

Abstract
Introduction
Penetrating cardiac injuries are emergencies that require prompt surgical management. Most of these injuries are caused by gunshots or stab wounds however the incidence of nail-gun injuries is rising due to their availability and widespread use. Cardiac injuries caused by nail-guns are often self-inflicted. These injuries almost always require operative management with a sternotomy or thoracotomy.
Case report
This case report describes a 47-year-old male with two self-inflicted nail-gun wounds to the chest. He presented in a stable condition and subsequently underwent an emergency sternotomy to repair a penetrating cardiac injury. We highlight our diagnostic and operative approach to this injury and present a contemporary narrative review of similar cases.
Conclusion
Almost all cases of penetrating trauma caused by nail-gun injuries require urgent surgery. Some cases require the use of cardiopulmonary bypass. In this case, the use of the Medtronic® urchin apical suction device, usually reserved for off pump cardiac surgery, facilitated exposure and repair of the lateral wall of the left ventricle.
Keywords: Penetrating cardiac injury, Nailgun, Trauma
Introduction
Penetrating cardiac injuries are emergencies that require prompt surgical management. Although commonly caused by gunshots and stab wounds, case reports detailing penetrating injuries caused by pneumatically fired nail-guns have also been described [1], [2], [3]. The incidence of these injuries is on the rise as nail-guns are being utilised more frequently in industrial and civil settings [3]. The majority of cases encompass orthopaedic trauma caused by nail-guns fired accidentally into the non-dominant arm [1]. Cardiac injuries caused by nail-guns are often self-inflicted [2]. The mortality rate given the relative infrequency of these injuries remains unclear [3]. These injuries generally require operative management in the form of a sternotomy or thoracotomy [3]. The right ventricle is most commonly affected due to its anterior location; however, reports exist of injury to the left ventricle, atria and even the thoracic aorta [3], [4]. This case report describes a 47-year-old male with two self-inflicted nail-gun wounds to the chest. We highlight our diagnostic and operative approach to this injury and present a contemporary narrative review of similar cases.
Case report
A 47-year-old male presented to the emergency department four hours after a suicide attempt in which he fired two nails into his chest. He remained stable and on examination, there were two puncture wounds noted; one in his third intercostal space (ICS) left of the sternal border and one in the 3rd intercostal space, midclavicular line (Fig. 1). Chest X-ray revealed two nails overlying the apex of the cardiac silhouette, with no evidence of a haemothorax or pneumothorax (Fig. 2). A formal ultrasound demonstrated a 1.5 cm pericardial effusion adjacent to the left ventricle. He subsequently underwent a cardiac gated CT scan that one nail penetrated the myocardium, with a surrounding pericardial effusion and the second nail was abutting the left ventricle (Fig. 3). The decision was then made to take the patient emergently to the operating theatre for exploration and repair.
Fig. 1.

Location of wounds.
Fig. 2.

Chest-Xray with nails evident.
Fig. 3.

Axial CT (reconstructed window) with nails.
An intraoperative trans-oesophageal echocardiogram (TOE) was performed, demonstrating a pericardial effusion with early evidence of tamponade. We performed a median sternotomy and had a cardiopulmonary bypass (CPB) circuit primed if needed. On entering the pericardium, a moderate volume of blood and clot was released under pressure, however initially the nails were not visible. Three small tears were noted on the lateral wall of the left ventricle with no evidence of active bleeding (Fig. 4). A pericardial stay was placed, and the apex of the heart was lifted using the Medtronic® urchin apical suction device, providing excellent exposure to the myocardial injuries on the lateral wall of the heart (Fig. 4). There was no haemodynamic compromise as a result of lifting the heart. The myocardial injury was sealed with Bioglue® with a bovine pericardial patch placed overlying the injuries to reinforce the repair (Fig. 5). Attention was then drawn to the location of the second nail. The left pleura was opened revealing the path of the nail (Fig. 6). There was no lung injury or active bleeding, and the nail was removed under direct vision. The mediastinum was washed with copious warm saline, and three drains (two pericardia and left pleural) were placed.
