
Figure 1. Histologic Features of LCH.
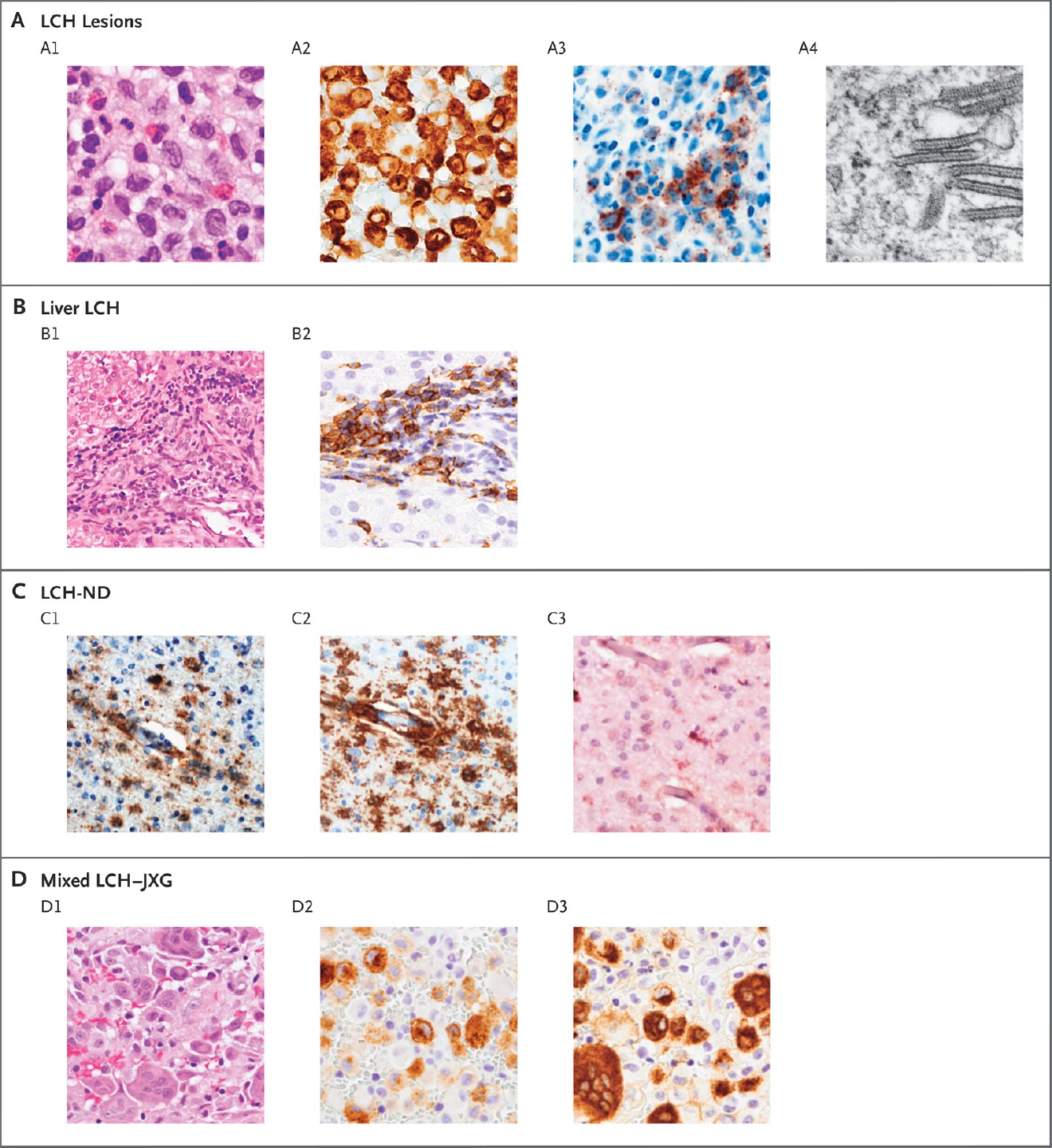
Panel A shows typical LCH lesions with large cells, pale cytoplasm, and reniform nuclei on hematoxylin and eosin staining (A1); CD207-positive immunostaining (A2); VE1-positive immunostaining for BRAF V600E protein (A3); and Birbeck granules visualized with electron microscopy (A4). Panel B shows liver involvement, which is frequently characterized by periportal infiltration by histiocytes (B1) and variable CD207-positive staining (B2). Panel C shows biopsy specimens from a patient with severe LCH-associated neurodegeneration (LCH-ND), characterized by perivascular VE1-positive staining (C1), CD163-positive staining (C2), and a P2RY12 infiltrate with occasional P2RY12-positive, tissue-resident microglia (C3). Panel D shows histiocytic lesions that are characteristic of both LCH and juvenile xanthogranuloma (JXG), with heterogeneous histologic features on hematoxylin and eosin staining (D1), including distinct cell populations that are CD207-positive (D2) and CD68-positive (D3).
(From NEJM, Langerhans Cell Histiocytosis, 379:856–8683; Copyright ©2018 Massachusetts Medical Society. Reprinted with permission.)