

Abstract
Objective.
Salivary glands are among the most sensitive target organs of medications with anticholinergic (AC) properties, interrupting the neural stimulation of saliva secretion and reducing saliva flow. Hyposalivation results in dry mouth, leading to dental caries, intraoral infection, orofacial pain, problems with speaking and swallowing, and diminished oral health–related quality of life. Current understanding of the pharmacokinetics of AC medications and their effect on muscarinic receptors in the salivary glands were reviewed to assist clinicians in predicting salivary damage in patients with AC medication–induced dry mouth.
Study Design.
We summarized the literature related to the mechanisms and properties of AC medications, anticholinergic adverse effects, and their effect on salivary function and management strategies to prevent oral health damage.
Results.
Although a large number of studies reported on the frequencies of medication-induced dry mouth, we found very limited data on predicting individual susceptibility to AC medication–caused hyposalivation and no prospective clinical studies addressing this issue.
Conclusion.
Dry mouth is most frequently caused by medications with AC properties, which interrupt the neural stimulation of saliva secretion. Interdisciplinary care should guide pharmacotherapeutics and dental interventions should aim in preventing AC salivary adverse effects and reducing the oral health burden from AC medication–induced dry mouth.
Anticholinergic (AC) toxicity syndrome1 with cognitive impairment and delirium2 recently gained increased attention as a harmful adverse reaction of AC medications.3 A considerably less studied issue, the most frequent AC adverse effect is decreased saliva secretion (hyposalivation), resulting in dry mouth, from over 600 medications that possess AC properties.4 Salivary variables are sensitive indicators of systemic health5 and are indeed commonly affected by medications, but only 2 recent publications offered insights into salivary secretion rates in relation to the AC burden of medications.6 Accordingly, the overall load of AC drugs showed a statistically significant association with lower saliva flow rates, which was further lowered by increased medication intake and polypharmacy (using 5 or more medications). Polypharmacy has risen by 70% during the past decade7; it affects 1 in 5 patients in the United States8 and is widespread in treating chronic diseases in patients of all ages. AC drugs are used to successfully treat conditions such as depression, psychological entities, urinary incontinence, gastroesophageal reflux, peptic ulcer disease, cardiovascular diseases, muscle spasm, neuropathic pain, irritable bowel syndrome, obstructive pulmonary disease, allergy, Parkinson disease, and epilepsy.9
Because decreased saliva flow rates are more prevalent among older adults, dry mouth and its destructive effects on oral health are almost exclusively described in the context of older adults.10,11 Prolonged AC exposure from medications has been linked to increased dementia incidence and irreversible cognitive decline in frail, older people,12 as confirmed by a recent large case-control study including 284,000 individuals.13 However, long-term exposures to AC medications and their combinations have also increased in younger age groups. The pharmacologic management of various common chronic conditions and diseases8,14 is frequently based on drugs with AC properties. Combination therapy with AC medications adds up to a cumulative AC effect with the prominent risk for adverse effects irrespective of age.15
The autonomic nervous system16 controls salivary secretion from the 3 major salivary glands (parotid, submandibular, and sublingual glands) and hundreds of minor salivary glands. Acetylcholine release from postganglionic neurons in the parasympathetic (or cholinergic) system binding to muscarinic receptors on salivary glands is the dominant stimulus for saliva fluid secretion and can be compromised by a large number of medications17 with the potential to block (antagonize) these receptors. Emerging scientific evidence18,19 supports a strong association between impaired salivary function and the intake of medications possessing properties that can antagonize acetylcholine transmission (i. e., AC effect). AC medications affect the oral health20 because of the ancillary impairment of salivary function such as hyposalivation (reduction in saliva secretion), resulting in dry mouth and/or xerostomia (the subjective sensation of oral dryness). Dry mouth is a known risk factor for dental caries21,22 and other maladies in the oral cavity.23 It has mostly been studied in older age groups because of the higher medication exposure in the geriatric population.24
The purpose of this review is to provide an evidence-based synopsis of the current knowledge and pharmacologic concepts of medications with AC properties and their effect on salivary function. We compiled a scientific synthesis of pertinent dental implications and summarized the most potent and often prescribed AC drugs because the oral health aspects of this significant problem have been understudied. We created a muscarinic receptor “map” of salivary functional units and a detailed figure of muscarinic receptors in the major and minor salivary glands. The tables provide a novel aspect of relevant data corresponding to clinical scenarios for patient care and based on pharmacologic and geriatric expert opinion as a reference for managing dry mouth.
PHARMACOLOGY OF ANTICHOLINERGIC MEDICATIONS
The most frequently prescribed medications with AC properties and their therapeutic indications are shown in Table I. A large group of medications (tricyclic antidepressants, antipsychotics, etc.) exerts unwanted or side effects owing to their nonselective antagonism of cholinergic (also known as muscarinic) receptors. In the central nervous system, acetylcholine modulates cognitive function and motor control.2,25 In the peripheral cholinergic nervous system, the most sensitive receptors to AC drugs can be found in the salivary, bronchial, and sweat glands.19 The adverse effects of AC drugs in the human body depend on the organ- or tissue-specific cholinergic innervation and the cholinergic receptor expression pattern.26 The muscarinic (M) receptors are classified into 5 subtypes: M1, M3, M5 excitatory and M2, M4 inhibitory receptors. The functional variety of these muscarinic receptors is based on structural differences and intracellular signal transmission pathways.27 The spatial distribution of muscarinic receptor subtypes is characteristic to specific tissues and organs; M1 receptors are more abundant in the central nervous system28; M2 receptors are more frequent in the heart, colon, and urinary bladder29; M3 receptors have a dominant role in the salivary glands,30,31 urinary bladder, and respiratory tract innervation; M4 receptors are expressed mainly in the basal ganglia in the brain; and M5 receptors are scattered throughout the central nervous system.28
Table I.
