

Abstract
A wide spectrum of phenotypic manifestations characterizes age-related macular degeneration (AMD). Drusen is considered the hallmark of AMD and is located underneath the retinal pigment epithelium (RPE). In contrast, subretinal drusenoid deposits (SDDs), also known as reticular pseudodrusens, are located in the subretinal space, on top of the RPE. SDDs are poorly detected by clinical examination and color fundus photography. Multimodal imaging is required for their proper diagnosis. SDDs are topographically and functionally related to rods. SDDs cause a deep impairment in retinal sensitivity and dark adaptation. SDDs are dynamic structures that may grow, fuse with each other, or regress over time. An intermediate step in some eyes is the development of an acquired vitelliform lesion. The presence of SDD confers an eye a high risk for the development of late AMD. SDD leads to macular neovascularization, particularly type 3, geographic atrophy, and outer retinal atrophy.
Keywords: Age-related macular degeneration, outer retinal atrophy, pseudodrusen, reticular drusen, reticular macular disease, reticular pseudodrusen, retinal angiomatous proliferation, subretinal drusenoid deposit, type 3 macular neovascularization
Introduction
Age-related macular degeneration (AMD) comprises a wide spectrum of phenotypic manifestations that vary from drusen to disciform scars. There has been a recent interest in defining the role and predictive value of subretinal drusenoid deposits (SDDs), also known as reticular pseudodrusen, reticular macular disease, and reticular drusen in the visual outcomes of AMD. SDD has been recognized as an important risk factor for the progression to late AMD.[1,2,3] Several reviews have been published in the past few years, underscoring the research interest in this topic.[3,4,5,6,7] In this narrative review, we aim to provide an updated description of this phenotypic characteristic of AMD.
Extracellular deposits in the fundus have been described for over a century and a half. However, it was not until the 1970s that Gass implicated drusen as part of the spectrum of AMD.[8,9] Clinically, these lesions appear as oval or round yellowish deposits of varying sizes in the posterior pole. In 1990, Mimoun et al.[10] used the term “les pseudo-drusen visibles en lumière bleue” (pseudodrusen best seen with blue light) to describe a yellowish interlacing reticular pattern of lesions of about 100 μ in size in patients with AMD. These were more easily seen under blue light. At the time, the authors were not sure what they were observing, thus the designation of pseudodrusen. They presumed that the lesions were located somewhere in the choroid.[10] The funduscopic appearance of SDD may resemble and may be confused with other phenotypic manifestations of AMD such as soft drusen or cuticular drusen. The differences in location with respect to the retinal pigment epithelium (RPE), differences in morphology, and the differences in optical filtering effects by the RPE and lesion composition determine their appearance under multimodal imaging. The Beer–Lambert law of light absorption explains these differences.[11] It is important to make the distinctions between the different extracellular macular deposits to more accurately assess the risk of disease progression in each patient. In 1991, the Wisconsin Age-Related Maculopathy Grading System recognized reticular soft drusen as part of the spectrum of AMD. They characterized them as drusen that formed “ill-defined networks of broad interlacing ribbons” on color fundus photographs (CFPs).[12] In 1995, Arnold et al.[13] coined the term reticular pseudodrusen to describe a particular yellowish pattern under the retina that consisted of lesions of 125–250 μm wide. This pattern was best seen with the He-Ne beam, with the red-free light or the infrared wavelength of the scanning laser ophthalmoscope (SLO). They noted that unlike true drusen, these pseudodrusens did not fluoresce on fluorescein or indocyanine green angiography (ICGA). In addition, they correlated the presence of reticular pseudodrusen as an important risk factor in the development of macular neovascularization (MNV).[13] During the next decade, histologic examination of donor eyes from an eye bank was shown to harbor deposits in the subretinal space in individuals with or without AMD. The protein components of these deposits were similar to drusen, hence their designation of SDD.[14] A decade ago, Zweifel et al.[15] and Schmitz-Valckenberg et al.[16] used spectral-domain optical coherence tomography (SD-OCT) to co-localize the so-called reticular pseudodrusen to these SDDs. It is currently accepted that SDD and reticular pseudodrusen refer to the same findings.
Subretinal Drusenoid Deposit and Conditions Other than Age-Related Macular Degeneration
SDDs are commonly found in patients with all phenotypes of AMD but are not specific to AMD.[16,17,18,19] The reported prevalence of SDD in AMD ranges from 9% to 70%.[13,17,20,21,22] The prevalence of SDD is strongly associated to AMD severity. For instance, in the ALSTAR study, SDDs were present in 49% of early AMD and 79% of intermediate AMD (iAMD) patients.[20] In patients with AMD and newly diagnosed MNV, 24% had SDD. The prevalence of type 3 MNV was significantly higher in eyes with SDD than in eyes without SDD.[17,23] Geographic atrophy (GA) has also been associated with SDD.[23] The prevalence of SDD was low in polypoidal choroidal vasculopathy (PCV) cases.[23,24]
SDDs have been reported in other conditions such as pseudoxanthoma elasticum,[25,26] Sorsby's dystrophy,[27] IgA nephropathy,[28] Vitamin A deficiency,[29] fundus albipunctatus,[30] retinitis punctate albescens,[30] adult-onset foveomacular dystrophy,[31] and extensive macular atrophy with pseudodrusen-like appearance.[32]
Some view SDD as an ocular manifestation of systemic disease and thus their designation of reticular macular disease.[33] Patients with SDD have been associated with cardiovascular risk and decreased renal function.[34,35] Patients with hypertensive choroidopathy and serous retinal detachment secondary to malignant hypertension and preeclampsia may develop lesions similar to SDD.[36] The Beaver Dam Eye Study reported that patients who had reticular drusen at baseline had a 54% poorer survival.[37] The Melbourne Collaborative Cohort Study did not find such an association.[38] A recent study also reported an impaired retinal arterial dilation in response to flicker light stimulation.[39]
SDD may even be present in healthy older individuals without any other ocular conditions. This finding raises the possibility that SDD may be a manifestation of aging or an earlier disease state of AMD.[40,41] In the absence of any other phenotypic AMD, the presence of SDD does not affect rod-mediated dark adaptation.[42]
Diagnosis
Over the past decade, it has been recognized that multimodal imaging is essential in the diagnosis of SDD. The imaging characteristics of SDD have been extensively reviewed by other authors.[3,6] Improvement of the diagnostic accuracy of SDD requires confirmation with at least two different imaging modalities. SD-OCT and near infrared reflectance (NIR) have the highest sensitivities [Figures 1 and 2].[21,33,40,43] Confocal blue reflectance, blue channel of CFP, and ICGA have a specificity of 100% but much lower sensitivities.[43]
Figure 1.
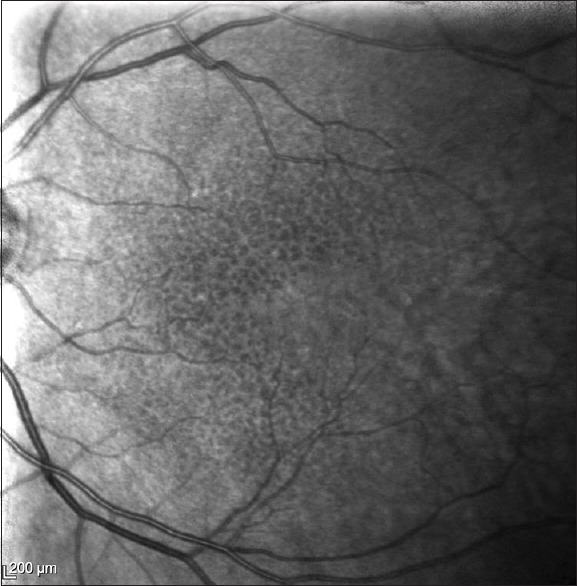
Near infrared reflectance image of an eye with SDD
Figure 2.
