
Central Figure: Bypassed native coronary arteries demonstrate increased disease activity and faster disease progression.
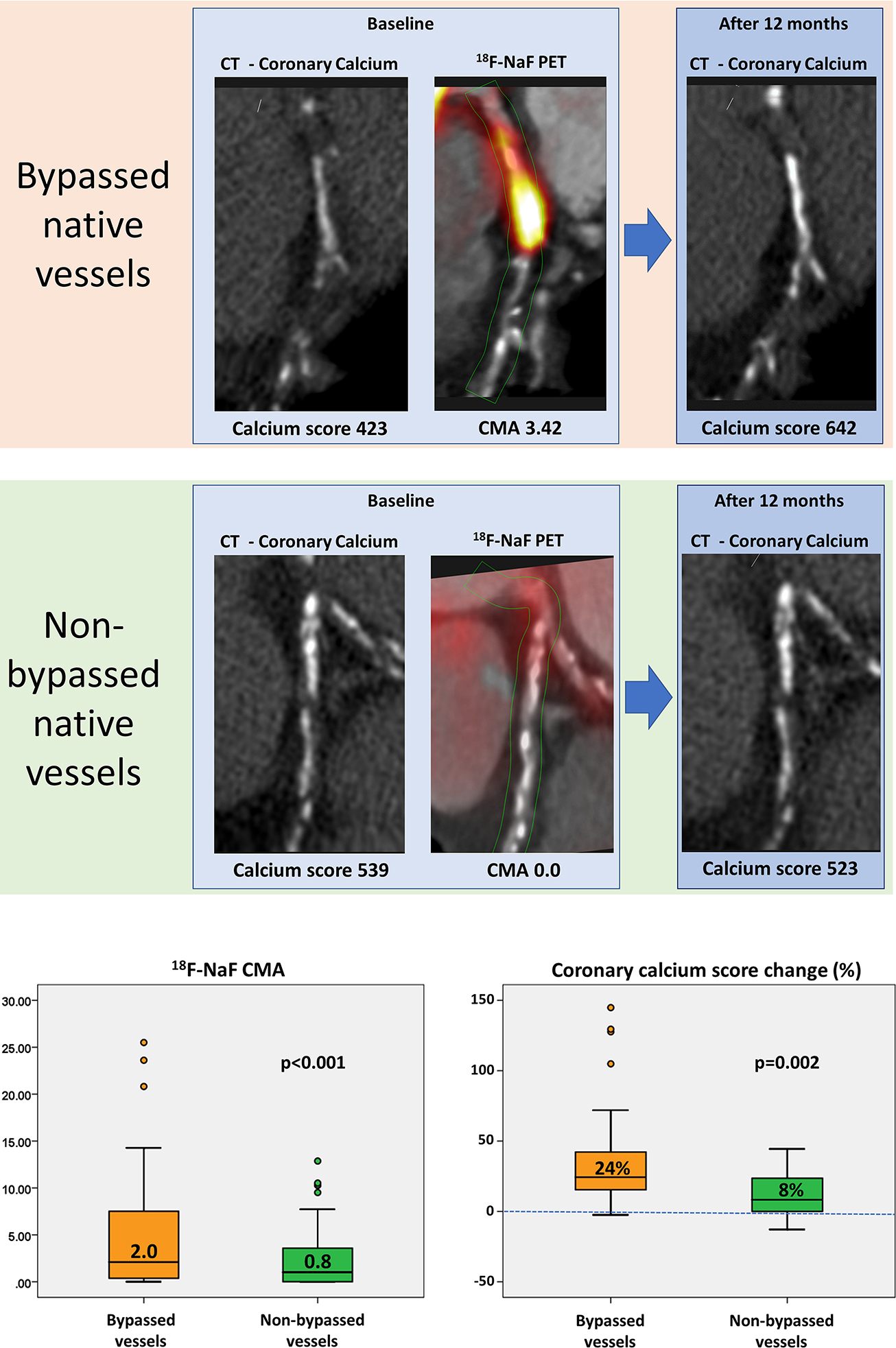
Co-registered coronary CT angiography with 18F-sodium fluoride (18F-NaF) positron emission tomography (PET) and non-contrast CT at baseline and after 12 months of follow-up in a patient with (top row) and without (bottom row) a history of surgical revascularization. Despite similar co-morbidities and plaque burdens bypassed native coronary vessels demonstrate both greater disease activity (coronary microcalcification activity [CMA] on 18F-NaF PET) and more rapid disease progression (change in the coronary calcium score on CT) than non-bypassed coronary arteries.