Conditions and diseases that are frequently treated by medications with anticholinergic properties
| Clinical conditions often treated with anticholinergic medications |
|---|
| Psychiatric conditions |
| Schizophrenia, schizoaffective disorder |
| Bipolar disorder |
| Depression |
| Obsessive-compulsive disorder |
| Anxiety |
| Insomnia |
| Neurologic conditions |
| Parkinson disease |
| Epilepsy |
| Somatic problems |
| Urinary incontinence |
| Gastroesophageal reflux, peptic ulcer disease |
| Cardiovascular diseases |
| Muscle spasm |
| Low back pain |
| Neuropathic pain |
| Irritable bowel syndrome |
| Obstructive pulmonary disease |
| Allergy |
The therapeutic and side effects of systemic AC drugs depend on the distribution of various muscarinic receptors in the target tissues; therefore, tissues expressing the same receptor subtypes might be similarly affected. In Figure 1, we provide an updated overview of organs and tissues in the human body containing M3 receptors, the predominant muscarinic receptor in the salivary glands. Additionally, we provide an illustration of the distribution of all muscarinic receptor subtypes in the 3 majors as well as minor salivary glands in Figure 1, based on currently available and published research results. The peripheral parasympathetic signals from the salivary nuclei to the salivary glands are principally mediated through the efferent fibers of chorda tympani lingual nerve (CN VII) toward the submandibular and sublingual glands. The parotid gland is supplied through the glossopharyngeal (CN IX), auriculotemporal (CN V), and facial (CN VII) nerves. The minor salivary glands receive parasympathetic nerve fibers from the mandibular (CN V), lingual (CN V), and palatine (CN V) nerves.
Fig. 1.
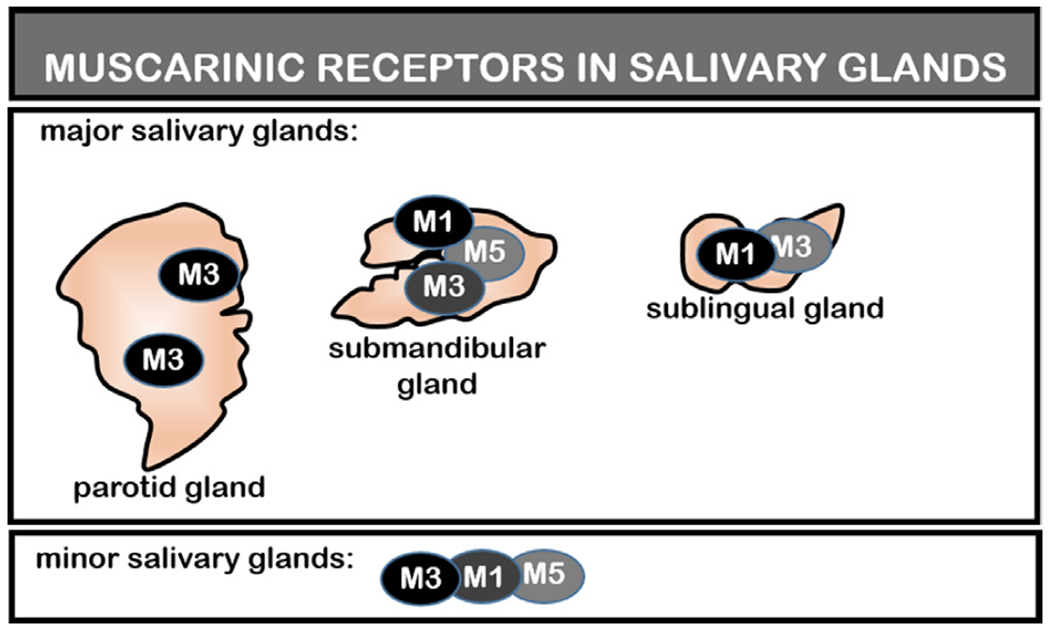
Salivary flow secretion principally mediated through muscarinic type 3 receptors. The heterogeneity of muscarinic receptors and their specific localization in the major and minor salivary glands, as well as other muscarinic type 3 receptor–mediated organs, were mostly established in animal studies. M1, muscarinic type 1 receptor; M3, muscarinic type 3 receptor; M5, muscarinic type 5 receptor.
To reduce the unwanted side effects of anticholinergic drugs, a unique pharmaco-physiologic approach (the concept of tissue selectivity32) was developed, which is based on the histologic and functional variation of the muscarinic receptor subtypes. Accordingly, organ-selective anticholinergic drugs with high affinity to a specific muscarinic receptor subtype achieve a selective therapeutic blockade of those muscarinic receptors within a particular organ.33 New selective antimuscarinic agents targeting organs such as the bladder rather than the the salivary glands demonstrated a lower risk for dry mouth.34
Multiple tools to estimate the AC toxicity of a patient’s medications have been developed and can be used to calculate each individual’s AC burden (e.g., Beers criteria,35 Rudolph risk scale,36 AC drug scale; Anticholinergic Drug Scale [ADS]37). The AC burden has been used to estimate the risk of dementia and mortality in older adults.38 Few dental studies6,39 have investigated the salivary secretion in relation to the AC burden14 and established a positive correlation between AC burden (measured by ADS) and dry mouth.40,41 The ADS, compiled by Carnahan et al.37 and Duran et al.,42 includes over 100 commonly prescribed muscarinic receptor antagonists27 according to their anti-muscarinic activity on muscarinic receptors.
EFFECT OF ANTICHOLINERGIC MEDICATIONS ON SALIVARY GLANDS
As discussed above, the current view on the mechanism of AC medication–induced dry mouth is that salivary function is either directly inhibited by AC drugs that block acetylcholine binding to muscarinic receptors in the salivary glands or indirectly inhibited by the AC drug effects in the central nervous system. Blocking the muscarinic receptors has been considered the mechanism responsible.43 Although mechanistic studies in humans were not conducted, an in vivo study44 suggested that muscarinic receptor antagonists cause detectable histologic and ultrastructural changes in rat salivary glands leading to the glandular tissue atrophy. Figure 2 illustrates the theoretical fine-tuned interaction between the stimulatory M1, M3 muscarinic receptors in salivary acinar cells and the inhibitory/modulatory M2, M4 receptors in postganglionic, presynaptic parasympathetic neurons, evoking the normal secretory responses45 of salivary glands as animal studies have confirmed. It should be noted that salivary glands also receive potentiating stimulation from non-cholinergic sources, such as neuropeptides, that are colocalized with acetylcholine and released from the glandular nerves.46
Fig. 2.