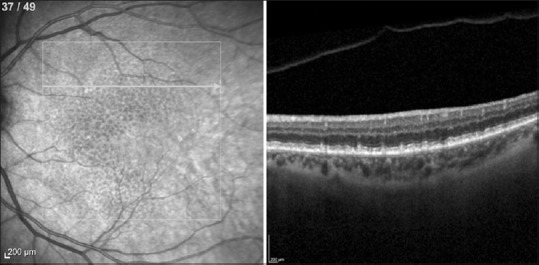
Spectral domain optical coherence tomograpic (SD-OCT) image of an eye with SDD and its corresponding near infrared (NIR) imaging. The horizontal line in the NIR image denotes the level of the SD-OCT scan
Several groups have explored deep learning algorithms to diagnose the presence of SDD from different multimodal images of the posterior pole of the eye.[44,45] van Grinsven et al.[44] built a model that used NIR, CFP, and fundus autofluorescence (FAF) images from the Rotterdam Eye Study. Keenan et al.[45] included CFP and FAF images from the AREDS2 dataset. Both of these studies have shown that deep learning models are not only capable but also exceed the diagnostic capabilities of ophthalmologists. Furthermore, the superior diagnostic properties of FAF over CFP were confirmed. Hu et al.[46] have tried to develop an algorithm to automatically segment SDD from en face OCT images.
Subretinal Drusenoid Deposit Subtypes
Different morphological types of SDD have been described. Multimodal imaging allows characterization of SDD into three different categories: dots, ribbons, and midperipheral.[47] NIR and green FAF are recommended for detecting dots, whereas SLO pseudocolor is more useful for detecting ribbons.[48] SDD subtypes may have different outcomes. Eyes with dot SDD subtype had a 2.5-fold increased risk of developing neovascular AMD (NV-AMD), whereas eyes with ribbon SDD subtype had a 4.3-fold increased risk of developing GA.[49] Adaptive optic SLO has shed some light into the differences between the dot and ribbon subtypes. The characteristic cone mosaic pattern was present in unaffected areas of eyes with dot SDD, whereas this pattern was not present in the unaffected areas of eyes with ribbon SDD. This suggests that in the ribbon SDD subtype, the adjacent areas are not really unaffected and may have undergone some type of outer segment and interdigitation zone degeneration.[50]
Epidemiology
SDDs have been identified in individuals of different ethnic and racial backgrounds, including Korean,[19,24,51] Japanese,[43] Caucasian,[20,37,52] and African-American populations.[20] There appear to be no ethnic differences in populations with SDD.[19] SDD is more prevalent in women and increases with age.[38,53] The reported incidence and prevalence of SDD will vary according to the imaging modality used to detect them.
The classification and risk stratification of AMD have conventionally been based on CFP.[12,54] Although the Wisconsin Age-Related Maculopathy Grading System recognized reticular drusen, it did not discriminate between them from regular soft drusen. The AREDS simplified severity scale did not even acknowledge their presence. Older studies such as the Beaver Dam that used only CFPs are of historical interest since many eyes with SDD will be missed by CFP. Sole reliance on CFP for the detection of SDD will miss 30%–50% of cases.[2] In addition, it is important to note that SDDs are often located outside the central macula, a location that has not been typically screened when assessing AMD severity. Thus, these traditional methods need to be replaced by others that account for the presence of SDD.[53] More recent studies such as the Montrachet and Alienor studies incorporate multimodal imaging in their imaging protocol.[40,55,56] In the Alienor study, the prevalence of SDD using multimodal imaging was 13.4% compared to only 4.5% when using CFP.[40] In the AREDS 2 study, the prevalence of SDD, based on FAF images, was 24% of iAMD eyes or 29% of individuals with iAMD. The prevalence of SDD varied with the baseline AMD severity ranging from 6% in early AMD to 36% in eyes with GA.[53]
Recently, Lei et al.[57] devised a simple scoring system based solely on OCT criteria to assess the risk of progression of eyes with early AMD to late AMD. The OCT criteria included drusen volume within a central 3 mm circle ≥0.3 mm3, intraretinal hyperreflective foci, hyporeflective foci within a drusenoid lesion, and SDD. A point is assigned for the presence of each criterion (maximum risk score of 4 per eye). Then, the points are summed up to obtain a total score, and the risk is assessed by categorization of the total score.[57] Given its novelty, this new risk assessment needs to be validated.
Genetics
Several polymorphisms in the CFH, ARMS2, and C3 genes that have been associated with AMD have also been associated with SDD.[3,6,53] An AMD genetic risk score based on 52 variants was calculated for participants in the AREDS 2 study. Interestingly, as the genetic risk score increased, the prevalence of SDD increased.[53] The association of CFH polymorphisms with SDD has not been consistent. Both the Beaver Dam Eye and Blue Mountain Eye studies, both of which relied on CFP to diagnose SDD, reported that the Y402H polymorphism in the CFH gene was associated with SDD.[37,52] In contrast, other studies that used multimodal imaging have found no association between SDD and polymorphisms in the CFH gene.[23,33,58,59,60,61] A meta-analysis confirmed the lack of association of CFH variants and SDD.[62] ARMS2 risk alleles for AMD, on the other hand, have been strongly associated with SDD.[53,62,63]
Histopathology
Histopathological studies confirm that these SDDs are not benign.[14,64,65] The pseudodrusens were found to be subretinal drusenoid deposits rich in vitronectin that extended into the photoreceptor outer segment and inner nuclear layers. These were associated with photoreceptor disruption, photoreceptor loss, localized Müller cell gliosis, and RPE alterations.[14,64,65] In addition, the choroidal vasculature underlying the SDD areas appeared to be unaltered.[64]
Pathophysiology
The exact mechanisms of development and progression of SDD have not been entirely elucidated, and their understanding has evolved over the years. There is a paucity of longitudinal studies using multimodal imaging. Based on these, the leading hypotheses that have been put forth to explain the pathogenesis of SDD includes choroidal vascular dysfunction,[35] RPE dysfunction or that SDD are para-inflammatory phenomena.[66] SDD and soft drusen are both extracellular deposits that contain similar components such as membranous debris, apoE, complement factor H, vitronectin, and to a lesser extent apoB and apoA-1. The main difference between SDD and soft drusen is the amount of cholesterol esterification. SDD is characterized by the large amount of unesterified cholesterol, whereas in soft drusen, the cholesterol is mostly esterified.[14]
In a recent review, Spaide et al.[3] reported that several investigators used SD-OCT and swept-source (SS)-OCT to demonstrate that SDD are associated with age-related choroidal atrophy, choroidal thinning, and a reduced macular choroidal volume. It appears that these changes in the choroid are driven by changes in the choroidal vasculature. The advent of OCT-angiography (OCTA) allowed several groups to study the choriocapillaris in eyes with SDD. Eyes with SDD manifest a significantly decreased choriocapillaris vessel density and larger areas of choriocapillaris nonperfusion.[67,68] Despite these findings, they emphasized that the mere presence of choroidal thinning was not sufficient to give rise to SDD. They noted that elderly myopic patients despite their extremely thin choroids do not develop SDD.[3] Choriocapillaris ischemia leads to RPE hypoxia.
