
FIGURE 2.
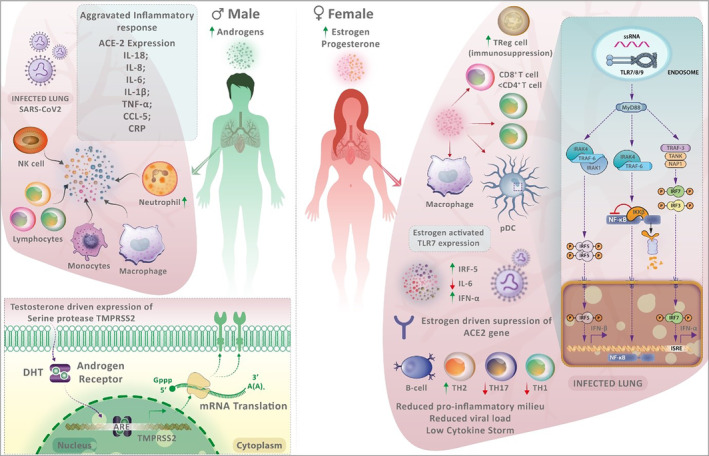
The sex differences in the immune response to severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) infection. Males have more testosterone and dihydrotestosterone, whilst females have higher oestrogen and progesterone levels. Men experience aggravated immune responses to SARS‐CoV‐2 infection due to various factors. The expression of transmembrane serine protease 2 (TMPRSS2), which facilitates viral entry, is regulated by androgen receptors and higher in males. Males with coronavirus disease 2019 (COVID‐19) have higher neutrophil‐to‐lymphocyte ratios, lower lymphocyte count and greater serum C‐reactive protein levels. Older males have decreased naïve T and B cells. Males experience hyperinflammation and cytokine storms, which translate into increased COVID‐19 severity. In females, SARS‐CoV‐2 infection is better controlled due to the efficient sensing of the viral genome by endosomally expressed TLR7 in immune cells. TLR7 expression is enhanced by higher levels of oestrogen in females. Such intracellular detection of the viral genome in immune cells amplifies the production of type I interferon (IFN), which confers antiviral immunity. In plasmacytoid dendritic cells of females, IRF5 expression is higher, which may explain the greater production of type I IFN in females. Additionally, oestradiol promotes regulatory T cells, and women also have increased CD4+:CD8+ T‐cell ratios, which may have an impact on COVID‐19 progression. Females exhibit more robust adaptive immunity compared with males, with pronounced effects on reducing dysregulated inflammation.