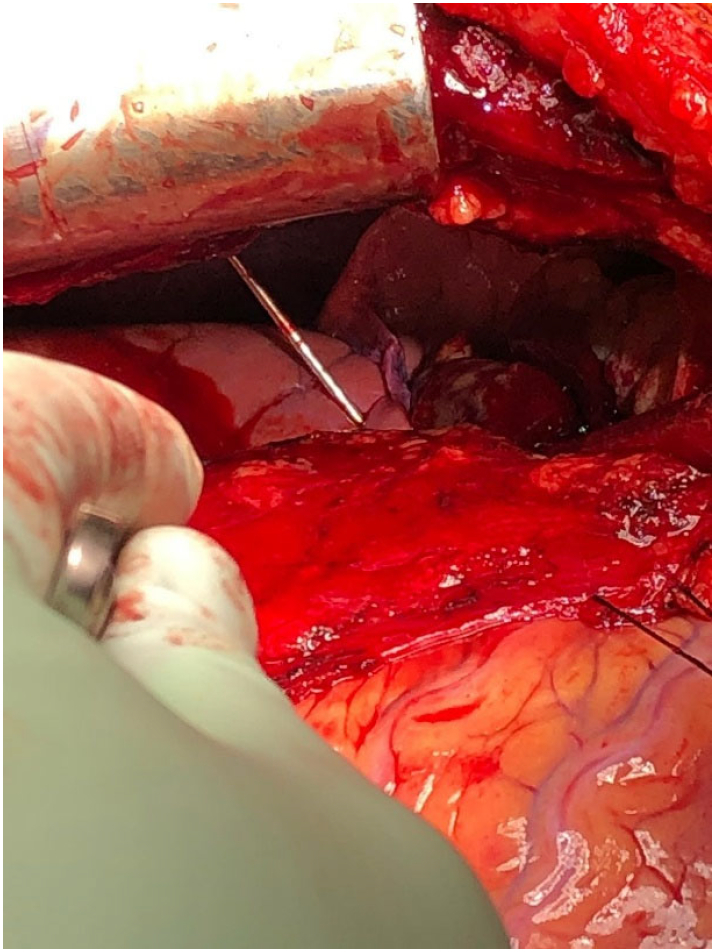
Fig. 4.

Off pump retractor and view of myocardial injury.
Fig. 5.

Bioglue and bovine pericardial patch.
Fig. 6.
Opened left pleura and nail.
The patient remained stable and was extubated postoperative-day one. He remained on broad spectrum intravenous antibiotics during his hospital admission. He was discharged to a mental health facility on postoperative day 7. A narrative review of case reports pertaining to nail-gun related cardiac injury was performed [4], [5], [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20] (Supplementary Table 1). Medical illustrations and case reports of paediatric patients (under 16) were excluded.
Discussion
Pneumatic nail-guns have been in use since the 1960's. These tools can be divided into low- and high-velocity types, with speeds up to 150 m/s. Currently, the majority of nail-gun trauma are inadvertent orthopaedic injuries in the non-dominant arm, however, the incidence of nail-gun related cardiac injuries is on the rise due to their widespread use and availability [3], [19]. A series of 16 cases by Vosswinkel et al. demonstrated a mortality of 25% (4/16) [3]. In comparison, the mortality of other penetrating aetiologies (stab wounds, gunshot wounds) is 22–62% and 60–90% respectively [25]. The majority of presentations in our review were hemodynamically stable. Those who were unstable were due to pericardial effusion causing tamponade. A few cases describe a delayed presentation, up to 24 h after injury [22], [23]. Bargoud et al. hypothesized that the annular ribbing found on nails provides a nidus for platelet aggregation, especially when a low-pressure chamber such as the right ventricle were affected, effectively tamponading the bleeding [22]. Nonetheless, all cases described were managed operatively.
Patients with penetrating nail-gun injuries to the chest require urgent imaging. Bedside transthoracic echocardiography (TTE) is useful in determining the presence of a pericardial effusion, cardiac tamponade or in rare cases, valvular involvement [17], [19], [25]. Nails can be up to 6 cm long with unclear, trajectories, and can hence involve multiple structures. Assumptions of injury on the basis of surface anatomy can therefore be misleading. A case by Ho et al detailed a single nailgun injury to the 4th intercostal space affecting the right ventricle, left atrium and diaphragm [1]. Consequently, a contrast enhanced CT (CECT) scan can be used to determine the trajectory of the nail and outline the spectrum of injuries [1], [19], [26]. In addition, it will give useful information as to the position of the nail in the patient, aiding in removal [1], [26]. In this case, a CECT scan was useful in determining the position of the nails: one nail was abutting the apex of the left ventricle whereas the second was embedded within the myocardium. As the patient was hemodynamically stable and in a level 1 trauma centre, obtaining a timely CECT scan was tenable. Patients' who have unstable presentations require prompt transfer to the operating theatre. In these instances, there should be no delay in treatment with further CT imaging.
The right ventricle is commonly injured due to its anterior location [3]. This was injured in 12/22 cases. Less commonly, the left ventricle and lung parenchyma are affected. In these instances, a wedge resection was required to remove the damaged segment of lung. Jodati et al details a case whereby the anterior mitral valve leaflet was transfixed, resulting in moderate MR and heart failure [19]. In this instance, a mitral valve repair was performed utilising cardiopulmonary bypass. One case details a nailgun injury to the thoracic aorta, requiring transection of the affected segment and replacement with a tubular graft [24]. In this case, the patient sustained an uncommon injury to the apex of the left ventricle. These injuries can be fraught with added danger, as they may be compounded by coronary artery involvement [21].
