
Figure 1. Schematic illustration of various common renal diseases.
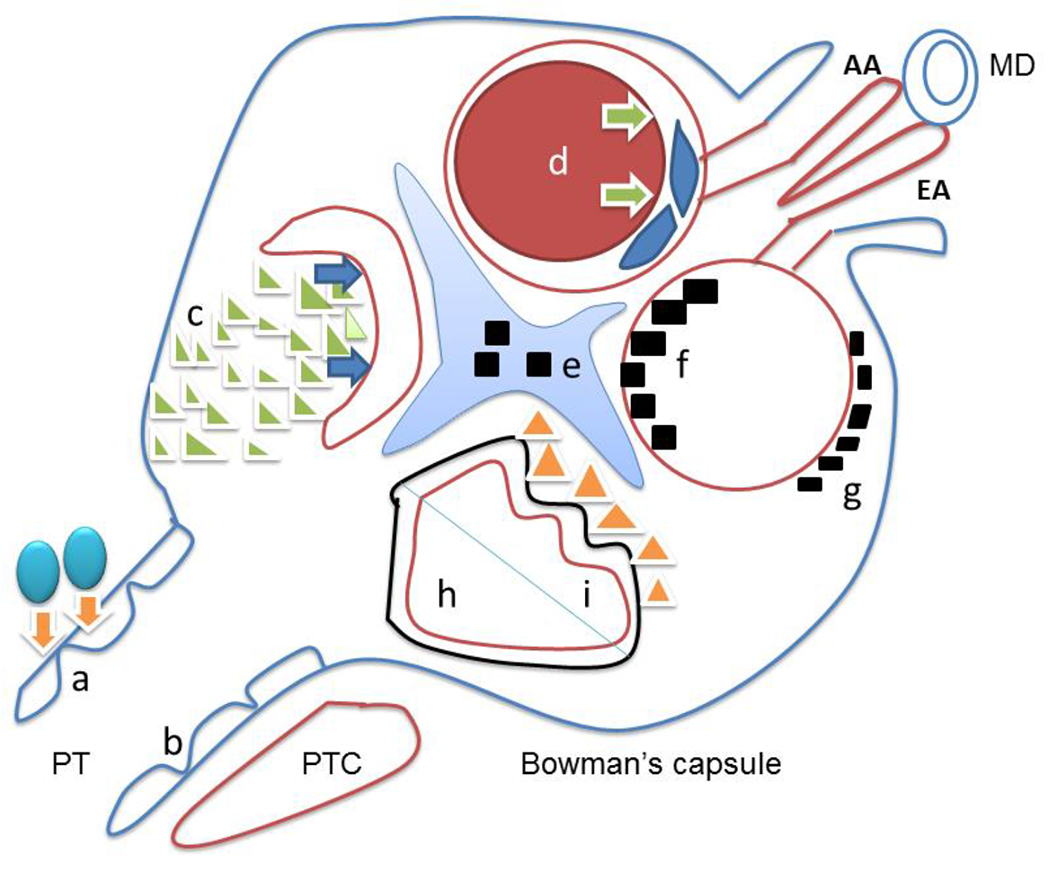
Letters represent following renal diseases: a. acute cellular rejection is due to T lymphocytes infiltration (blue balls) to renal tubules (orange arrows); b. acute tubular injury with flattened epithelium (blue line) usually results from either ischemic or toxic insult to proximal tubules; c. crescentic glomerulonephritis associated with ANCA or anti-glomerular basement antibody results from the proliferation of parietal epithelial cells (green triangles), leading to collapsing glomerular capillary loops (blue arrows) and acute renal failure; d. thrombotic microangiopathy with multiple etiologies, is characterized with thrombosis (red circle) causing luminar obstruction (green arrows) and edematous glomerular endothelial cells (blue spindle endothelial cells); e. mesangial deposits are seen in IgA nephropathy; f. subendothelial deposits are usually found in membranoprolifeative glomerulonephritis and diffuse proliferative lupus nephritis (black squares within red glomerular basement membrane) ; g. subepithelial deposits seen in membranous glomerulopathy are due to primary or secondary etiologies (black squares outside the red glomerular basement membrane); h. minimal change disease and focal segmental glomerulosclerosis (NOS) typically shows diffuse fusion of fusion processes (solid black line outside of red glomerular basement membrane); i, collapsing glomerulopathy is characterized by collapsed glomerular basement membrane (curved red line) with proliferative podocytes (yellow triangles). AA – afferent arteriole, EA – efferent arteriole, MD – macular densa, PT – proximal tubules, PTC – peritubular capillaries.