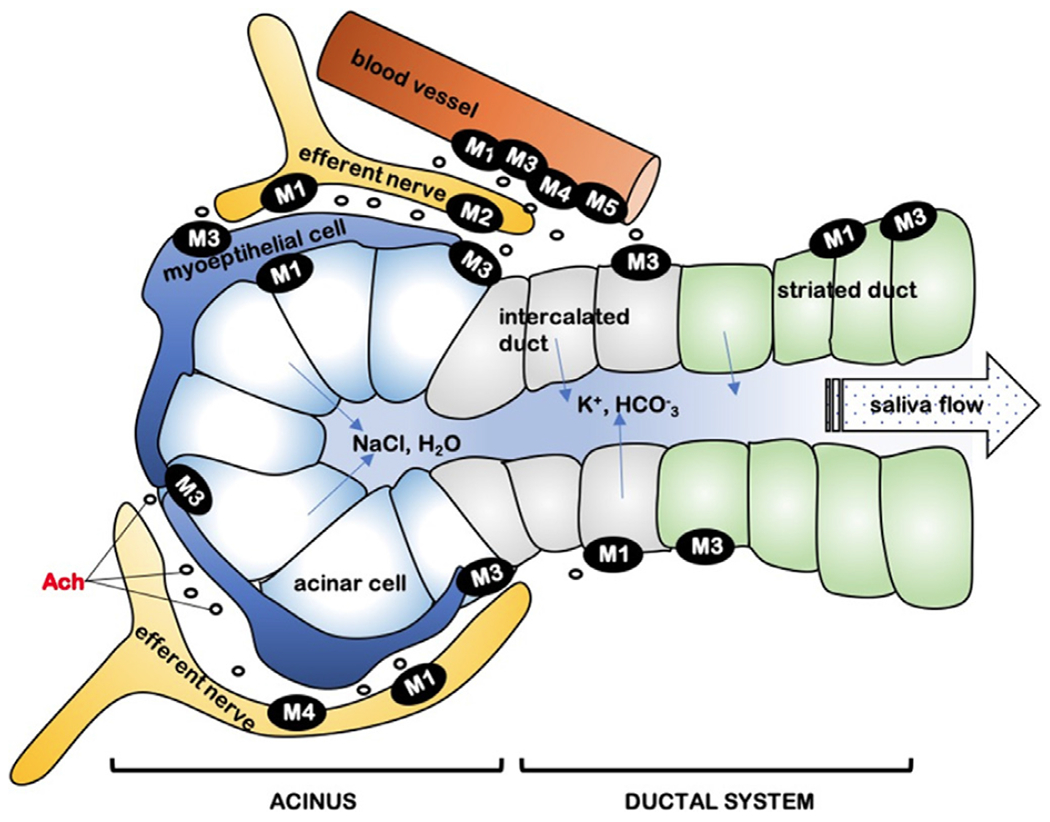
Localization of the muscarinic receptor subtypes in the salivary glands.81–83 The schematic drawing depicts a secretory unit (secretory, aka acinar cells connected to the ductal compartment) of salivary glands, surrounded by efferent nerves, contractible myoepithelial cells, and blood vessels. The secretory activity is regulated by the peripheral parasympathetic (CN VII and IX) and sympathetic (T1-T3) nerves through muscarinic prejunctional (M1, facilitatory; M2 or M4, inhibitory) effects on the secretory unit cells. The neurotransmitter acetylcholine is released into the synaptic cleft and responsible for signal transmission through the muscarinic receptors, and the mixture of mostly M3 and M1 receptors mediates cholinergic salivary signaling.30 Acetylcholine released from parasympathetic nerve endings binds to acinar M3 and M1 receptors (G protein–coupled receptors), which activates the intracellular coupling mechanisms for salivary fluid and protein secretion. The intracellular increase of calcium concentration from endoplasmic reticulum stores triggers the transmembrane sodium-potassium pumps, which create an osmotic gradient to secrete fluid into the ductal system. Parasympathetic signals may also activate protein exocytosis from acinar cells by a vasoactive intestinal peptide–coupled intracellular cyclic adenosine monophosphate generation pathway or a cyclic adenosine monophosphate–independent pathway. M1, muscarinic type 1 receptor; M2, muscarinic type 2 receptor; M3, muscarinic type 3 receptor; M4, muscarinic type 4 receptor; M5, muscarinic type 5 receptor.
AC medications may also affect the function of minor salivary glands.47 Hundreds of these minor salivary glands secrete saliva continuously into the oral cavity, and their flow rates are not in response to salivary stimuli. Though the secretion of minor salivary glands comprises only 7% to 10% of the whole saliva, it is driven under an exclusive parasympathetic influence and cholinergic transmission; thus, the secretion rates may be directly affected by AC drugs. However, most of the existing published evidence related to medication-induced dry mouth is based on studying the 3 major salivary glands, with very little information regarding the effects of AC medications on minor salivary glands.48,49
AC DRUGS MOST RELEVANT TO ORAL HEALTH
The most commonly reported adverse side effect associated with AC drugs is dry mouth (frequencies range between 16% and 30%), which has been confirmed by randomized clinical trials50–52 and a worldwide doubleblind placebo-controlled trial performed at 167 centers (patients were enrolled in Australia, Europe, and North America).53 Furthermore, a recent meta-analysis54 of 26 studies calculated a high risk of dry mouth from AC psycholeptics and bladder antimuscarinics. A large computational model55 of 578,228 individuals established a significant correlation between AC toxicity and incidence rates of the most common adverse effects, including dry mouth. Considering probable relevant clinical scenarios and various medications that patients are taking, the most common drugs with known AC effects are presented in Table II, including information on each drug’s antimuscarinic potency representing the binding affinity to block muscarinic receptors. The lower the inhibitory constant (Ki), the greater the blocking of the predominant M3 receptors in the salivary glands. For example, the tricyclic antidepressant amitriptyline (Ki = 25.9) is significantly more potent at blocking muscarinic receptors compared with the antidepressant trazodone (Ki = 324,000). However, because Ki values are generally calculated from experiments in vitro, they may not explicitly predict dry mouth. Therefore, risk ratios calculated in various human clinical studies for dry mouth may reflect higher risk than expected solely based on Ki values. Table II summarizes Ki values of various AC drugs and risk ratios from published data. These data may be useful in clinical practice for evaluating known AC medications causing dry mouth. The patient’s medication list reflecting comorbidities and ongoing treatments allows anticipation of dry mouth–triggered dental and oral health problems. Recognizing a medication with high risk for dry mouth and substituting (when medically possible) with a less potent AC drug is a favorable approach.
