. J Endod. 2018;44(1):51–55. doi: 10.1016/j.joen.2017.08.012. [DOI] [PubMed] [Google Scholar]
- 44.Alenezi MA, et al. Root and root canal morphology of permanent mandibular incisors in a Kuwaiti subpopulation: a cone-beam computed tomography study. Saudi Endod J. 2021;11(3):315. [Google Scholar]
- 45.Baxter S, Jablonski M, Hülsmann M. Cone-beam-computed-tomography of the symmetry of root canal anatomy in mandibular incisors. J Oral Sci. 2020;62(2):180–183. doi: 10.2334/josnusd.19-0113. [DOI] [PubMed] [Google Scholar]
- 46.Pedemonte E, et al. Root and canal morphology of mandibular premolars using cone-beam computed tomography in a Chilean and Belgian subpopulation: a cross-sectional study. Oral Radiol. 2018;34(2):143–150. doi: 10.1007/s11282-017-0297-5. [DOI] [PubMed] [Google Scholar]
- 47.Mirhosseini F, et al. Evaluation of root canal anatomy in mandibular incisors using CBCT imaging technique in an iranian population. J Dent. 2019;20(1):24. doi: 10.30476/DENTJODS.2019.44559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Jaju PP, Jaju SP. Clinical utility of dental cone-beam computed tomography: current perspectives. Clin Cosmet Investig Dent. 2014;6:29. doi: 10.2147/CCIDE.S41621. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.