An increasing body of evidence of histopathological,[69] SS-OCT,[70] and SD-OCT[71,72] studies implicates choroidal vascular dysfunction in the pathogenesis of both AMD and SDD. SDD may be a manifestation of choroidal vascular disease. Some believed that SDD was an ocular marker of cardiovascular disease that led to an impaired choroidal filling.[34] They have noted the association between SDD and multilobular GA,[73] the location of SDD along the choroidal watershed zones,[72] and the association of SDD with choroidal thinning. In the Alienor study, patients with choroidal thickness at baseline were more prone to develop SDD.[56] A cross-sectional study that corrected for confounding variables through a multivariate analysis showed that in eyes with intermediate AMD with SDD, the choroid was attenuated when compared to eyes without SDD.[74] Eyes with SDD have a decreased mean macular choroidal thickness, choroidal vascular thickness, and choroidal vascularity index.[74]
The spatial association between SDD and the choroidal vasculature has been fraught with controversy. On the one hand, several authors claimed that SDDs result from fibrous replacement of the choroidal stroma to outer retina lipid cycling.
Patients with iAMD exhibit a systemic dysregulation of the complement system. However, the complement factor levels were not related to the presence or absence of SDD.[75]
Natural History
SDDs are dynamic structures and undergo changes. A three-stage SD-OCT-based grading system was proposed in 2010.[3,4,6] In Stage 1, granular hyperreflective material was deposited in the interdigitation zone between the RPE and the inner segment/outer segment layer. When mounds of material alter the contour of the ellipsoid line, Stage 2 is reached. In Stage 3, thicker material adopts a conical appearance and breaks through the ellipsoid. Stage 4 was added a few years later to characterize fading of material due to migration and reabsorption within the inner retinal layers.[3,4,6] Spaide[76] recognized that on SDD regression, outer retinal atrophy (ORA), a previously unrecognized form of late AMD, developed. This ORA was characterized by the collapse of the outer nuclear layer, an attenuated ellipsoid zone, thin choroid, and an intact RPE. He differentiated ORA from GA. A histopathological survey and clinicopathological correlation of eyes with SDD confirmed the progression of SDD to ORA on SDD regression.[66] This observation led to recognition of ORA led to Classification of Atrophy Meetings group.
The assessment of the natural history of an individual SDD is challenging.[77] Even the Heidelberg Spectralis has alignment inaccuracies of the confocal scanning laser ophthalmoscope (cSLO) + SD-OCT with an alignment error of up to 35 μm.[78] According to Steinberg et al.,[77] analysis of a single corresponding follow-up scan does not suffice. To minimize these problems, they recommend a very dense OCT volume scan of at least <11 μm between scans coupled to analysis of the neighboring scans.[77] Using this strategy, they reported that in 18 eyes with a median observational time of 5 months, none of the individual SDD disappeared. In contrast, if only the corresponding follow-up scan was used, 21% of the SDD lesions had vanished.
The lifecycle of an individual SDD is more dynamic and does not necessarily progress through the different stages. Recently, Zhang et al.[79] used adaptive optics scanning laser ophthalmoscope (AO-SLO) and SD-OCT to describe the life cycles of individual SDD. They reported that after 12 months of follow-up, in 6 eyes of 4 patients, 69% of the SDD grew, 15% shrank, 6% remained unchanged, 11% disappeared, and 0.6% re-appeared following regression.
Some studies have suggested that microglia may be involved in the regression of SDD.[64] Others have challenged this idea and have stated that there is currently no evidence to suggest that invading phagocytes are involved at all. They instead ascribe it to fluctuations in the activity of surrounding outer retinal cells.[79]
SDD has been recognized as an important risk factor for the progression to the late stages of AMD.[17,59,80] However, these studies involved eyes that also had soft drusen, which introduced a confounding factor since soft drusen are known to be a risk factor for the development of late AMD. Recently, Spaide et al.[81] conducted a longitudinal study of 85 eyes with SDD and no drusen and followed them with multimodal imaging for an average of 5 years. They confirmed that eyes with SDD were at an increased risk of developing MNV and GA. They also noted that 20% of eyes harbored vitelliform lesions at baseline. During follow-up, an additional 8 eyes developed vitelliform lesions and 12 eyes lost the vitelliform lesion. The sequelae from the regression of vitelliform material depended on its amount, location, and size. Larger vitelliform lesions that were often subfoveal developed GA and MNV. In contrast, smaller nonfoveal vitelliform lesions left round hyperpigmented spots that were often surrounded by a hypopigmented halo.[81] These hyperpigmented spots have been associated with the development of MNV, in particular type 3 MNV.[81,82] These patients with vitelliform lesions were excluded from having Best disease and pattern dystrophy by genetic testing for the BEST1 and PRPH 2 genes. The vitelliform lesions may be a marker of RPE dysfunction and an intermediate step in the development of late AMD.[81] As mentioned previously, different SDD subtypes have different outcomes.
Several iAMD phenotypes that predispose to the development of GA, including SDD, large drusen, refractile deposits, pigment epithelial detachments, and vitelliform lesions, were identified. The rates of GA progression were compared among these precursor lesions. Eyes with SDD were associated with the fastest GA enlargement.[83]
Reiter et al.[84] reported that the presence of SDD accelerated the progression of GA, particularly in the superior-temporal and temporal sectors.
Several precursor lesions of GA, including large subretinal pigment epithelial drusen, SDD, refractile deposits, pigment epithelial detachment, and vitelliform lesions, have been identified. Of these, the presence of SDD is associated with the fastest GA enlargement.[83]
Eyes with iAMD and SDD develop progressive outer retinal degeneration, which manifests itself as decreases in scotopic and mesopic retinal sensitivities.[85]
In eyes with exudative NV-AMD, the presence of SDD is an important risk factor for the development of macular atrophy.[86] SDD hastens the GA enlargement rate.[87]
Structural Changes
Enhanced depth imaging (EDI) SD-OCT and SS-OCT have shown that most eyes with SDD have a thinner choroid than iAMD eyes without SDD and age-controlled healthy individuals.[3,6] Sattler's layer has been implicated in one report. In contrast, most recent investigations point to the choriocapillaris. Spaide et al.[3] have emphasized that the choroid is not uniformly thin in eyes with SDD and some patients with SDD have a thick choroid.
EDI SD-OCT images have shown that eyes with SDD and eyes with drusen experienced progressive thinning of the choroid. In contrast, normal control eyes did not experience any choroidal thinning over the same time period. The rate of thinning was similar between luminal and stromal areas; however, overall, the SDD eyes had thinner choroids when compared to the eyes with drusen. In addition, the luminal to total choroidal area ratio was lower, and the stromal to total choroidal area ratio was higher in eyes with SDD than the eyes with drusen and the control eyes.[88] An OCTA comparative analysis of eyes with SDD, eyes with drusen, and eyes with both SDD and drusen and normal controls revealed total choroidal vessel density, choriocapillaris vessel density, Sattler's layer vessel density, and Haller's layer vessel density were all reduced in eyes with SDD. Furthermore, the vessel to stroma ratio at all the choroidal vascular layers was reduced significantly.[89] These findings support the notion that choroidal vascular depletion and fibrotic replacement occurs in eyes with SDD.