Table II.
Commonly prescribed anticholinergic drugs associated with dry mouth
| Medication (frequency of usage) | Xerostomia risk | Muscarinic receptor antagonism (Ki)* |
|---|---|---|
| Selective serotonin reuptake inhibitors (22%) | ||
| Paroxetine | 1.98 | 72.0 |
| Escitalopram | 2.19 | 1240.0 |
| Sertraline | 1.48 | 1300.0 |
| Fluoxetine | 1.64 | 2000.0 |
| Citalopram | 2.01 | 2200.0 |
| Serotonin-norepinephrine reuptake inhibitors (11%) | ||
| Duloxetine | 6.02 | 3000.0 |
| Venlafaxine | 2.67 | >10,000.0 |
| Antidepressant agents (50%) | ||
| Mirtazapine | 1.42 | 800.0 |
| Vilazodone | 1.50 | 28,000.0 |
| Bupropion | 2.00 | 48,000.0 |
| Trazodone | 1.51 | 324,000.0 |
| Tricyclic antidepressants (27%) | ||
| Dothiepin | 25.0 | |
| Amitriptyline | 3.28 | 25.9 |
| Nortriptyline | 50.0 | |
| Doxepin | 2.91 | 52.0 |
| Imipramine | 3.81 | 102.0 |
| Antipsychotics | ||
| Olanzapine | 13.0 | |
| Chlorpromazine | 4.00 | 67.0 |
| Quetiapine | 2.42 | 1320.0 |
| Risperidone | >10,000.0 | |
| Overactive bladder medications (30%) | ||
| Trospium | 0.8 | |
| Darifenacin | 7.41 | 0.8 |
| Tolterodine | 4.82 | 3.4 |
| Oxybutynin | 18.85 | 11.2 |
| Fesoterodine | 6.94 | 26.9 |
| Solifenacin | 5.34 | 64.3 |
| Asthma (20%) | ||
| Tiotropium | 0.2 | |
| Ipratropium | 0.5 | |
| Muscle control | ||
| Biperiden | 3.9 | |
| Cyclobenzaprine | 6.0 | |
Medications are reported by indication and frequency and further ranked by their muscarinic anticholinergic potency: Lower values of Ki denote higher potency. Available xerostomia risk is reported by relative risk ratio. (Relative risk ratio based on published data35,44,46,65–67; Ki extracted from the Psychoactive Drug Screening Program database.)
Ki, muscarinic receptor inhibitor constant.
IMPLICATIONS FOR DENTAL PRACTITIONERS
Many individuals in all age groups in the United States are affected by the side effects of AC drugs. Early recognition of dry mouth, as 1 of the most frequent side effects of AC medication use, is best achieved by dental providers. Commonly accepted confounding factors, such as age and sex, may modify the symptoms of dry mouth and xerostomia. The symptoms may worsen with age because decreased saliva flow is more prevalent among patients of older ages10 owing to polypharmacy (taking multiple medications)24 and age-related changes in salivary function.18 Although salivary secretion in healthy aging individuals has been found intact with stable saliva flow, age-related dehydration and diminishing biting force may also result in hyposalivation. Moreover, systemic conditions, diseases, and medication-induced salivary changes contribute to a more prevalent oral dryness among geriatric patients.56 A logistic regression analysis established a correspondence in the increase of xerostomia prevalence by the odds ratio of 1.24 per decade of age.57 In contrast, other investigations20,58–61 could not verify the effect of aging on salivary function and found that secretion rates in healthy individuals were not age dependent. As emphasized by Ship et al.56 healthy aging does not tend to present salivary flow concerns and presumably dry mouth is secondary to medical conditions and medications.
Additionally, the female sex is associated with a higher total number of medications, a higher risk of AC exposure, reduced saliva secretion, and oral dryness.62
Long-term AC drug exposure3,63 has been associated with the increased prevalence of AC side effects in patients with defective genetic variants of certain cytochrome P450 enzymes64 in the liver, responsible for the metabolic clearance of these drugs. A pioneer study65 examining the association between the genetic polymorphism of cytochrome P450 enzymes and xerostomia in older adults measured a significant difference in the level of serum AC activity between metabolizing phenotypes. Although genetic variations of various drug-metabolizing enzymes are responsible for an increased prevalence of AC adverse events in patients are well documented, pharmacogenetics is not considered currently in the management of xerogenic medication–induced dry mouth.
Our suggested management of patients taking high-risk AC drugs is based on 3 pillars, including a comprehensive dental evaluation with salivary assessment, a multidisciplinary pharmacologic review and optimization,18 and frequent reassessment of overall oral health, salivary function, and management success, as detailed in Table III. Patients presenting at the dental office with medication-induced dry mouth might have chewing or swallowing problems, speaking difficulties, intraoral mucosal lesions, increased rate of dental caries, tooth loss,21 and orofacial pain due to reduced saliva flow. The executive summary of evidence-based clinical recommendations of the American Dental Association identified medication-induced dry mouth as a significant risk factor for dental caries.66 Dental caries status has been previously associated with dry mouth.20,21,23,67 Salivary gland hypofunction based on parameters such as the decayed, missing, and filled teeth indices was recommended to identify patients with high risk for dry mouth,68 because the risk for dry mouth is associated with a lower number of remaining natural teeth.69 Root caries is significantly associated with lower salivary flow rates23,70 even from the minor salivary gland.48,71 Furthermore, a recent retrospective study72 conducted by the Department of Veterans Affairs investigated 95,850 dentate patients and found an 8% increase in the rate of dental caries–-related treatment in individuals taking at least 1 drug with strong AC activity. Dry mouth increases susceptibility to bacterial colonization or inflammation in the oral cavity as well as infections in the upper respiratory tract, which further impairs patients’ quality of life.70 Affected patients should receive intensive preventive care, including oral hygiene instruction, dietary advice, and regular topical fluoride treatments.
