
Central Illustration. Pericoronary Adipose Tissue Attenuation and Low Attenuation Plaque Burden Provide Complementary Predictive Value for 5-year Risk of Fatal or Nonfatal Myocardial Infarction in Patients with Suspected Coronary Artery Disease.
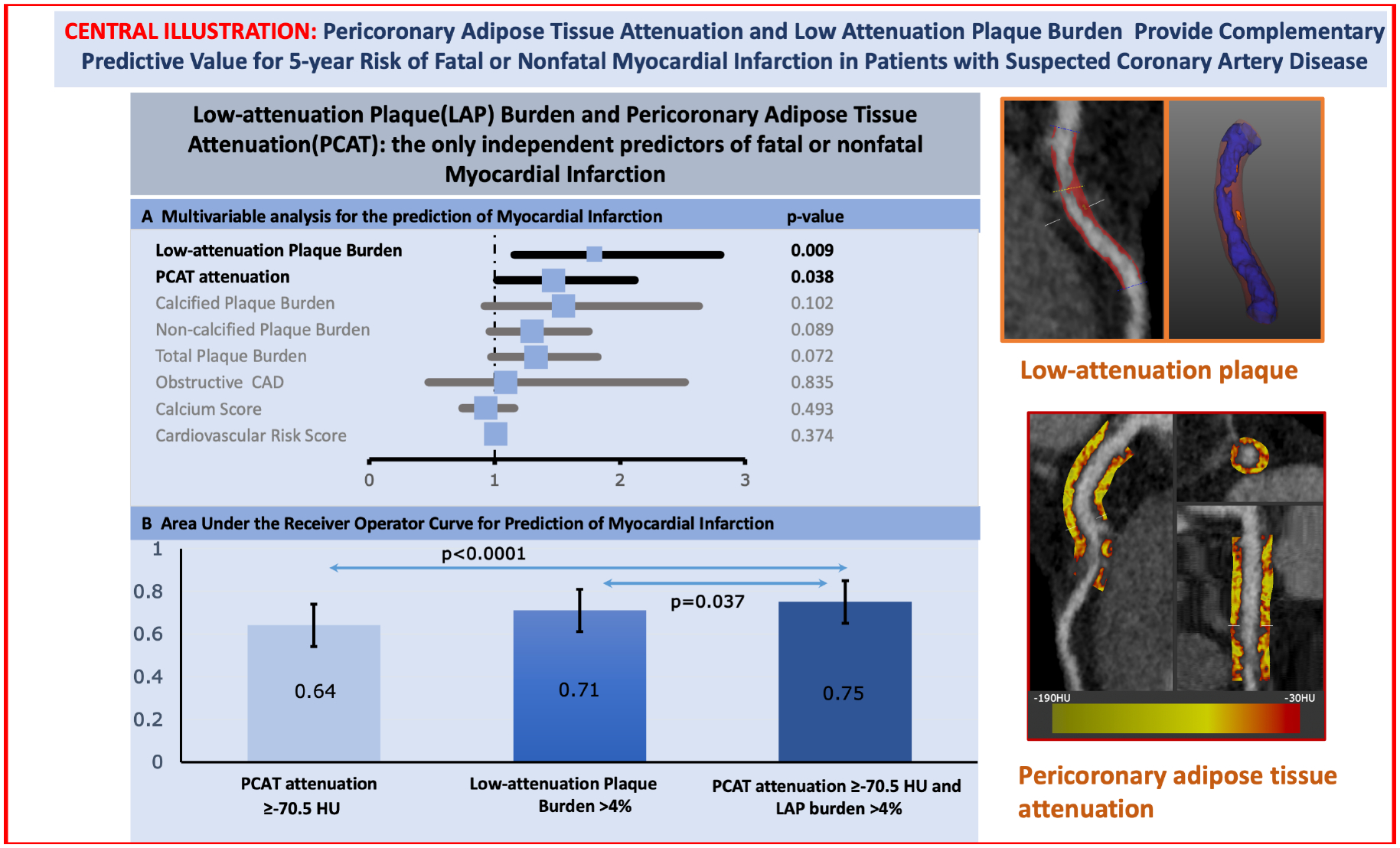
(Left – Top) Forrest plot of the multivariable analysis for the prediction of myocardial infarction. Low-attenuation Plaque (LAP) Burden and Pericoronary Adipose Tissue Attenuation (PCAT) are the only independent predictors of fatal or nonfatal Myocardial Infarction. (Left-Bottom) Bar graph with 95% confidence interval error bars comparing the area under the receiver operator characteristic curve (AUC) for the prediction of myocardial. Low-attenuation plaque burden showed higher area-under-the-curve (AUC) compared to PCAT-RCA attenuation for the prediction for myocardial infarction [0.71 (0.62–0.80) versus 0.64 (0.54–0.74); p<0.001], with the combination of both parameters yielding the highest AUC [0.75 (0.65–0.85); p=0.037] (Right) Based on the Youden’s index of the ROC curves, the optimal cut-off of the right coronary artery PCAT attenuation was −70.5 HU for the primary endpoint of fatal or non-fatal myocardial infarction. Patients with PCAT-RCA above ≥−70.5 HU were nearly 2.5 times more likely to suffer a myocardial infarction (HR 2.45, 95% CI 1.23 to 4.80; p=0.001). Patients with low-attenuation plaque burden (greater than 4%) were nearly 5 times more likely to suffer a myocardial infarction (HR 4.87, 95% CI 2.03 to 11.78, p<0.0001). When the two metrics were combined, patients with both low-attenuation plaque burden >4% and PCAT-RCA ≥−70.5 HU were at the greatest risk of myocardial infarction (HR 11.7, 95% CI 3.3 to 40.9, p<0.0001)