Functional Changes
SDD by virtue of their anatomic location overlying the RPE may alter photoreceptor structure and in turn influence retinal function even in early stages.[3,6,90] Histopathological examination of an eye with SDD and non-NV-AMD showed photoreceptors with loss of the inner segment deflection and outer segment shortening.[65] SDDs are most commonly located in the superior macula and surrounding the optic nerve.[3,6] The most severely affected areas were the superior areas and the least affected were the central areas. In eyes with SDD, the functional changes correlated with the physical and topographical distribution of the SDD, which happen to coincide with the topographical distribution of rods.
Several investigators have compared functional parameters such as best-corrected visual acuity, low luminance visual acuity, dark adaptation times, retinal sensitivity between healthy age-controlled eyes, iAMD eyes with SDD, and iAMD eyes without SDD.[3,4,6,91] A recent pilot study suggests that the magnitude of functional losses in eyes with iAMD and SDD are greater than eyes with iAMD without SDD. These losses are similar to those from parafoveal atrophy.[91]
In contrast, Neely et al.[42] reported that SDD in the eyes of older individuals without any other signs of macular pathology do not exhibit any functional deficits.
This preference of SDD toward rods partly explains the results of multifocal electroretinogram (mfERG) on eyes with SDD. Since the main mfERG signals are cone driven, it is not surprising that the presence of SDD did not appear to alter the electrophysiological activity of areas affected by SDD when compared to eyes without SDD.[92] Loss of chromatic sensitivity has been observed in eyes with SDD.[93] Recent studies have shown that cones are affected as well.[93,94]
Treatment
Despite the success of anti-VEGF drugs in the management of NV-AMD, many eyes do not gain or maintain useful vision.[95,96] Eyes with GA have no treatment currently available. Some researchers have reasoned that intervention at the iAMD stage may modify the natural history of the disease.
Subthreshold nanopulsed laser treatment of a mouse model of AMD, characterized by a thickened Bruch's membrane, caused an upregulation of genes involved with turnover of Bruch's membrane extracellular matrix.[97] Some investigators have explored subthreshold nanopulsed laser as a means of slowing the progression of iAMD to late AMD and preventing visual loss.[98,99] At 3 years of follow-up, subthreshold nanosecond laser delivered every 6 months caused a twofold increase in progression in eyes with iAMD and SDD, whereas eyes with iAMD without SDD had a fourfold reduction in progression.[99] A 24-month observational extension of the study confirmed these observations.[100] The mechanism underlying subthreshold nanopulsed laser treatment is not entirely understood but is presumably based on selective photo-thermolysis where the laser pulse leads to RPE loss which triggers a wound healing response. Eyes with SDD may be so damaged that they are unable to heal and instead the laser pulse hastens their demise.[100]
The PASCAL-GA trial is an ongoing single-center, nonrandomized, phase I–II pilot study that aims to assess if subthreshold laser can restore the RPE function in eyes with SDD and incipient GA. Power titration was performed to obtain a barely visible threshold burn. Eyes were treated with end point management consisting of 30% of the power required to obtain the barely visible threshold burn with a pattern of 5 × 3 spots (1.27 mm2 area). The treatment area was selected within the vascular arcades but outside the fovea.[98] Results at 3 months of follow-up demonstrated SDD stage regression and outer nuclear layer thickening in the areas of treatment.[101]
Patients with iAMD and SDD exhibit significantly reduced macular pigment optical density when compared to control subjects and patients with iAMD featuring intermediate and large drusen. Following a 3-month supplementation of lutein and zeaxanthin, the macular pigment optical density (MPOD) in the SDD eyes improved, but the best corrected visual acuity (BCVA) and the retinal sensitivity, as measured by microperimetry, remained unchanged.[102]
Future treatment trials of iAMD need to phenotypically stratify eyes according to the presence or absence of SDD. As illustrated by the LEAD study, treatment outcomes may differ depending on the presence or absence of SDD.[99,100,103] Eyes with SDD may be irreversibly committed to undergo disease progression.
Summary
SDDs are extracellular deposits located in the subretinal space. They differ in content from drusen by having more esterified cholesterol. SDDs have a predilection for perifoveal rod-rich areas in contrast to soft drusen that preferentially appears in the cone-rich fovea. IR reflectance and SD-OCT are the preferred methods of diagnosis. The presence of SDD may be a poor prognostic sign for eyes with iAMD and may signify irreversible disease progression to the development of late forms of AMD such as GA, type 3 MNV, and ORA.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors declare that there are no conflicts of interests of this paper.
References
- 1.Marsiglia M, Boddu S, Bearelly S, Xu L, Breaux BE, Jr, Freund KB, et al. Association between geographic atrophy progression and reticular pseudodrusen in eyes with dry age-related macular degeneration. Invest Ophthalmol Vis Sci. 2013;54:7362–9. doi: 10.1167/iovs.12-11073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Steinberg JS, Göbel AP, Fleckenstein M, Holz FG, Schmitz-Valckenberg S. Reticular drusen in eyes with high-risk characteristics for progression to late-stage age-related macular degeneration. Br J Ophthalmol. 2015;99:1289–94. doi: 10.1136/bjophthalmol-2014-306535. [DOI] [PubMed] [Google Scholar]
- 3.Spaide RF, Ooto S, Curcio CA. Subretinal drusenoid deposits AKA pseudodrusen. Surv Ophthalmol. 2018;63:782–815. doi: 10.1016/j.survophthal.2018.05.005. [DOI] [PubMed] [Google Scholar]
- 4.Wightman AJ, Guymer RH. Reticular pseudodrusen: Current understanding. Clin Exp Optom. 2019;102:455–62. doi: 10.1111/cxo.12842. [DOI] [PubMed] [Google Scholar]
- 5.Rabiolo A, Sacconi R, Cicinelli MV, Querques L, Bandello F, Querques G. Spotlight on reticular pseudodrusen. Clin Ophthalmol. 2017;11:1707–18. doi: 10.2147/OPTH.S130165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sivaprasad S, Bird A, Nitiahpapand R, Nicholson L, Hykin P, Chatziralli I, et al. Perspectives on reticular pseudodrusen in age-related macular degeneration. Surv Ophthalmol. 2016;61:521–37. doi: 10.1016/j.survophthal.2016.02.005. [DOI] [PubMed] [Google Scholar]