Table III.
Evaluation and management of dry mouth based on the multidisciplinary approach
| Dental Evaluation/Dry Mouth Assessment | • Comprehensive Dental Evaluation/Dry Mouth Assessment • Measurement of Salivary Gland Flow Rate/Xerostomia • Oral Health Assessment |
| Multidisciplinary Medication Assessment and Management | • Refer to Primary Care Physician/Other Medical Specialists/Clinical Pharmacologist • Management of Associated Systemic Diseases to Reduce Vulnerability (Comorbidities and Polypharmacy • Discontinue/Reduce Dose or Frequency/Higher Ki or Substitute Non-anticholinergic Medications |
| Dental Management | • Frequent Dental Examinations • Reassessment of Salivary Function • Reassessment of Risk Category and Preventive Regimen • Palliative Recommendations as Necessary |
Ki, muscarinic receptor inhibitor constant.
Measurable clinical features can support identifying patients with dry mouth who are taking AC drugs at the dental office. Assessing saliva secretion is a feasible tool to screen patients with a suspected AC medication–induced dry mouth at their regular dental visit. Clinical signs of reduced saliva secretion status can be confirmed by quantifying the resting saliva flow rate,73 which has been validated by randomized control studies to determine hyposalivation (saliva flow rate <0.1 mL/min). Xerostomia questionnaires are reliable evidence-based tools for the subjective perception of oral dryness,67,74 because the feeling of mouth dryness is correlated to the amount of resting (unstimulated) saliva.75 Xerostomia sensation generally occurs when saliva volume decreases to half or more of the normal secretion levels.76 However, the perceived oral dryness of a patient is not always reflected by reduced saliva flow.
Dental practitioners should promote medication management by working with patients’ medical providers to reduce the number of AC medications, adjusting their dosage, and possibly replacing them with medications with fewer AC side effects. As dentistry is integrated into systemic health care, informed decisions regarding AC toxicity are among the responsibilities of dental providers to advocate for reducing oral health complications. Concern for hyposalivation should be evaluated based on individual patient risk-benefit assessments, and that concern should be discussed with patients’ physicians. An up-to-date medication list and the revision of pharmaco-medical history at dental visits may prevent AC medication–related morbidity among affected patients. Collaborating with the prescribing physicians is the most suitable action plan to address drug-induced dry mouth issues. Based on limited clinical studies, alternative pharmacotherapeutics with less salivary antagonism can alleviate the severity of the AC adverse effect on salivary function.39,77 Tailored interventions such as choosing AC medications for patients with lower binding affinity to salivary muscarinic receptors may reduce oral health problems.
Identifying individuals taking known high-risk AC drugs often necessitates personalized pharmacotherapy choices to complement the accepted standards of xerostomia treatment based on a multidisciplinary approach between dental and other medical professionals. Interactions among AC medications52,78 are known modifiers of adverse effects, and the endogenous AC activity from stress,79 inflammatory processes,13 and comorbidities80 should be considered as well. Considerations for special needs populations should include renal or hepatic impairment, which modifies AC medications’ bioavailability and clearance. Counseling patients about the side effects of AC medications is essential, because without aggressive preventive actions, dry mouth–related changes in oral and systemic health will become permanent. Currently available symptomatic management or salivary substitutes are not effective in preventing or reversing the damage but only alleviate the complaints. Clinical investigations of AC medication–induced hyposalivation and AC burden are needed to compare preventive strategies and support salivary function. New evidence-based guidelines for tailored preventive measures to control AC medication–induced dry mouth and salivary damage are required for all patients regardless of age. Studies should address whether novel pharmacogenetic assays can be employed in predicting poor metabolizing profiles of patients and potentially severe xerostomia cases.
CONCLUSION
The exposure to AC medications has increased significantly among adults of all ages. The most sensitive parasympathetic receptor organs to AC drugs are the salivary glands and the most commonly reported peripheral adverse effect of AC drugs is dry mouth. Medication-induced dry mouth can have a devastating effect on the oral health status of patients, and such patients should receive intensive preventive care, including the assessment of reduced saliva secretion, oral dryness, caries status, comorbidities, and pharmacologic interactions. Accordingly, the management of AC medication–induced dry mouth should involve discussion with patients’ other health care providers. Recognizing and avoiding high-risk anticholinergics can aid dental care of the affected patients, because no standard test is available for predicting AC susceptibility. Identification and management of AC medication–induced dry mouth is not possible without understanding and clarifying the underlying mechanisms. The molecular pathway behind the notable sensitivity of the salivary glands to AC medications is largely unexplored. The lack of available clinical research on AC drug–induced salivary effects calls for future clinical studies to explore this existing knowledge gap.
Statement of Clinical Relevance.
The article provides an evidence-based background of the current pharmacological trends of anticholinergic drug use, which increases the risk for anticholinergic toxicity. We compiled a scientific synthesis of dental implications and created figures with direct relevance for patient care.
FUNDING
This study was sponsored by the Finger Lakes Geriatric Education Center, funded by the Health Resources and Service Administration (HRSA), Department of Health and Human Services (DHHS) under the Geriatric Workforce Enhancement Program #U1QHP28738.