Presentations vary from chronic to acute, and from stable to unstable [8], [12], [22], [23]. Some patients have had missed injuries, and present with complications years later [8]. These injuries commonly require operative management. Patients who have unstable presentations to a peripheral centre may be temporized with a pericardial drain or fluid resuscitation, and when in extremis, require an emergency room thoracotomy [12], [14]. Patients who are stable enough require prompt transfer to a centre with cardiothoracic and trauma expertise [12], [14], [27]. In terms of approach, a median sternotomy provides excellent exposure to the heart and mediastinal structures. The pleura may also be opened bilaterally to allow access to the lungs. This approach provided adequate exposure to the myocardial injury in our case. When the second nail was not able to be located within the mediastinum the left pleura was opened and sternum retracted upwards, providing excellent visualization (Fig. 6).
The patient in our case had multiple superficial myocardial breaches caused by a single nail. We opted to repair the defects with Bioglue®, reinforced with a bovine pericardial patch. Cases of transmural injuries were repaired with a prolene® or polypropylene pledgeted sutures [1], [6], [7], [10], [12], [13], [14], [16], [17], [18]. Haemostasis with the use of fibrin sealants and pericardial patches have also been reported in literature [4], [9]. We opted against suture repair due to the bleeding caused by multiple suture holes. Cardiopulmonary bypass may be necessary to repair these injuries and should be initiated immediately if there are anatomical and physiological concerns [6]. Cardiopulmonary bypass may also be unsafe in certain situations due to heparinisation, and this should be considered in the context of the patients' other injuries [7]. In this case, the left ventricle was repaired without the use of CPB however a circuit was primed as a contingency. We used the Medtronic® urchin apical suction device to expose the lateral wall. The use of this device is usually reserved for off pump cardiac surgery, and no cases exist detailing its use in penetrating cardiac trauma. In this instance, it provided excellent exposure to the lateral wall of the heart facilitating repair without causing haemodynamic compromise by lifting of the heart.
Conclusion
This case highlights the management of an uncommon injury. A chest X-ray and TTE should be done to assess for a pneumothorax, haemothorax and/or pericardial effusion. Select patients should get a CECT to assess the trajectory of the nail. The majority of cases are self-inflicted and require urgent surgical management. The use of the Medtronic® urchin apical suction device provided excellent exposure of the lateral wall of the heart, facilitating repair.
The following is the supplementary data related to this article.
Declaration of competing interest
No conflicts of interest or financial obligations to disclose.
References
- 1.Ho S., Liu B., Fernac N. Self-inflicted cardiac injury with nail gun without hemodynamic compromise: a case report. Cureus. 2017;9(1) doi: 10.7759/cureus.971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Beaver A.C., Cheatham M.L. Life-threatening nail gun injuries. Am. Surg. 1999;65:1113–1116. [PubMed] [Google Scholar]
- 3.Vosswinkel J.A., Bilfinger T.V. Cardiac nail gun injuries: lessons learned. J. Trauma. 1999;47:588–590. doi: 10.1097/00005373-199909000-00032. [DOI] [PubMed] [Google Scholar]
- 4.Haghshenas J., et al. Nail gun to the heart—patch repair of penetrating cardiac injury. Am. Surg. 2019;85:E249–E251. [PubMed] [Google Scholar]
- 5.Temple A., Fesmore F., Seaberg D., Severance H. Cardiac injury due to accidental discharge of nail gun. J Emerg. Med. 2013;44(2):E161–E163. doi: 10.1016/j.jemermed.2012.01.054. [DOI] [PubMed] [Google Scholar]
- 6.Hajsadeghi, et al. Role of chest CT scan in atypical cardiac trauma management: left ventricle injury by a nail gun. Radiol. Case Rep. 2021;16:3280–3284. doi: 10.1016/j.radcr.2021.07.068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wang S., Chen M., Yan J., Huang T., Chang C., Chien C. Survival after multiple nail gun injuries to the brain, lung, and heart: a case report and a review of the literature. J. Int. Med. Res. 2021;49(10):1–10. doi: 10.1177/03000605211049923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Albacker T., et al. Penetrating chest injury afflicting coronary artery fistula—a delayed and asymptomatic occurrence. J. Card. Surg. 2021;36:3892–3897. doi: 10.1111/jocs.15775. [DOI] [PubMed] [Google Scholar]