- 7.Alten F, Eter N. Current knowledge on reticular pseudodrusen in age-related macular degeneration. Br J Ophthalmol. 2015;99:717–22. doi: 10.1136/bjophthalmol-2014-305339. [DOI] [PubMed] [Google Scholar]
- 8.de Jong PT. A historical analysis of the quest for the origins of aging macula disorder, the tissues involved, and its terminology. Ophthalmol Eye Dis. 2016;8:5–14. doi: 10.4137/OED.S40523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gass JD. Drusen and disciform macular detachment and degeneration. Trans Am Ophthalmol Soc. 1972;70:409–36. [PMC free article] [PubMed] [Google Scholar]
- 10.Mimoun G, Soubrane G, Coscas G. Macular drusen. J Fr Ophtalmol. 1990;13:511–30. [PubMed] [Google Scholar]
- 11.Spaide RF, Curcio CA. Drusen characterization with multimodal imaging. Retina. 2010;30:1441–54. doi: 10.1097/IAE.0b013e3181ee5ce8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Klein R, Davis MD, Magli YL, Segal P, Klein BE, Hubbard L. The Wisconsin age-related maculopathy grading system. Ophthalmology. 1991;98:1128–34. doi: 10.1016/s0161-6420(91)32186-9. [DOI] [PubMed] [Google Scholar]
- 13.Arnold JJ, Sarks SH, Killingsworth MC, Sarks JP. Reticular pseudodrusen. A risk factor in age-related maculopathy. Retina. 1995;15:183–91. [PubMed] [Google Scholar]
- 14.Rudolf M, Malek G, Messinger JD, Clark ME, Wang L, Curcio CA. Sub-retinal drusenoid deposits in human retina: Organization and composition. Exp Eye Res. 2008;87:402–8. doi: 10.1016/j.exer.2008.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zweifel SA, Spaide RF, Curcio CA, Malek G, Imamura Y. Reticular pseudodrusen are subretinal drusenoid deposits. Ophthalmology. 2010(117):303–12.e1. doi: 10.1016/j.ophtha.2009.07.014. [DOI] [PubMed] [Google Scholar]
- 16.Schmitz-Valckenberg S, Steinberg JS, Fleckenstein M, Visvalingam S, Brinkmann CK, Holz FG. Combined confocal scanning laser ophthalmoscopy and spectral-domain optical coherence tomography imaging of reticular drusen associated with age-related macular degeneration. Ophthalmology. 2010;117:1169–76. doi: 10.1016/j.ophtha.2009.10.044. [DOI] [PubMed] [Google Scholar]
- 17.Cohen SY, Dubois L, Tadayoni R, Delahaye-Mazza C, Debibie C, Quentel G. Prevalence of reticular pseudodrusen in age-related macular degeneration with newly diagnosed choroidal neovascularisation. Br J Ophthalmol. 2007;91:354–9. doi: 10.1136/bjo.2006.101022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sarks J, Arnold J, Ho IV, Sarks S, Killingsworth M. Evolution of reticular pseudodrusen. Br J Ophthalmol. 2011;95:979–85. doi: 10.1136/bjo.2010.194977. [DOI] [PubMed] [Google Scholar]
- 19.Lee MY, Yoon J, Ham DI. Clinical characteristics of reticular pseudodrusen in Korean patients. Am J Ophthalmol. 2012;153:530–5. doi: 10.1016/j.ajo.2011.08.012. [DOI] [PubMed] [Google Scholar]
- 20.Zarubina AV, Neely DC, Clark ME, Huisingh CE, Samuels BC, Zhang Y, et al. Prevalence of subretinal drusenoid deposits in older persons with and without age-related macular degeneration, by multimodal imaging. Ophthalmology. 2016;123:1090–100. doi: 10.1016/j.ophtha.2015.12.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.De Bats F, Mathis T, Mauget-Faÿsse M, Joubert F, Denis P, Kodjikian L. Prevalence of reticular pseudodrusen in age-related macular degeneration using multimodal imaging. Retina. 2016;36:46–52. doi: 10.1097/IAE.0000000000000648. [DOI] [PubMed] [Google Scholar]
- 22.Mathis T, De Bats F, Mauget-Faÿsse M, Denis P, Kodjikian L. Re: Zarubina et al.: Prevalence of subretinal drusenoid deposits in older persons with and without age-related macular degeneration, by multimodal imaging (Ophthalmology 2016;123:1090-1100) Ophthalmology. 2017;124:e19–20. doi: 10.1016/j.ophtha.2016.05.014. [DOI] [PubMed] [Google Scholar]
- 23.Ueda-Arakawa N, Ooto S, Nakata I, Yamashiro K, Tsujikawa A, Oishi A, et al. Prevalence and genomic association of reticular pseudodrusen in age-related macular degeneration. Am J Ophthalmol. 2013;155:260–9.e2. doi: 10.1016/j.ajo.2012.08.011. [DOI] [PubMed] [Google Scholar]
- 24.Kim JH, Chang YS, Kim JW, Lee TG, Kim CG. Prevalence of subtypes of reticular pseudodrusen in newly diagnosed exudative age-related macular degeneration and polypoidal choroidal vasculopathy in Korean patients. Retina. 2015;35:2604–12. doi: 10.1097/IAE.0000000000000633. [DOI] [PubMed] [Google Scholar]
- 25.Gliem M, Hendig D, Finger RP, Holz FG, Charbel Issa P. Reticular pseudodrusen associated with a diseased bruch membrane in pseudoxanthoma elasticum. JAMA Ophthalmol. 2015;133:581–8. doi: 10.1001/jamaophthalmol.2015.117. [DOI] [PubMed] [Google Scholar]
- 26.Zweifel SA, Imamura Y, Freund KB, Spaide RF. Multimodal fundus imaging of pseudoxanthoma elasticum. Retina. 2011;31:482–91. doi: 10.1097/IAE.0b013e3181f056ce. [DOI] [PubMed] [Google Scholar]
- 27.Gliem M, Müller PL, Mangold E, Bolz HJ, Stöhr H, Weber BH, et al. Reticular pseudodrusen in sorsby fundus dystrophy. Ophthalmology. 2015;122:1555–62. doi: 10.1016/j.ophtha.2015.04.035. [DOI] [PubMed] [Google Scholar]
- 28.Lally DR, Baumal C. Subretinal drusenoid deposits associated with complement-mediated IgA nephropathy. JAMA Ophthalmol. 2014;132:775–7. doi: 10.1001/jamaophthalmol.2014.387. [DOI] [PubMed] [Google Scholar]
- 29.Aleman TS, Garrity ST, Brucker AJ. Retinal structure in vitamin A deficiency as explored with multimodal imaging. Doc Ophthalmol. 2013;127:239–43. doi: 10.1007/s10633-013-9403-0. [DOI] [PubMed] [Google Scholar]
- 30.Genead MA, Fishman GA, Lindeman M. Spectral-domain optical coherence tomography and fundus autofluorescence characteristics in patients with fundus albipunctatus and retinitis punctata albescens. Ophthalmic Genet. 2010;31:66–72. doi: 10.3109/13816810903584971. [DOI] [PubMed] [Google Scholar]
- 31.Wilde C, Lakshmanan A, Patel M, Morales MU, Dhar-Munshi S, Amoaku WM. Prevalence of reticular pseudodrusen in newly presenting adult onset foveomacular vitelliform dystrophy. Eye (Lond) 2016;30:817–24. doi: 10.1038/eye.2016.46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Boon CJ, Theelen T, Hoyng CB. Extensive macular atrophy with pseudodrusen-like appearance: A new clinical entity. Am J Ophthalmol. 2009;148:173–4. doi: 10.1016/j.ajo.2009.03.017. [DOI] [PubMed] [Google Scholar]
- 33.Smith RT, Sohrab MA, Busuioc M, Barile G. Reticular macular disease. Am J Ophthalmol. 2009;148:733–43.e2. doi: 10.1016/j.ajo.2009.06.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rastogi N, Smith RT. Association of age-related macular degeneration and reticular macular disease with cardiovascular disease. Surv Ophthalmol. 2016;61:422–33. doi: 10.1016/j.survophthal.2015.10.003. [DOI] [PubMed] [Google Scholar]