REFERENCES
- 1.Collamati A, Martone AM, Poscia A, et al. Anticholinergic drugs and negative outcomes in the older population: from biological plausibility to clinical evidence. Aging Clin Exp Res. 2016;28:25–35. [DOI] [PubMed] [Google Scholar]
- 2.Nebes RD, Pollock BG, Halligan EM, Kirshner MA, Houck PR. Serum anticholinergic activity and motor performance in elderly persons. J Gerontol A Biol Sci Med Sci. 2007;62:83–85. [DOI] [PubMed] [Google Scholar]
- 3.Salahudeen MS, Duffull SB, Nishtala PS. Anticholinergic burden quantified by anticholinergic risk scales and adverse outcomes in older people: a systematic review. BMC Geriatr. 2015;15:31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tollefson GD, Montague-Clouse J, Lancaster SP. The relationship of serum anticholinergic activity to mental status performance in an elderly nursing home population. J Neuropsychiatry Clin Neurosci. 1991;3:314–319. [DOI] [PubMed] [Google Scholar]
- 5.Giannobile WV, McDevitt JT, Niedbala RS, Malamud D. Translational and clinical applications of salivary diagnostics. Adv Dent Res. 2011;23:375–380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tiisanoja A, Syrjala AM, Komulainen K, et al. Anticholinergic burden and dry mouth among Finnish, community-dwelling older adults. Gerodontology. 2018;35:3–10. [DOI] [PubMed] [Google Scholar]
- 7.Gu QD, Dillon CF;, Burt VL. Prescription drug use continues to increase: U.S. prescription drug data for 2007-2008. NCHS Data Brief. 2010:(42):1–8. [PubMed] [Google Scholar]
- 8.Kantor ED, Rehm CD, Du M, White E, Giovannucci EL. Trends in dietary supplement use among U.S. adults from 1999-2012. JAMA. 2016;316:1464–1474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lopez-Alvarez J, Sevilla-Llewellyn-Jones J, Aguera-Ortiz L. Anticholinergic drugs in geriatric psychopharmacology. Front Neurosci. 2019;13:1309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Thomson WM. Dry mouth and older people. Aust Dent J. 2015;60(1):54–63. Suppl. [DOI] [PubMed] [Google Scholar]
- 11.Wolff A, Zuk-Paz L, Kaplan I. Major salivary gland output differs between users and non-users of specific medication categories. Gerodontology. 2008;25:210–216. [DOI] [PubMed] [Google Scholar]
- 12.Dawson AH, Buckley NA. Pharmacological management of anticholinergic delirium—theory, evidence and practice. Br J Clin Pharmacol. 2016;81:516–524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Coupland CAC, Hill T, Dening T, Morriss R, Moore M, Hippisley-Cox J. Anticholinergic drug exposure and the risk of dementia: a nested case-control study. JAMA Intern Med. 2019;179:1084–1093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tiisanoja A, Syrjala AH, Kullaa A, Ylostalo P. Anticholinergic burden and dry mouth in middle-aged people. JDR Clin Trans Res. 2020;5:62–70. [DOI] [PubMed] [Google Scholar]
- 15.Field TS, Gurwitz JH, Avorn J, et al. Risk factors for adverse drug events among nursing home residents. Arch Intern Med. 2001;161:1629–1634. [DOI] [PubMed] [Google Scholar]
- 16.Proctor GB, Carpenter GH. Salivary secretion: mechanism and neural regulation. Monogr Oral Sci. 2014;24:14–29. [DOI] [PubMed] [Google Scholar]
- 17.Villa A, Wolff A, Narayana N, et al. World Workshop on Oral Medicine VI: a systematic review of medication-induced salivary gland dysfunction. Oral Dis. 2016;22:365–382. [DOI] [PubMed] [Google Scholar]
- 18.Barbe AG. Medication-induced xerostomia and hyposalivation in the elderly: culprits, complications, and management. Drugs Aging. 2018;35:877–885. [DOI] [PubMed] [Google Scholar]
- 19.Bostock C, McDonald C. Antimuscarinics in older people: dry mouth and beyond. Dent Update. 2016;43:186–188. 191. [DOI] [PubMed] [Google Scholar]
- 20.Thomson WM, Lawrence HP, Broadbent JM, Poulton R. The impact of xerostomia on oral-health-related quality of life among younger adults. Health Qual Life Outcomes. 2006;4:86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lexomboon D, Tan EC, Hoijer J, et al. The effect of xerostomic medication on oral health in persons with dementia. J Am Med Dir Assoc. 2018;19(1080-1085):e1082. [DOI] [PubMed] [Google Scholar]
- 22.Hu KF, Chou YH, Wen YH, et al. Antipsychotic medications and dental caries in newly diagnosed schizophrenia: a nationwide cohort study. Psychiatry Res. 2016;245:45–50. [DOI] [PubMed] [Google Scholar]
- 23.Bardow A, Nyvad B, Nauntofte B. Relationships between medication intake, complaints of dry mouth, salivary flow rate and composition, and the rate of tooth demineralization in situ. Arch Oral Biol. 2001;46:413–423. [DOI] [PubMed] [Google Scholar]
- 24.Smidt D, Torpet LA, Nauntofte B, Heegaard KM, Pedersen AM. Associations between oral and ocular dryness, labial and whole salivary flow rates, systemic diseases and medications in a sample of older people. Community Dent Oral Epidemiol. 2011;39:276–288. [DOI] [PubMed] [Google Scholar]
- 25.Richardson K, Fox C, Maidment I, et al. Anticholinergic drugs and risk of dementia: case-control study. BMJ. 2018;361:k1315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tobin G, Giglio D, Lundgren O. Muscarinic receptor subtypes in the alimentary tract. J Physiol Pharmacol. 2009;60:3–21. [PubMed] [Google Scholar]
- 27.Soukup O, Winder M, Killi UK, et al. Acetylcholinesterase inhibitors and drugs acting on muscarinic receptors—potential crosstalk of cholinergic mechanisms during pharmacological treatment. Curr Neuropharmacol. 2017;15:637–653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Scarr E Muscarinic receptors: their roles in disorders of the central nervous system and potential as therapeutic targets. CNS Neurosci Ther. 2012;18:369–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mansfield KJ, Liu L, Mitchelson FJ, Moore KH, Millard RJ, Burcher E. Muscarinic receptor subtypes in human bladder detrusor and mucosa, studied by radioligand binding and quantitative competitive RT-PCR: changes in ageing. Br J Pharmacol. 2005;144:1089–1099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gautam D, Heard TS, Cui Y, Miller G, Bloodworth L, Wess J. Cholinergic stimulation of salivary secretion studied with M1 and M3 muscarinic receptor single- and double-knockout mice. Mol Pharmacol. 2004;66:260–267. [DOI] [PubMed] [Google Scholar]
