

Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by impaired social interaction and restricted behaviour patterns, with an onset that usually occurs in early childhood (1). Epidemiological studies show an increasing prevalence of ASD worldwide (2). The reported prevalence of atopic dermatitis (AD), which also has an onset predominantly in childhood, has also increased. AD is associated with various mental health disorders, such as anxiety, depression and attention deficit hyperactivity disorder (3). Miyazaki et al. (4) showed, in a meta-analysis published in 2015, that, compared with controls, patients with ASD have a higher prevalence of asthma and allergic rhinitis, but not of AD. However, only 5 studies involving 417 patients with AD were included in this meta-analysis (4). More epidemiological studies have since been published addressing this issue (5, 6). The aim of the current study was to examine the correlation between ASD and AD in a systematic review and meta-analysis.
MATERIALS AND METHODS
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist and was registered in PROSPERO (CRD 42019140441).
Studies indexed in PubMed, the Cochrane Library, and Embase databases from the inception of the databases to 15 April 2019, were investigated. Only clinical studies in humans were included. The search terms included [“atopic dermatitis” or “eczema”] and [“autism” or “Asperger syndrome” or “autism spectrum disorders”]. References within the searched articles were also reviewed to identify studies that could have been missed.
The study selection included cohort, case-control, and population survey studies comparing the prevalence of AD in patients with ASD, or the prevalence of ASD in patients with AD, with that in controls. The titles and abstracts of identified articles were screened independently by 2 authors (TYT and YCC). Review articles, case reports, correspondence, and data from conferences were excluded.
The outcomes analysed in this study were the prevalence of AD in patients with ASD compared with that in controls and vice versa.
Data were extracted independently by 2 authors (TYT and YCC). Data extraction results were compared, and discrepancies were resolved by consensus. The quality of each study was evaluated using the Newcastle-Ottawa Scale. Data were collected regarding: the country where the study was conducted; study design; data sources; inclusion periods and criteria; sample size; diagnostic criteria for AD and ASD; study results; and study quality scores (Table SI1).
A random effects model was used. Odds ratio (OR) with 95% confidence interval (95% CI) were used to compare the prevalence of the diseases. Subgroup analysis was performed according to study designs. For included studies that had overlapping datasets collected from the same databases, only one of the studies was used for quantitative analysis. Sensitivity analyses were performed by including only one of the studies that used the same databases at a time. Heterogeneity was assessed with the I2 test, and risk of publication bias with the Begg’s test. All analyses were performed with Comprehensive Meta-Analysis Version 3 (Biostat, Inc., Englewood, NJ, USA).
RESULTS
Of the 24 potentially relevant publications identified through online database searches, 17 met the inclusion criteria (Fig. 1). The characteristics of the included studies are summarized in Table SI1. There were 10 population-based studies (2 cohort, 4 case-control, and 4 population survey studies) and 7 institution-based case-control studies. One population survey and 5 institution-based studies found no significant correlation between AD and ASD. The other 11 studies found significant correlations between AD and ASD.
Fig. 1.
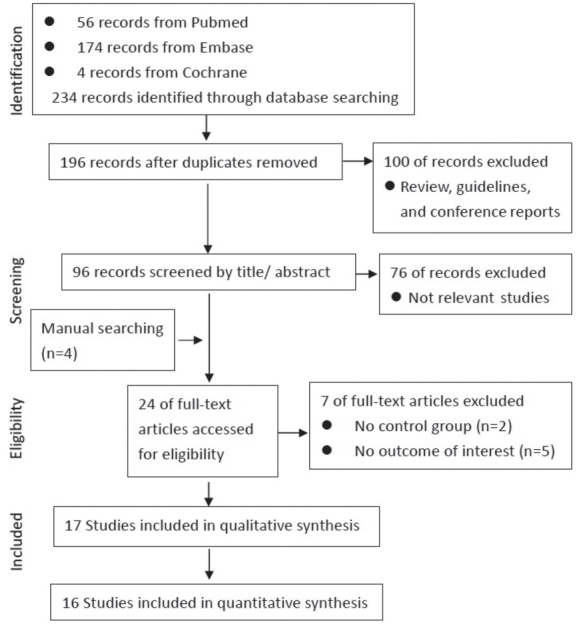
Study flow diagram. Selection of studies included in the present systematic review and meta-analysis.
The overall pooled analysis and subgroup analyses according to different study types all showed significantly higher prevalence of AD in patients with ASD than in controls (overall OR 1.49; 95% CI 1.20–1.83). Pooling the adjusted ORs also revealed a significant correlation between AD and ASD (OR 1.98; 95% CI 1.34–2.94). The results remained consistent in all sensitivity analyses (Fig. 2). No publication bias was noted.
Fig. 2.

