
Figure 2. Cumulative Incidence of COVID-19 Vaccination in the Culturally Tailored Primary Care Physician (PCP) Outreach, Standard PCP Outreach, and Usual Care Arms Among Black and Latino Adults Aged 65 Years and Older.
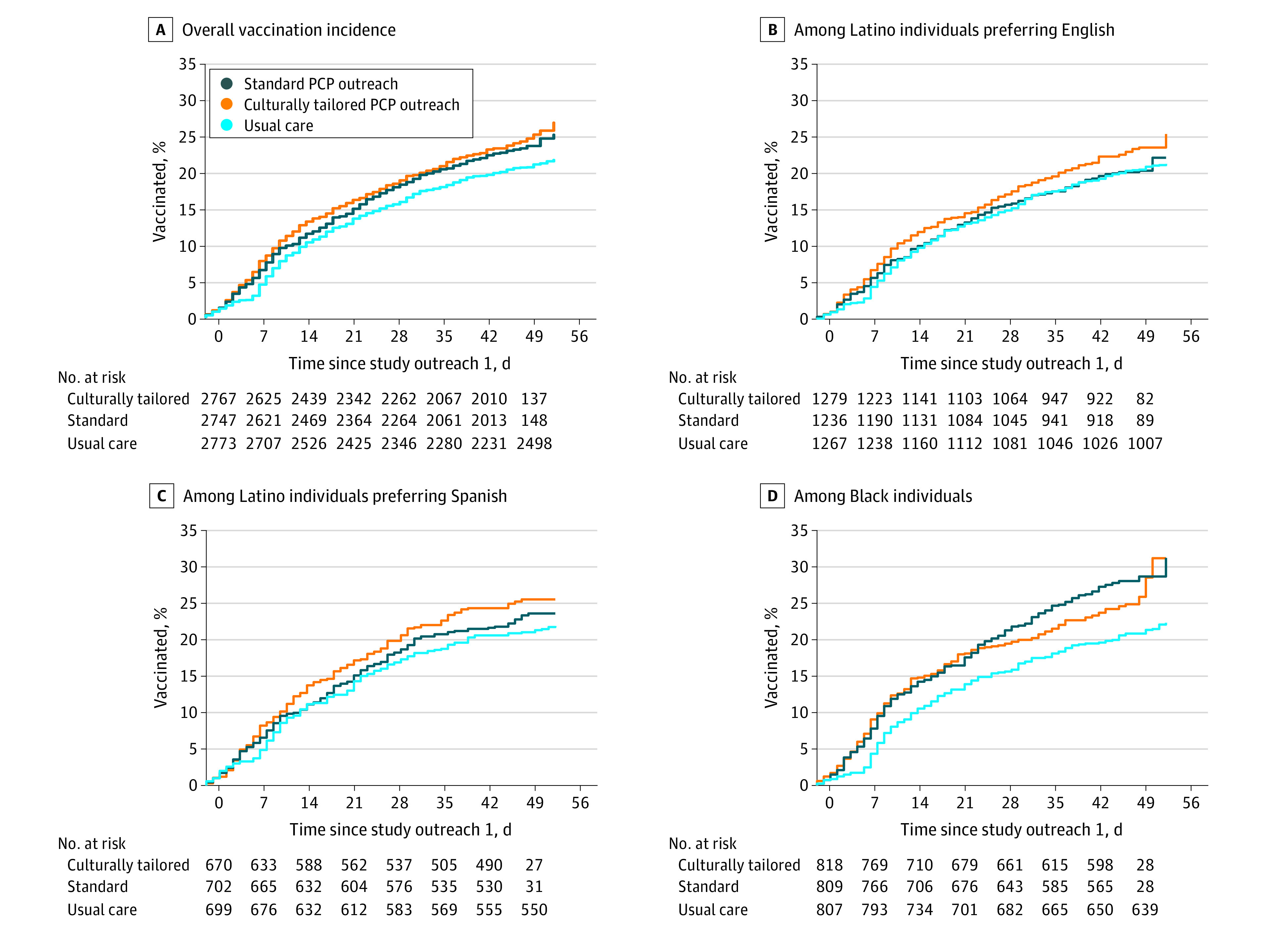
A. Culturally tailored PCP outreach resulted in a significantly higher rate of vaccination than usual care (adjusted hazard ratio [aHR], 1.22; 95% CI, 1.09-1.37; P < .001), as did standard PCP outreach (aHR, 1.17; 95% CI, 1.04-1.31; P = .007). The difference between culturally tailored and standard PCP outreach was not significant (aHR, 1.04; 95% CI, 0.94-1.17; P = .42). B. Culturally tailored PCP outreach resulted in a higher rate of vaccination than usual care, but the difference was not statistically significant (aHR, 1.16; 95% CI, 0.98-1.37; P = .09). The differences between standard PCP outreach and usual care (aHR, 1.02; 95% CI, 0.85-1.21; P = .85) and between culturally tailored and standard PCP outreach (aHR, 1.14; 95% CI, 0.96-1.35; P = .13) were not significant. C. Culturally tailored PCP outreach resulted in a significantly higher rate of vaccination than usual care (aHR, 1.25; 95% CI, 1.00 - 1.56; P = .049). The differences between standard PCP outreach and usual care (aHR, 1.12; 95% CI, 0.89-1.40, P = .33) and between culturally tailored and standard PCP outreach was not significant (aHR, 1.12; 95% CI, 0.90-1.39, P = .32) were not significant. D. Culturally tailored PCP outreach resulted in a significantly higher rate of vaccination than usual care (aHR, 1.30; 95% CI, 1.06-1.59; P = .011), as did standard PCP outreach (aHR, 1.45; 95% CI, 1.19-1.77; P < .001). The difference between culturally tailored and standard PCP outreach was not significant (aHR, 0.90; 95% CI, 0.74-1.08; P = .25).