- 31.Culp DJ, Luo W, Richardson LA, Watson GE, Latchney LR. Both M1 and M3 receptors regulate exocrine secretion by mucous acini. Am J Physiol. 1996;271:C1963–C1972. [DOI] [PubMed] [Google Scholar]
- 32.Andersson KE. Advances in the pharmacological control of the bladder. Exp Physiol. 1999;84:195–213. [DOI] [PubMed] [Google Scholar]
- 33.Nelson CP, Gupta P, Napier CM, Nahorski SR, Challiss RA. Functional selectivity of muscarinic receptor antagonists for inhibition of M3-mediated phosphoinositide responses in guinea pig urinary bladder and submandibular salivary gland. J Pharmacol Exp Ther. 2004;310:1255–1265. [DOI] [PubMed] [Google Scholar]
- 34.Yamada S, Kuraoka S, Ito Y, Kato Y, Onoue S. Muscarinic receptor binding of fesoterodine, 5-hydroxymethyl tolterodine, and tolterodine in rat tissues after the oral, intravenous, or intravesical administration. J Pharmacol Sci. 2019;140:73–78. [DOI] [PubMed] [Google Scholar]
- 35.Panel By the American Geriatrics Society Beers Criteria Update Expert. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63:2227–2246. [DOI] [PubMed] [Google Scholar]
- 36.Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168:508–513. [DOI] [PubMed] [Google Scholar]
- 37.Carnahan RM, Lund BC, Perry PJ, Pollock BG, Culp KR. The Anticholinergic Drug Scale as a measure of drug-related anticholinergic burden: associations with serum anticholinergic activity. J Clin Pharmacol. 2006;46:1481–1486. [DOI] [PubMed] [Google Scholar]
- 38.Hilmer SN, Mager DE, Simonsick EM, et al. Drug burden index score and functional decline in older people. Am J Med. 2009;122:1142–1149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kersten H, Molden E, Willumsen T, Engedal K, Bruun Wyller T. Higher anticholinergic drug scale (ADS) scores are associated with peripheral but not cognitive markers of cholinergic blockade. Cross sectional data from 21 Norwegian nursing homes. Br J Clin Pharmacol. 2013;75:842–849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ness J, Hoth A, Barnett MJ, Shorr RI, Kaboli PJ. Anticholinergic medications in community-dwelling older veterans: prevalence of anticholinergic symptoms, symptom burden, and adverse drug events. Am J Geriatr Pharmacother. 2006;4:42–51. [DOI] [PubMed] [Google Scholar]
- 41.Tiisanoja A, Syrjala AM, Anttonen V, Ylostalo P. Anticholinergic burden, oral hygiene practices, and oral hygiene status—cross-sectional findings from the Northern Finland Birth Cohort 1966. Clin Oral Investig. 2021;25:1829–1837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Duran CE, Azermai M, Vander Stichele RH. Systematic review of anticholinergic risk scales in older adults. Eur J Clin Pharmacol. 2013;69:1485–1496. [DOI] [PubMed] [Google Scholar]
- 43.Scully C Drug effects on salivary glands: dry mouth. Oral Dis. 2003;9:165–176. [DOI] [PubMed] [Google Scholar]
- 44.Aboulhoda BE, Ali EN. Evaluating the effect of three newly approved overactive bladder syndrome treating agents on parotid and submandibular salivary glands: modulation of CXCL10 expression. Acta Histochem. 2018;120:269–281. [DOI] [PubMed] [Google Scholar]
- 45.Tobin G, Ryberg AT, Gentle S, Edwards AV. Distribution and function of muscarinic receptor subtypes in the ovine submandibular gland. J Appl Physiol. 1985;100:1215–1223. 2006. [DOI] [PubMed] [Google Scholar]
- 46.Ryberg AT, Selberg H, Soukup O, Gradin K, Tobin G. Cholinergic submandibular effects and muscarinic receptor expression in blood vessels of the rat. Arch Oral Biol. 2008;53:605–616. [DOI] [PubMed] [Google Scholar]
- 47.Bretz WA, Loesche WJ, Chen YM, Schork MA, Dominguez BL, Grossman N. Minor salivary gland secretion in the elderly. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:696–701. [DOI] [PubMed] [Google Scholar]
- 48.Eliasson L, Carlen A. An update on minor salivary gland secretions. Eur J Oral Sci. 2010;118:435–442. [DOI] [PubMed] [Google Scholar]
- 49.Lee SK, Lee SW, Chung SC, Kim YK, Kho HS. Analysis of residual saliva and minor salivary gland secretions in patients with dry mouth. Arch Oral Biol. 2002;47:637–641. [DOI] [PubMed] [Google Scholar]
- 50.Leung HY, Yip SK, Cheon C, et al. A randomized controlled trial of tolterodine and oxybutynin on tolerability and clinical efficacy for treating Chinese women with an overactive bladder. BJU Int. 2002;90:375–380. [DOI] [PubMed] [Google Scholar]
- 51.Moller HJ, Demyttenaere K, Olausson B, et al. Two phase III randomised double-blind studies of fixed-dose TC-5214 (dexmecamylamine) adjunct to ongoing antidepressant therapy in patients with major depressive disorder and an inadequate response to prior antidepressant therapy. World J Biol Psychiatry. 2015;16:483–501. [DOI] [PubMed] [Google Scholar]
- 52.Cappetta K, Beyer C, Johnson JA, Bloch MH. Meta-analysis: risk of dry mouth with second generation antidepressants. Prog Neuropsychopharmacol Biol Psychiatry. 2018;84:282–293. [DOI] [PubMed] [Google Scholar]
- 53.Van Kerrebroeck P, Kreder K, Jonas U, Zinner N, Wein A, Group Tolterodine Study. Tolterodine once-daily: superior efficacy and tolerability in the treatment of the overactive bladder. Urology. 2001;57:414–421. [DOI] [PubMed] [Google Scholar]
- 54.Tan ECK, Lexomboon D, Sandborgh-Englund G, Haasum Y, Johnell K. Medications that cause dry mouth as an adverse effect in older people: a systematic review and metaanalysis. J Am Geriatr Soc. 2018;66:76–84. [DOI] [PubMed] [Google Scholar]
- 55.Xu D, Anderson HD, Tao A, et al. Assessing and predicting drug-induced anticholinergic risks: an integrated computational approach. Ther Adv Drug Saf. 2017;8:361–370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Ship JA, Pillemer SR, Baum BJ. Xerostomia and the geriatric patient. J Am Geriatr Soc. 2002;50:535–543. [DOI] [PubMed] [Google Scholar]
