
Figure 1. Model structure.
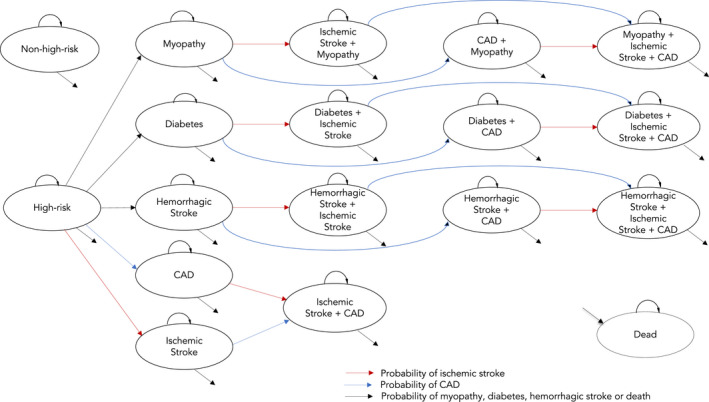
The Markov model structure used in this study is shown with a total of 18 health states. The initial cohort was distributed in 2 groups: high‐risk cohort and nonhigh‐risk cohort. We defined high risk as individuals in the top quintile of the polygenic risk score (PRS) for coronary artery disease (CAD‐PRS) distribution or having other risk‐enhancing factor (eg, family history), while the nonhigh‐risk group included individuals in the bottom 80% of the CAD‐PRS distribution without any risk‐enhancing factor. In the pooled cohort equation (PCE)+CAD‐PRS strategy, all of the high‐risk cohort was initiated on statin preventive therapy to reduce the risk of coronary artery disease (CAD) and stroke, while for the PCE‐alone strategy only a proportion of patients with other risk‐enhancing factors initiated statins. We accounted for statin side effects such as diabetes, myopathy, and hemorrhagic stroke and subsequent risk of ischemic stroke and CAD. In the PCE‐alone strategy, CAD‐PRS was not considered as a risk‐enhancing factor, so only those with other risk‐enhancing factors initiated statins. Health outcomes were not examined for the nonhigh‐risk cohort.