- 35.Leisy HB, Ahmad M, Marmor M, Smith RT. Association between decreased renal function and reticular macular disease in age-related macular degeneration. Ophthalmol Retina. 2017;1:42–8. doi: 10.1016/j.oret.2016.08.011. [DOI] [PubMed] [Google Scholar]
- 36.Otero-Marquez O, Chung H, Lee CS, Choi EY, Ledesma-Gil G, Alauddin S, et al. Subretinal deposits in pre-eclampsia and malignant hypertension: Implications for age-related macular degeneration. Ophthalmol Retina. 2021;5:750–60. doi: 10.1016/j.oret.2020.10.018. [DOI] [PubMed] [Google Scholar]
- 37.Klein R, Meuer SM, Knudtson MD, Iyengar SK, Klein BE. The epidemiology of retinal reticular drusen. Am J Ophthalmol. 2008;145:317–26. doi: 10.1016/j.ajo.2007.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Finger RP, Chong E, McGuinness MB, Robman LD, Aung KZ, Giles G, et al. Reticular pseudodrusen and their association with age-related macular degeneration: The Melbourne collaborative cohort study. Ophthalmology. 2016;123:599–608. doi: 10.1016/j.ophtha.2015.10.029. [DOI] [PubMed] [Google Scholar]
- 39.Rabiolo A, Benatti L, Tomasso L, Zucchiatti I, Gelormini F, Casaluci M, et al. Retinal arterial dilation is impaired in eyes with drusen and reticular pseudodrusen. Retina. 2019;39:2205–11. doi: 10.1097/IAE.0000000000002283. [DOI] [PubMed] [Google Scholar]
- 40.Chan H, Cougnard-Grégoire A, Delyfer MN, Combillet F, Rougier MB, Schweitzer C, et al. Multimodal imaging of reticular pseudodrusen in a population-based setting: The Alienor study. Invest Ophthalmol Vis Sci. 2016;57:3058–65. doi: 10.1167/iovs.16-19487. [DOI] [PubMed] [Google Scholar]
- 41.Cleland SC, Domalpally A, Liu Z, Pak JW, Blodi BA, Bailey S, et al. Reticular pseudodrusen characteristics and associations in the carotenoids in age-related eye disease study 2 (CAREDS2), an ancillary study of the women's health initiative. Ophthalmol Retina. 2021;5:721–9. doi: 10.1016/j.oret.2020.12.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Neely D, Zarubina AV, Clark ME, Huisingh CE, Jackson GR, Zhang Y, et al. Association between visual function and subretinal drusenoid deposits in normal and early age-related macular degeneration eyes. Retina. 2017;37:1329–36. doi: 10.1097/IAE.0000000000001454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ueda-Arakawa N, Ooto S, Tsujikawa A, Yamashiro K, Oishi A, Yoshimura N. Sensitivity and specificity of detecting reticular pseudodrusen in multimodal imaging in Japanese patients. Retina. 2013;33:490–7. doi: 10.1097/IAE.0b013e318276e0ae. [DOI] [PubMed] [Google Scholar]
- 44.van Grinsven MJ, Buitendijk GH, Brussee C, van Ginneken B, Hoyng CB, Theelen T, et al. Automatic identification of reticular pseudodrusen using multimodal retinal image analysis. Invest Ophthalmol Vis Sci. 2015;56:633–9. doi: 10.1167/iovs.14-15019. [DOI] [PubMed] [Google Scholar]
- 45.Keenan TD, Chen Q, Peng Y, Domalpally A, Agrón E, Hwang CK, et al. Deep learning automated detection of reticular pseudodrusen from fundus autofluorescence images or color fundus photographs in AREDS2. Ophthalmology. 2020;127:1674–87. doi: 10.1016/j.ophtha.2020.05.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hu Z, Shi Y, Nandanan K, Sadda SR APGS Study Group. Semiautomated segmentation and analysis of retinal layers in three-dimensional spectral-domain optical coherence tomography images of patients with atrophic age-related macular degeneration. Neurophotonics. 2017;4:011012. doi: 10.1117/1.NPh.4.1.011012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Suzuki M, Sato T, Spaide RF. Pseudodrusen subtypes as delineated by multimodal imaging of the fundus. Am J Ophthalmol. 2014;157:1005–12. doi: 10.1016/j.ajo.2014.01.025. [DOI] [PubMed] [Google Scholar]
- 48.Cozzi M, Monteduro D, Parrulli S, Corvi F, Zicarelli F, Corradetti G, et al. Sensitivity and specificity of multimodal imaging in characterizing drusen. Ophthalmol Retina. 2020;4:987–95. doi: 10.1016/j.oret.2020.04.013. [DOI] [PubMed] [Google Scholar]
- 49.Zhou Q, Daniel E, Maguire MG, Grunwald JE, Martin ER, Martin DF, et al. Pseudodrusen and incidence of late age-related macular degeneration in fellow eyes in the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2016;123:1530–40. doi: 10.1016/j.ophtha.2016.02.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Xu X, Wang X, Sadda SR, Zhang Y. Subtype-differentiated impacts of subretinal drusenoid deposits on photoreceptors revealed by adaptive optics scanning laser ophthalmoscopy. Graefes Arch Clin Exp Ophthalmol. 2020;258:1931–40. doi: 10.1007/s00417-020-04774-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Erdogan E, Sakarya R, Sakarya Y, Ozcimen M, Goktas S. Clinical characteristics of reticular pseudodrusen in Korean patients. Am J Ophthalmol. 2014;157:261. doi: 10.1016/j.ajo.2013.09.030. [DOI] [PubMed] [Google Scholar]
- 52.Joachim N, Mitchell P, Rochtchina E, Tan AG, Wang JJ. Incidence and progression of reticular drusen in age-related macular degeneration: Findings from an older Australian cohort. Ophthalmology. 2014;121:917–25. doi: 10.1016/j.ophtha.2013.10.043. [DOI] [PubMed] [Google Scholar]
- 53.Domalpally A, Agrón E, Pak JW, Keenan TD, Ferris FL, 3rd, Clemons TE, et al. Prevalence, risk, and genetic association of reticular pseudodrusen in age-related macular degeneration: Age-related eye disease study 2 report 21. Ophthalmology. 2019;126:1659–66. doi: 10.1016/j.ophtha.2019.07.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Ferris FL, 3rd, Wilkinson CP, Bird A, Chakravarthy U, Chew E, Csaky K, et al. Clinical classification of age-related macular degeneration. Ophthalmology. 2013;120:844–51. doi: 10.1016/j.ophtha.2012.10.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gabrielle PH, Seydou A, Arnould L, Acar N, Devilliers H, Baudin F, et al. Subretinal drusenoid deposits in the elderly in a population-based study (the Montrachet study) Invest Ophthalmol Vis Sci. 2019;60:4838–48. doi: 10.1167/iovs.19-27283. [DOI] [PubMed] [Google Scholar]
- 56.Dutheil C, Le Goff M, Cougnard-Grégoire A, Gattoussi S, Korobelnik JF, Rougier MB, et al. Incidence and risk factors of reticular pseudodrusen using multimodal imaging. JAMA Ophthalmol. 2020;138:467–77. doi: 10.1001/jamaophthalmol.2020.0266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Lei J, Balasubramanian S, Abdelfattah NS, Nittala MG, Sadda SR. Proposal of a simple optical coherence tomography-based scoring system for progression of age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2017;255:1551–8. doi: 10.1007/s00417-017-3693-y. [DOI] [PubMed] [Google Scholar]
