
ED Fig. 2. Additional patient images by isotope showing the versatility of CCLI reflect the employed tracer and patient imaging location.
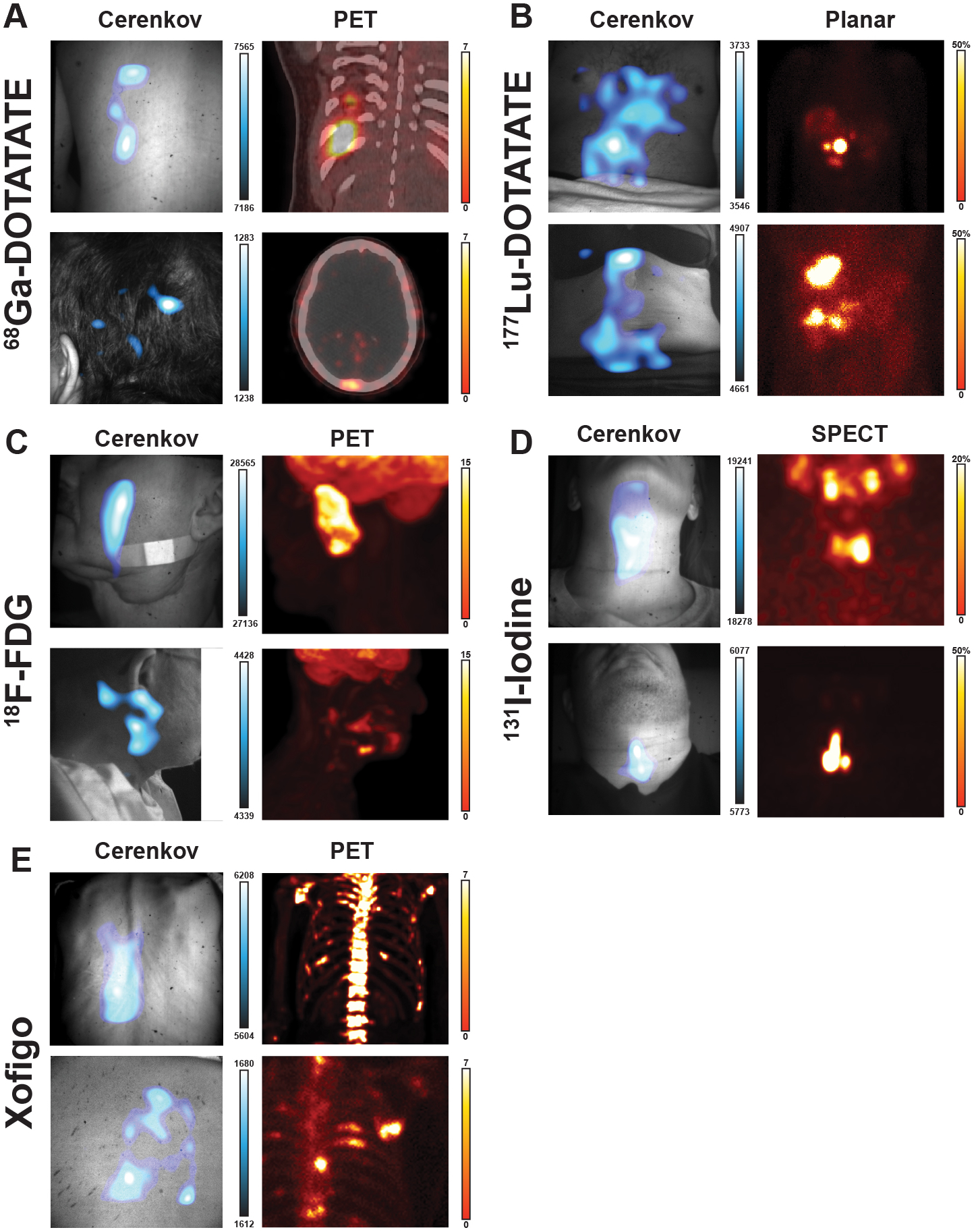
A) Top, 68Ga-DOTATATE CLI image shows three lesions on the posterior agree with the PET/CT, the presence on the posterior of a superficial lesion near the ribcage, directly above the spleen. Lesion discrepancy between PET and CLI is likely due to rib bone absorption. Bottom, a second patient has a prominent spot on their head in the CLI image which aligns with a lesion seen in the PET/CT in the occipital bone near the lamboid suture. B) Top, 177Lu-DOTATATE CLI image shows a patient with the brightest spot below the liver with a secondary area near the patient midline below the Xiphoid Process. The main focal spot is in agreement with the planar scan the patient received prior showing one main lesion in a cluster of four below the liver near the patient midline. Bottom, CLI image of a second patient showing a focal region just above the Xiphoid Process with a secondary focal area to the patient’s right abdomen in line with the navel. The corresponding planar image shows two sets of lesions, one in the top of the right lobe as well as two lesions in the bottom of the right lobe of the liver. C) Top, 18F-FDG CLI image shows a vertical focal signal in the cheek and not near the applied bandage. The corresponding PET image shows the most avid region by the zygomatic bone and nearly vertical with the patient. The physiologic uptake in the brain is not seen as it is both less intense and attenuated by the skull. Bottom, a second 18F-FDG patient CLI image shows three clusters at the base of the jaw and around the ear. The corresponding PET scan shows three sets of avid tissue in the region in agreement with the CLI image, with the brightest lesion buried in the submandibular triangle. E) Top, 223RaCl2 CLI image shown from the patients back that the main CLI intensity is to the left of the spine, near the liver. A prior 18F scan from the previous month shows extensive uptake in the spine, suggesting the CLI intensity seen is distribution of 223RaCl2 through the liver and not appreciable bone uptake. Bottom, CLI image showing a patient’s right posterior to the left of the scapula from an elevated angle above the patient with three focal regions seen. The prior 18F bone scan from the previous month shows uptake in the 4th and 5th ribs, alongside two focal lesions on either side. Here the CLI image shows potential agreement with the 18F scan, though physiologic distribution via stomach and gastrointestinal tract confounds agreement.