
Figure 4. Adoptive cell therapy with alloprimed CXCR5+CD8+ T cells into CCR5 KO kidney transplant recipients significantly inhibits alloantibody production.
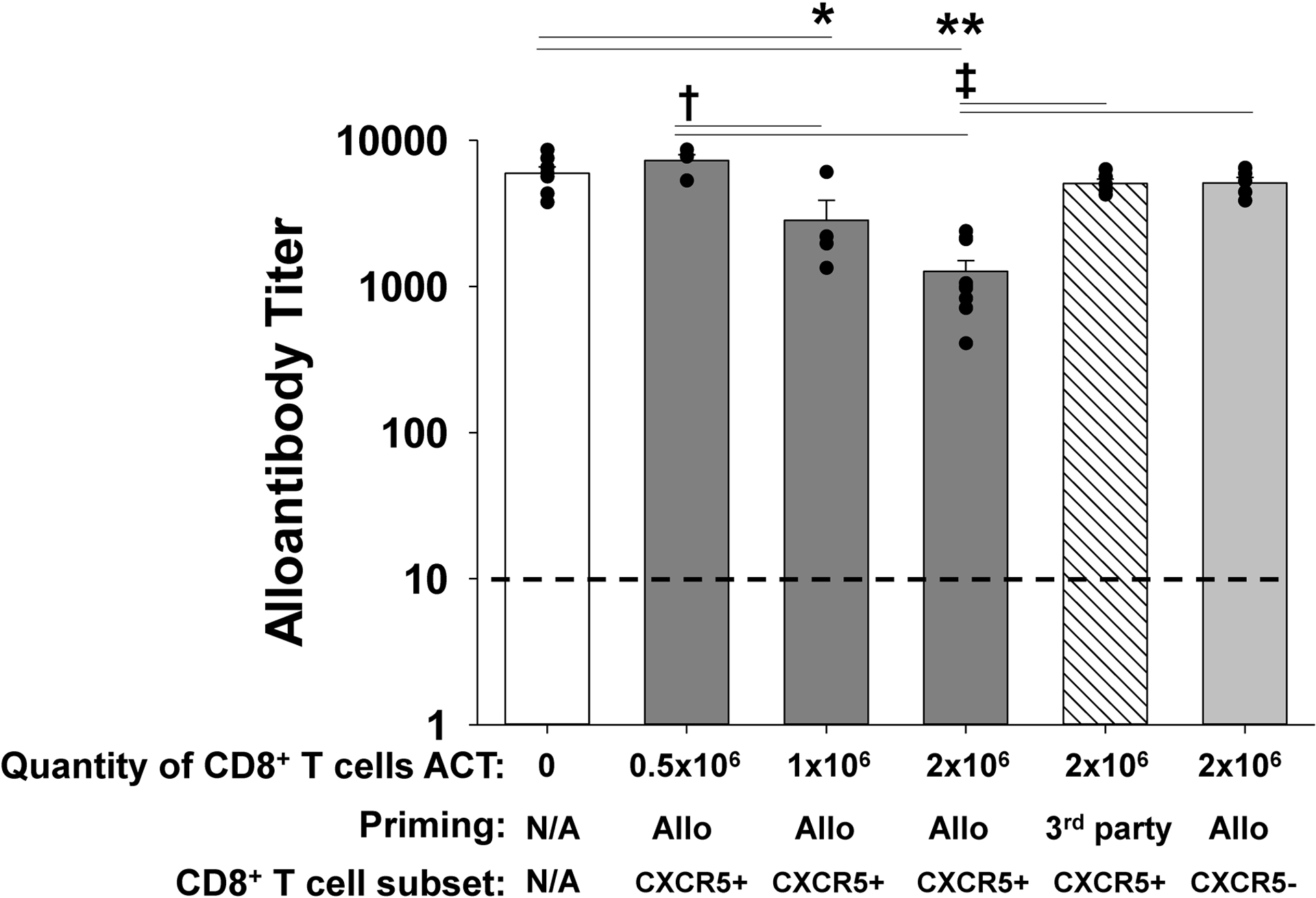
CCR5 KO (H-2b) mice were transplanted with an allogeneic kidney (A/J, H-2a). On day 5 posttransplant, a cohort of CCR5 KO recipients received adoptive cell therapy (ACT) with 0.5×106, 1×106, or 2×106 flow-sorted alloprimed CXCR5+CD8+ T cells (retrieved from A/J allolysate primed C57BL/6, H-2b, mice). Day 14 posttransplant serum from kidney transplant recipients was analyzed for alloantibody titer. Alloantibody production was significantly reduced following ACT with 1×106 CXCR5+CD8+ T cells (titer = 2,800±1,100, n=4; *p=0.0015) and ACT with 2×106 cells (titer = 1,300±240, n=9; **p<0.0001) compared to CCR5 KO recipients without ACT (titer= 6,000±630, n=7). Both ACT of 1×106 and 2×106 alloprimed CXCR5+CD8+ T cells inhibited alloantibody titer more than ACT with 0.5×106 alloprimed cells (†p<0.0002 for both). No significant reduction was observed with ACT with 0.5×106 alloprimed CXCR5+CD8+ T cells (titer = 7,300±700, n=4), 2×106 3rd party primed (FVB/N, H-2q) CXCR5+CD8+ T cells (titer = 5,100±370, n=5), or with 2×106 alloprimed CXCR5−CD8+ T cells (titer= 5,100±470, n=5). Recipient mice that received ACT with either 2×106 3rd party primed CXCR5+CD8+ T cells or alloprimed CXCR5−CD8+ T cells had significantly higher alloantibody titers compared to recipients that received 2×106 alloprimed CXCR5+CD8+ T cells (‡p<0.0001 for both). Dashed line represents naïve control sera.