- 58.Boddu S, Lee MD, Marsiglia M, Marmor M, Freund KB, Smith RT. Risk factors associated with reticular pseudodrusen versus large soft drusen. Am J Ophthalmol. 2014;157:985–93.e2. doi: 10.1016/j.ajo.2014.01.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Pumariega NM, Smith RT, Sohrab MA, Letien V, Souied EH. A prospective study of reticular macular disease. Ophthalmology. 2011;118:1619–25. doi: 10.1016/j.ophtha.2011.01.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Smith RT, Merriam JE, Sohrab MA, Pumariega NM, Barile G, Blonska AM, et al. Complement factor H 402H variant and reticular macular disease. Arch Ophthalmol. 2011;129:1061–6. doi: 10.1001/archophthalmol.2011.212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Puche N, Blanco-Garavito R, Richard F, Leveziel N, Zerbib J, Tilleul J, et al. Genetic and environmental factors associated with reticular pseudodrusen in age-related macular degeneration. Retina. 2013;33:998–1004. doi: 10.1097/IAE.0b013e31827b6483. [DOI] [PubMed] [Google Scholar]
- 62.Jabbarpoor Bonyadi MH, Yaseri M, Nikkhah H, Bonyadi M, Soheilian M. Association of risk genotypes of ARMS2/LOC387715 A69S and CFH Y402H with age-related macular degeneration with and without reticular pseudodrusen: A meta-analysis. Acta Ophthalmol. 2018;96:e105–10. doi: 10.1111/aos.13494. [DOI] [PubMed] [Google Scholar]
- 63.Lin LY, Zhou Q, Hagstrom S, Maguire MG, Daniel E, Grunwald JE, et al. Association of single-nucleotide polymorphisms in age-related macular degeneration with pseudodrusen: Secondary analysis of data from the comparison of AMD treatments trials. JAMA Ophthalmol. 2018;136:682–8. doi: 10.1001/jamaophthalmol.2018.1231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Greferath U, Guymer RH, Vessey KA, Brassington K, Fletcher EL. Correlation of histologic features with in vivo imaging of reticular pseudodrusen. Ophthalmology. 2016;123:1320–31. doi: 10.1016/j.ophtha.2016.02.009. [DOI] [PubMed] [Google Scholar]
- 65.Curcio CA, Messinger JD, Sloan KR, McGwin G, Medeiros NE, Spaide RF. Subretinal drusenoid deposits in non-neovascular age-related macular degeneration: Morphology, prevalence, topography, and biogenesis model. Retina. 2013;33:265–76. doi: 10.1097/IAE.0b013e31827e25e0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Chen L, Messinger JD, Zhang Y, Spaide RF, Freund KB, Curcio CA. Subretinal drusenoid deposit in age-related macular degeneration: Histologic insights into initiation, progression to atrophy, and imaging. Retina. 2020;40:618–31. doi: 10.1097/IAE.0000000000002657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Alten F, Heiduschka P, Clemens CR, Eter N. Exploring choriocapillaris under reticular pseudodrusen using OCT-Angiography. Graefes Arch Clin Exp Ophthalmol. 2016;254:2165–73. doi: 10.1007/s00417-016-3375-1. [DOI] [PubMed] [Google Scholar]
- 68.Nesper PL, Soetikno BT, Fawzi AA. Choriocapillaris nonperfusion is associated with poor visual acuity in eyes with reticular pseudodrusen. Am J Ophthalmol. 2017;174:42–55. doi: 10.1016/j.ajo.2016.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Mullins RF, Johnson MN, Faidley EA, Skeie JM, Huang J. Choriocapillaris vascular dropout related to density of drusen in human eyes with early age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52:1606–12. doi: 10.1167/iovs.10-6476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Ueda-Arakawa N, Ooto S, Ellabban AA, Takahashi A, Oishi A, Tamura H, et al. Macular choroidal thickness and volume of eyes with reticular pseudodrusen using swept-source optical coherence tomography. Am J Ophthalmol. 2014;157:994–1004. doi: 10.1016/j.ajo.2014.01.018. [DOI] [PubMed] [Google Scholar]
- 71.Grewal DS, Chou J, Rollins SD, Fawzi AA. A pilot quantitative study of topographic correlation between reticular pseudodrusen and the choroidal vasculature using en face optical coherence tomography. PLoS One. 2014;9:e92841. doi: 10.1371/journal.pone.0092841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Alten F, Clemens CR, Heiduschka P, Eter N. Localized reticular pseudodrusen and their topographic relation to choroidal watershed zones and changes in choroidal volumes. Invest Ophthalmol Vis Sci. 2013;54:3250–7. doi: 10.1167/iovs.13-11923. [DOI] [PubMed] [Google Scholar]
- 73.Xu L, Blonska AM, Pumariega NM, Bearelly S, Sohrab MA, Hageman GS, et al. Reticular macular disease is associated with multilobular geographic atrophy in age-related macular degeneration. Retina. 2013;33:1850–62. doi: 10.1097/IAE.0b013e31828991b2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Keenan TD, Klein B, Agrón E, Chew EY, Cukras CA, Wong WT. Choroidal thickness and vascularity vary with disease severity and subretinal drusenoid deposit presence in nonadvanced age-related macular degeneration. Retina. 2020;40:632–42. doi: 10.1097/IAE.0000000000002434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Lynch AM, Palestine AG, Wagner BD, Patnaik JL, Frazier-Abel AA, Mathias MT, et al. Complement factors and reticular pseudodrusen in intermediate age-related macular degeneration staged by multimodal imaging. BMJ Open Ophthalmol. 2020;5:e000361. doi: 10.1136/bmjophth-2019-000361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Spaide RF. Outer retinal atrophy after regression of subretinal drusenoid deposits as a newly recognized form of late age-related macular degeneration. Retina. 2013;33:1800–8. doi: 10.1097/IAE.0b013e31829c3765. [DOI] [PubMed] [Google Scholar]
- 77.Steinberg JS, Auge J, Fleckenstein M, Holz FG, Schmitz-Valckenberg S. Longitudinal analysis of reticular drusen associated with age-related macular degeneration using combined confocal scanning laser ophthalmoscopy and spectral-domain optical coherence tomography imaging. Ophthalmologica. 2015;233:35–42. doi: 10.1159/000368168. [DOI] [PubMed] [Google Scholar]
- 78.Barteselli G, Bartsch DU, Viola F, Mojana F, Pellegrini M, Hartmann KI, et al. Accuracy of the Heidelberg Spectralis in the alignment between near-infrared image and tomographic scan in a model eye: A multicenter study. Am J Ophthalmol. 2013;156:588–92. doi: 10.1016/j.ajo.2013.04.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Zhang Y, Wang X, Sadda SR, Clark ME, Witherspoon CD, Spaide RF, et al. Lifecycles of individual subretinal drusenoid deposits and evolution of outer retinal atrophy in age-related macular degeneration. Ophthalmol Retina. 2020;4:274–83. doi: 10.1016/j.oret.2019.10.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Zweifel SA, Imamura Y, Spaide TC, Fujiwara T, Spaide RF. Prevalence and significance of subretinal drusenoid deposits (reticular pseudodrusen) in age-related macular degeneration. Ophthalmology. 2010;117:1775–81. doi: 10.1016/j.ophtha.2010.01.027. [DOI] [PubMed] [Google Scholar]
- 81.Spaide RF, Yannuzzi L, Freund KB, Mullins R, Stone E. Eyes with subretinal drusenoid deposits and no drusen: Progression of macular findings. Retina. 2019;39:12–26. doi: 10.1097/IAE.0000000000002362. [DOI] [PubMed] [Google Scholar]