- 9.Straus J., Woods R., McCarthy M., Anstadt M., Kwon N. Cardiac pneumatic nailgun injury. J. Thorac. Cardiovasc. Surg. 2006;132(3):702–703. doi: 10.1016/j.jtcvs.2006.04.030. [DOI] [PubMed] [Google Scholar]
- 10.Tulhadhar S., Eltayeb A., Laskmanan S., Yiu P. Delayed presentation of right and left ventricle perforation due to suicidal nail gun injury. Ann. Card. Anaesth. 2009;12(2):136–138. doi: 10.4103/0971-9784.53448. [DOI] [PubMed] [Google Scholar]
- 11.Hulsman N., Hiddema P., Veen E., Van der Meer N. Traumatic cardiac injury by gun nails. Int. J. Crit. Illness Injury Sci. 2014;4(2):186–187. doi: 10.4103/2229-5151.134190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chirumamilla V., et al. Pericardiocentesis followed by thoracotomy and repair of penetrating cardiac injury caused by nail gun injury to the heart. Int. J. Surg. Case Rep. 2016;23:98–100. doi: 10.1016/j.ijscr.2016.04.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Guo R., Myers L. Penetrating cardiac injury: the nail gun, a potentially dangerous tool. Can. J. Surg. 2008;51(1):E7–E8. [PMC free article] [PubMed] [Google Scholar]
- 14.Catarino P., Halstead J., Westaby S. Attempted nail-gun suicide: fluid management in penetrating cardiac injury. Injury, Int. J. Care Injured. 2000;31:209–211. doi: 10.1016/s0020-1383(99)00282-x. [DOI] [PubMed] [Google Scholar]
- 15.Lim H., Weinberg L., Tan C., Tay S., Kolivas C., Peyton P. Airway strategies for lung isolation in a patient with high-velocity nail gun injuries to the right cardiac ventricle and floor of the mouth: a case report. J. Med. Case Rep. 2013;7:137. doi: 10.1186/1752-1947-7-137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Madani M., et al. Nail gun may cause heart injury: a young adult’s misadventure. Int. Emerg. Nurs. 2012;20:98–101. doi: 10.1016/j.ienj.2011.06.006. [DOI] [PubMed] [Google Scholar]
- 17.Panicker A., Nugent K., Mink J., Glaser J., Bradley K., Siric F., Nomura J. Bedside ultrasonography in the management of penetrating cardiac injury caused by a nailgun. J. Emerg. Med. 2018;56(2):197–200. doi: 10.1016/j.jemermed.2018.09.036. [DOI] [PubMed] [Google Scholar]
- 18.Pritts T., Knight D., Davis B., Porembka D., Cuscheri J. Accidental self-inflicted nail gun injury to the heart. Injury Extra. 2005;36:517–519. [Google Scholar]
- 19.Jodati A., Safaei N., Toufan M., Kazemi B. A unique nail gun injury to the heart with a delayed presentation. Interact. Cardiovasc. Thorac. Surg. 2011;13:363–365. doi: 10.1510/icvts.2011.272120. [DOI] [PubMed] [Google Scholar]
- 20.Eren E., et al. Penetrating injury of the heart by a nail gun. J. Thorac. Cardiovasc. Surg. 2004;127:598. doi: 10.1016/j.jtcvs.2003.09.041. [DOI] [PubMed] [Google Scholar]
- 21.Comoglio C., Sansone F., Boffini M., Ribezzo M., Rinaldi M. Nail gun penetrating injury of the heart mimicking an acute coronary syndrome. Int. J. Emerg. Med. 2010;3:135–137. doi: 10.1007/s12245-009-0152-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bargoud C., et al. Delayed presentation of a pneumatic nail gun injury to the right ventricle without circulatory compromise. Trauma Case Rep. 2022;37 doi: 10.1016/j.tcr.2021.100597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Thakur S., Lee M., Cullen H. Patient who was unaware of nail gun injury to his heart. ANZ J. Surg. 2021;91(6):E423–E424. doi: 10.1111/ans.16516. [DOI] [PubMed] [Google Scholar]
- 24.Yamamoto A et al Penetrating nail-gun injury of the thoracic descending aorta. [DOI] [PMC free article] [PubMed]
- 25.Attar S., Suter C., Hankins J.R., et al. Penetrating cardiac injuries. Ann. Thorac. Surg. 1991;51:711–716. doi: 10.1016/0003-4975(91)90110-c. [DOI] [PubMed] [Google Scholar]
- 26.Co S., et al. Role of imaging in penetrating and blunt traumatic injury to the heart. Radiographics. 2011 doi: 10.1148/rg.314095177. [DOI] [PubMed] [Google Scholar]
- 27.Tahalele P.L., Puruhito P.A., et al. Penetrating cardiac injury. J. Cardiothorac. Surg. 2013;8:P41. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.