Forest plots. The forest plots revealed significantly higher prevalence of atopic dermatitis in patients with autism spectrum disorder (ASD) than in controls (overall odds ratio (OR) 1.485; 95% confidence interval (95% CI) 1.203–1.834).Subgroup analyses, based on different study designs and sensitivity analyses, revealed consistent results.
DISCUSSION
In contrast to the meta-analysis of Miyazaki et al. (4), the current study found a significant correlation between AD and ASD. This finding is consistent with the results of the systematic review by Billeci et al. (7). However, the current study analysed the findings of a higher number of studies, including 2 new population-based cohort studies, and undertook quantitative analysis to strengthen the evidence.
The correlation between AD and ASD could be attributable to shared genetic and immunological pathways. The pathogenesis of AD and ASD both involve interactions between genes and the environment (7). Several genes have been found to play important roles in both conditions; for example, ADRB2, GATA-3, and brain-derived neurotrophic factor genes (7). From the immunological perspective, pro-inflammatory cytokines produced in atopic responses, such as interleukin 6 (IL-6) and tumour necrosis factor (TNF)-α, could disrupt blood–brain barriers, inducing neuroimmunological effects on neural circuits associated with emotional and behavioural functions (8). Moreover, mast cells, a major effector cell in the pathogenesis of AD, may be activated perinatally by various factors, leading to the production of neurotoxins that contribute to the mechanisms of ASD (9). Vitamin D regulates innate and adaptive immune pathways and vitamin D deficiency is associated with various allergic conditions, including AD (10). There is increasing evidence for maternal and neonatal vitamin D deficiency in patients with ASD, which supports the hypothesis that AD and ASD share common pathophysiological mechanisms (11). When patients are diagnosed with AD or ASD, clinicians should remain vigilant for the early symptoms and signs of the other condition, in order to allow early detection and timely interventions for either condition. Further research is needed into the possibility of shared pathophysiology between AD and ASD, as this could lead to the development of interventions targeted at common pathways, in order to treat the symptoms of both conditions simultaneously.
This study has a number of limitations. A major limitation is the significant heterogeneity, possibly stemming from variations in study design, disease diagnostic criteria, age, race, and disease severity among participants in the included studies. In addition, it should be noted that the study only shows correlation between AD and ASD, and not causation.
In conclusion, this study demonstrates a significant correlation between AD and ASD. Physicians should therefore be alert to the early symptoms and signs of ASD in patients with AD and vice versa. Further research is needed into the possibility of shared pathogenesis between AD and ASD.
The authors have no conflicts of interest to declare.
REFERENCES
- 1.Matson JL, Kozlowski AM. The increasing prevalence of autism spectrum disorders. Res Autism Spectr Disord 2011; 5: 418–425. [Google Scholar]
- 2.Chiarotti F, Venerosi A. Epidemiology of autism spectrum disorders: a review of worldwide prevalence estimates since 2014. Brain Sciences 2020; 10: 274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Simpson EL. Comorbidity in atopic dermatitis. Curr Dermatol Rep 2012; 1: 29–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Miyazaki C, Koyama M, Ota E, Swa T, Amiya RM, Mlunde LB, et al. Allergies in children with autism spectrum disorder: a systematic review and meta-analysis. J Autism Dev Disord 2015; 2: 374–401. [Google Scholar]
- 5.Liao TC, Lien YT, Wang S, Huang SL, Chen CY. Comorbidity of atopic disorders with autism spectrum disorder and attention deficit/hyperactivity disorder. J Pediatr 2016; 171: 248–245. [DOI] [PubMed] [Google Scholar]
- 6.Lee CY, Chen MH, Jeng MJet al. Longitudinal association between early atopic dermatitis and subsequent attention-deficit or autistic disorder: A population-based case-control study. Medicine (Baltimore) 2016; 95: e5005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Billeci L, Tonacci A, Tartarisco G, Ruta L, Pioggia G, Gangemi S. Association between atopic dermatitis and autism spectrum disorders: a systematic review. Am J Clin Dermatol 2015; 16: 371–388. [DOI] [PubMed] [Google Scholar]
- 8.Theoharides TC, Tsilioni I, Patel AB, Doyle R. Atopic diseases and inflammation of the brain in the pathogenesis of autism spectrum disorders. Transl Psychiatry 2016; 6: e844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Theoharides TC, Angelidou A, Alysandratos KD, Zhang B, Asadi S, Francis K, et al. Mast cell activation and autism. Biochim Biophys Acta 2012; 1822: 34–41. [DOI] [PubMed] [Google Scholar]
- 10.Kim G, Bae JH. Vitamin D and atopic dermatitis: a systematic review and meta-analysis. Nutrition 2016; 32: 913–920. [DOI] [PubMed] [Google Scholar]
- 11.Mazahery H, Camargo CA Jr, Conlon C, Beck KL, Kruger MC, von Hurst PR. Vitamin D and autism spectrum disorder: a literature review. Nutrients 2016; 8: 236. [DOI] [PMC free article] [PubMed] [Google Scholar]