
Figure 1. Percutaneous Intramyocardial Septal Radiofrequency Ablation (PIMSRA) Procedure Illustration and Echo Imaging.
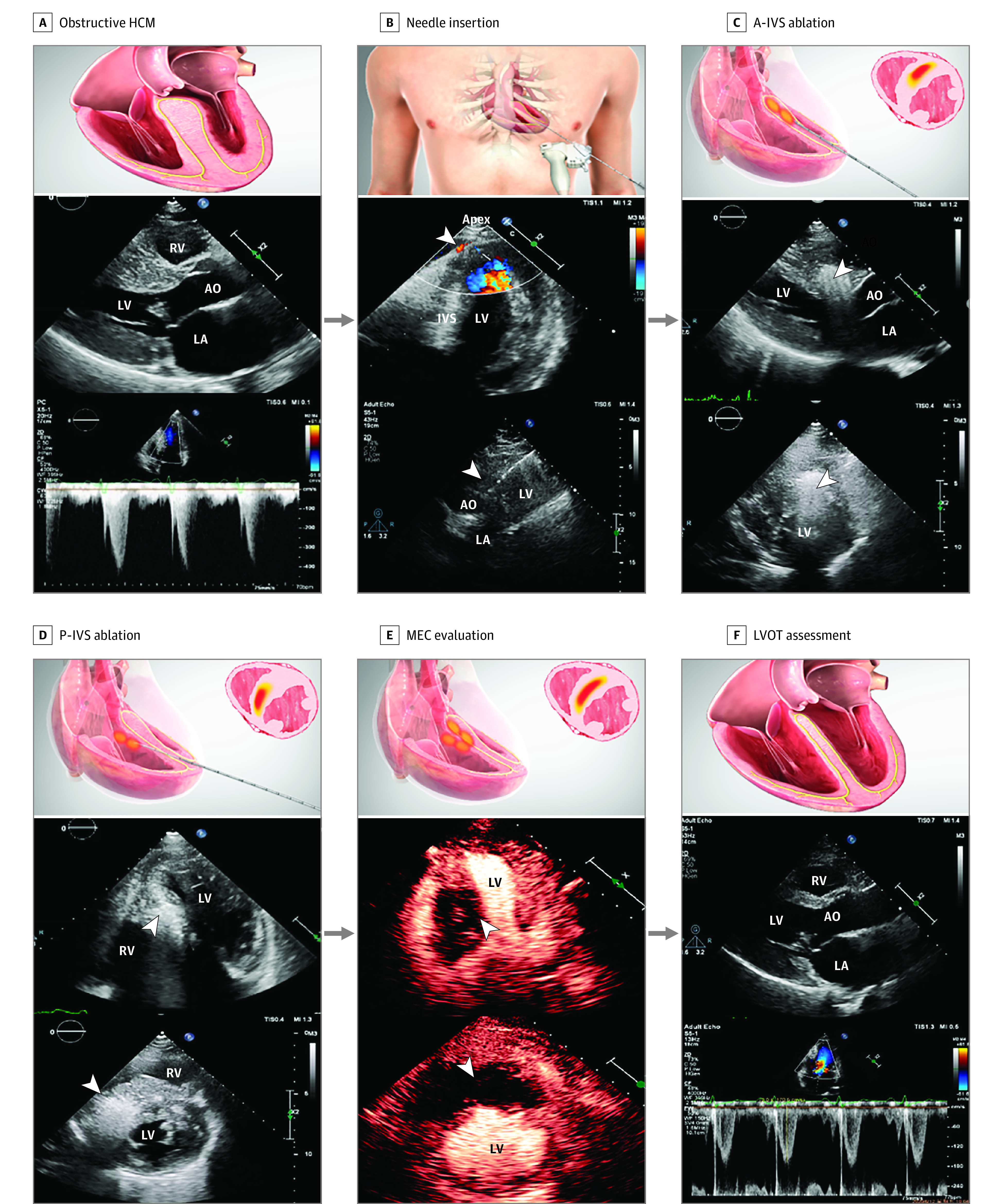
A, Before PIMSRA, the ventricular septum was hypertrophic and left ventricular outflow tract (LVOT) was obstructive. B, The needle was percutaneously inserted through the left ventricular (LV) apex, while using color Doppler guidance to avoid vascular injury. The arrowhead showed vessels at the apex and the needle in the intraventricular septum (IVS) through the guide frame. C, Basal and midanterior ventricular septum was ablated. The bright echo signal as the arrowhead showed was the ablation area. D, Then, the needle was withdrawn and repositioned in the hypertrophic posterior septum for ablation. E, After the basal and mid portion of anterior IVS (A-IVS) and posterior IVS (P-IVS) ablation, contrast echo was used to assess whether the ablation range was adequate. F, Nine months after PIMSRA, the ventricular septum became thinner and LVOT peak gradient decreased. AO indicates aorta; HCM, hypertrophic cardiomyopathy; LA, left atrium; MEC, myocardial echo contrast; RV, right ventricle.