- 57.Field EA, Fear S, Higham SM, et al. Age and medication are significant risk factors for xerostomia in an English population, attending general dental practice. Gerodontology. 2001;18:21–24. [DOI] [PubMed] [Google Scholar]
- 58.Pajukoski H, Meurman JH, Halonen P, Sulkava R. Prevalence of subjective dry mouth and burning mouth in hospitalized elderly patients and outpatients in relation to saliva, medication, and systemic diseases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:641–649. [DOI] [PubMed] [Google Scholar]
- 59.Loesche WJ, Bromberg J, Terpenning MS, et al. Xerostomia, xerogenic medications and food avoidances in selected geriatric groups. J Am Geriatr Soc. 1995;43:401–407. [DOI] [PubMed] [Google Scholar]
- 60.Ogasawara T, Andou N, Kawase S, et al. Potential factors responsible for dryness of the dorsum of the tongue in elderly requiring care. Gerodontology. 2008;25:217–221. [DOI] [PubMed] [Google Scholar]
- 61.Dormenval V, Budtz-Jorgensen E, Mojon P, Bruyere A, Rapin CH. Associations between malnutrition, poor general health and oral dryness in hospitalized elderly patients. Age Ageing. 1998;27:123–128. [DOI] [PubMed] [Google Scholar]
- 62.Bergdahl M, Bergdahl J. Low unstimulated salivary flow and subjective oral dryness: association with medication, anxiety, depression, and stress. J Dent Res. 2000;79:1652–1658. [DOI] [PubMed] [Google Scholar]
- 63.Lampela P, Tolppanen AM, Tanskanen A, Tiihonen J, Hartikainen S, Taipale H. Anticholinergic exposure and risk of pneumonia in persons with Alzheimer’s disease: a nested case-control study. J Alzheimers Dis. 2017;56:119–128. [DOI] [PubMed] [Google Scholar]
- 64.Ingelman-Sundberg M Human drug metabolising cytochrome P450 enzymes: properties and polymorphisms. Naunyn Schmiedebergs Arch Pharmacol. 2004;369:89–104. [DOI] [PubMed] [Google Scholar]
- 65.Kersten H, Wyller TB, Molden E. Association between inherited CYP2D6/2C19 phenotypes and anticholinergic measures in elderly patients using anticholinergic drugs. Ther Drug Monit. 2014;36:125–130. [DOI] [PubMed] [Google Scholar]
- 66.Affairs American Dental Association Council on Scientific. Professionally applied topical fluoride: evidence-based clinical recommendations. J Am Dent Assoc. 2006;137:1151–1159. [DOI] [PubMed] [Google Scholar]
- 67.Jager DHJ, Bots CP, Forouzanfar T, Brand HS. Clinical oral dryness score: evaluation of a new screening method for oral dryness. Odontology. 2018;106:439–444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Humphrey SP, Williamson RT. A review of saliva: normal composition, flow, and function. J Prosthet Dent. 2001;85:162–169. [DOI] [PubMed] [Google Scholar]
- 69.Janssens B, Petrovic M, Jacquet W, Schols J, Vanobbergen J, De Visschere L. Medication use and its potential impact on the oral health status of nursing home residents in Flanders (Belgium). J Am Med Dir Assoc. 2017;18. 809.e1–809.e8. [DOI] [PubMed] [Google Scholar]
- 70.Aliko A, Wolff A, Dawes C, et al. World Workshop on Oral Medicine VI: clinical implications of medication-induced salivary gland dysfunction. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120:185–206. [DOI] [PubMed] [Google Scholar]
- 71.Tandon A, Singh NN, Sreedhar G. Minor salivary glands and dental caries: approach towards a new horizon. J Nat Sci Biol Med. 2013;4:364–368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Jurasic MM, Gibson G, Wehler CJ, Orner MB, Jones JA. Caries prevalence and associations with medications and medical comorbidities. J Public Health Dent. 2019;79:34–43. [DOI] [PubMed] [Google Scholar]
- 73.Navazesh M Methods for collecting saliva. Ann N Y Acad Sci. 1993;694:72–77. [DOI] [PubMed] [Google Scholar]
- 74.Billings RJ, Proskin HM, Moss ME. Xerostomia and associated factors in a community-dwelling adult population. Community Dent Oral Epidemiol. 1996;24:312–316. [DOI] [PubMed] [Google Scholar]
- 75.Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc. 1987;115:581–584. [DOI] [PubMed] [Google Scholar]
- 76.Singh ML, Papas A. Oral implications of polypharmacy in the elderly. Dent Clin North Am. 2014;58:783–796. [DOI] [PubMed] [Google Scholar]
- 77.Kersten H, Molden E, Tolo IK, Skovlund E, Engedal K, Wyller TB. Cognitive effects of reducing anticholinergic drug burden in a frail elderly population: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2013;68:271–278. [DOI] [PubMed] [Google Scholar]
- 78.Vrolijk MF, Opperhuizen A, Jansen EH, Bast A, Haenen GR. Anticholinergic accumulation: a slumbering interaction between drugs and food supplements. Basic Clin Pharmacol Toxicol. 2015;117:427–432. [DOI] [PubMed] [Google Scholar]
- 79.Guggenheimer J, Moore PA. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc. 2003;134:61–69. quiz 118-119. [DOI] [PubMed] [Google Scholar]
- 80.Dauphinot V, Mouchoux C, Veillard S, Delphin-Combe F, Krolak-Salmon P. Anticholinergic drugs and functional, cognitive impairment and behavioral disturbances in patients from a memory clinic with subjective cognitive decline or neurocognitive disorders. Alzheimers Res Ther. 2017;9:58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Ryberg AT, Warfvinge G, Axelsson L, Soukup O, Gotrick B, Tobin G. Expression of muscarinic receptor subtypes in salivary glands of rats, sheep and man. Arch Oral Biol. 2008;53:66–74. [DOI] [PubMed] [Google Scholar]
- 82.Abrams P, Andersson KE, Buccafusco JJ, et al. Muscarinic receptors: their distribution and function in body systems, and the implications for treating overactive bladder. Br J Pharmacol. 2006;148:565–578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Tobin G, Giglio D, Gotrick B. Studies of muscarinic receptor subtypes in salivary gland function in anaesthetized rats. Auton Neurosci. 2002;100:1–9. [DOI] [PubMed] [Google Scholar]