- 82.Spaide RF. Fundus autofluorescence and age-related macular degeneration. Ophthalmology. 2003;110:392–9. doi: 10.1016/S0161-6420(02)01756-6. [DOI] [PubMed] [Google Scholar]
- 83.Thiele S, Nadal J, Pfau M, Saßmannshausen M, Fleckenstein M, Holz FG, et al. Prognostic value of intermediate age-related macular degeneration phenotypes for geographic atrophy progression. Br J Ophthalmol. 2021;105:239–45. doi: 10.1136/bjophthalmol-2020-316004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Reiter GS, Told R, Schranz M, Baumann L, Mylonas G, Sacu S, et al. Subretinal drusenoid deposits and photoreceptor loss detecting global and local progression of geographic atrophy by SD-OCT imaging. Invest Ophthalmol Vis Sci. 2020;61:11. doi: 10.1167/iovs.61.6.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Sassmannshausen M, Pfau M, Thiele S, Fimmers R, Steinberg JS, Fleckenstein M, et al. Longitudinal analysis of structural and functional changes in presence of reticular pseudodrusen associated with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2020;61:19. doi: 10.1167/iovs.61.10.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Sadda SR, Abdelfattah NS, Lei J, Shi Y, Marion KM, Morgenthien E, et al. Spectral-domain OCT analysis of risk factors for macular atrophy development in the HARBOR study for neovascular age-related macular degeneration. Ophthalmology. 2020;127:1360–70. doi: 10.1016/j.ophtha.2020.03.031. [DOI] [PubMed] [Google Scholar]
- 87.Holmen IC, Aul B, Pak JW, Trane RM, Blodi B, Klein M, et al. Precursors and development of geographic atrophy with autofluorescence imaging: Age-related eye disease study 2 report number 18. Ophthalmol Retina. 2019;3:724–33. doi: 10.1016/j.oret.2019.04.011. [DOI] [PubMed] [Google Scholar]
- 88.Corvi F, Souied EH, Capuano V, Costanzo E, Benatti L, Querques L, et al. Choroidal structure in eyes with drusen and reticular pseudodrusen determined by binarisation of optical coherence tomographic images. Br J Ophthalmol. 2017;101:348–52. doi: 10.1136/bjophthalmol-2016-308548. [DOI] [PubMed] [Google Scholar]
- 89.Cicinelli MV, Rabiolo A, Marchese A, de Vitis L, Carnevali A, Querques L, et al. Choroid morphometric analysis in non-neovascular age-related macular degeneration by means of optical coherence tomography angiography. Br J Ophthalmol. 2017;101:1193–200. doi: 10.1136/bjophthalmol-2016-309481. [DOI] [PubMed] [Google Scholar]
- 90.Leal C, De Bats F, Morales M, Decullier E, Denis P, Amoaku W, et al. Anatomical-functional concordance of microperimetry and the simplified age-related macular degeneration study classification: A pilot study. Eur J Ophthalmol. 2022;32:402–9. doi: 10.1177/1120672121999348. [DOI] [PubMed] [Google Scholar]
- 91.Grewal MK, Chandra S, Gurudas S, Rasheed R, Sen P, Menon D, et al. Functional clinical endpoints and their correlations in eyes with AMD with and without subretinal drusenoid deposits – A pilot study. Eye (Lond) 2022;36:398–406. doi: 10.1038/s41433-021-01488-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Alten F, Heiduschka P, Clemens CR, Eter N. Multifocal electroretinography in eyes with reticular pseudodrusen. Invest Ophthalmol Vis Sci. 2012;53:6263–70. doi: 10.1167/iovs.12-10094. [DOI] [PubMed] [Google Scholar]
- 93.Vemala R, Sivaprasad S, Barbur JL. Detection of early loss of color vision in age-related macular degeneration – With emphasis on drusen and reticular pseudodrusen. Invest Ophthalmol Vis Sci. 2017;58:O247–54. doi: 10.1167/iovs.17-21771. [DOI] [PubMed] [Google Scholar]
- 94.Mrejen S, Sato T, Curcio CA, Spaide RF. Assessing the cone photoreceptor mosaic in eyes with pseudodrusen and soft drusen in vivo using adaptive optics imaging. Ophthalmology. 2014;121:545–51. doi: 10.1016/j.ophtha.2013.09.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Nguyen V, Barthelmes D, Gillies MC. Neovascular age-related macular degeneration: A review of findings from the real-world Fight Retinal Blindness! registry. Clin Exp Ophthalmol. 2021;49:652–63. doi: 10.1111/ceo.13949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Arevalo JF, Lasave AF, Wu L, Acón D, Berrocal MH, Diaz-Llopis M, et al. Intravitreal bevacizumab for choroidal neovascularization in age-related macular degeneration: 5-year results of the Pan-American collaborative retina study group. Retina. 2016;36:859–67. doi: 10.1097/IAE.0000000000000827. [DOI] [PubMed] [Google Scholar]
- 97.Jobling AI, Guymer RH, Vessey KA, Greferath U, Mills SA, Brassington KH, et al. Nanosecond laser therapy reverses pathologic and molecular changes in age-related macular degeneration without retinal damage. FASEB J. 2015;29:696–710. doi: 10.1096/fj.14-262444. [DOI] [PubMed] [Google Scholar]
- 98.Querques G, Cicinelli MV, Rabiolo A, de Vitis L, Sacconi R, Querques L, et al. Laser photocoagulation as treatment of non-exudative age-related macular degeneration: State-of-the-art and future perspectives. Graefes Arch Clin Exp Ophthalmol. 2018;256:1–9. doi: 10.1007/s00417-017-3848-x. [DOI] [PubMed] [Google Scholar]
- 99.Guymer RH, Wu Z, Hodgson LA, Caruso E, Brassington KH, Tindill N, et al. Subthreshold nanosecond laser intervention in age-related macular degeneration: The LEAD randomized controlled clinical trial. Ophthalmology. 2019;126:829–38. doi: 10.1016/j.ophtha.2018.09.015. [DOI] [PubMed] [Google Scholar]
- 100.Guymer RH, Chen FK, Hodgson LA, Caruso E, Harper CA, Wickremashinghe SS, et al. Subthreshold nanosecond laser in age-related macular degeneration: Observational extension study of the LEAD clinical trial. Ophthalmol Retina. 2021;5:1196–203. doi: 10.1016/j.oret.2021.02.015. [DOI] [PubMed] [Google Scholar]
- 101.Querques G, Sacconi R, Gelormini F, Borrelli E, Prascina F, Zucchiatti I, et al. Subthreshold laser treatment for reticular pseudodrusen secondary to age-related macular degeneration. Sci Rep. 2021;11:2193. doi: 10.1038/s41598-021-81810-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Corvi F, Souied EH, Falfoul Y, Georges A, Jung C, Querques L, et al. Pilot evaluation of short-term changes in macular pigment and retinal sensitivity in different phenotypes of early age-related macular degeneration after carotenoid supplementation. Br J Ophthalmol. 2017;101:770–3. doi: 10.1136/bjophthalmol-2016-309115. [DOI] [PubMed] [Google Scholar]
- 103.Wu Z, Luu CD, Hodgson LA, Caruso E, Brassington KH, Tindill N, et al. Secondary and exploratory outcomes of the subthreshold nanosecond laser intervention randomized trial in age-related macular degeneration: A LEAD study report. Ophthalmol Retina. 2019;3:1026–34. doi: 10.1016/j.oret.2019.07.008. [DOI] [PubMed] [Google Scholar]