
Figure 1. Mitral Apparatus Ischemia and Infarction in Relation to ≥Moderate FMR.
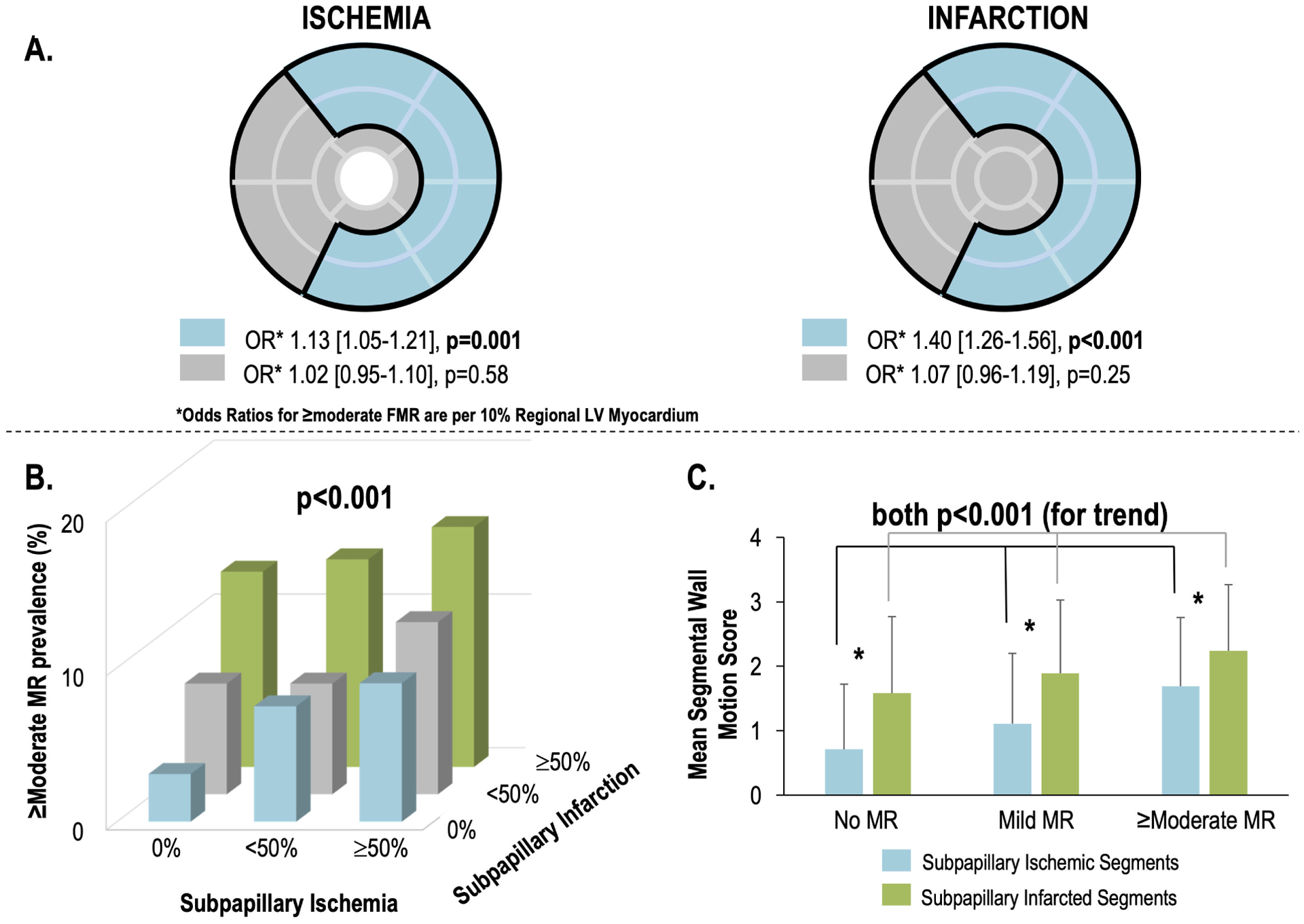
1A. Bullseye plot (17-segment model) illustrating LV myocardium subtended within the mitral apparatus, which was defined (concordant with an established algorithm)(2,18) as encompassing segments adjacent to the anterolateral and posteromedial papillary muscles (blue denotes sub-papillary regions [basal-mid anterior/anterolateral, inferior/inferolateral walls], grey denotes remote LV regions).
Note that sub-papillary ischemia (left) was associated with ≥moderate FMR (p=0.001) controlling for ischemia in remote regions (p=NS). Similarly sub-papillary infarction (right) was associated with ≥moderate FMR (p<0.001) controlling for infarction in remote regions (p=NS).
1B. Prevalence of ≥moderate FMR in relation to strata of sub-papillary ischemia (absent, <50%, ≥50% of segments with stress perfusion deficits) and infarction (absent, <50%, ≥50% of segments with late gadolinium enhancement). As shown, ≥moderate FMR prevalence increased in relation to extent of each sub-papillary tissue alteration (p<0.001 for logistic regression model).
1C. Sub-papillary mean wall motion scores (mean ± standard deviation) among ischemic (blue) and infarcted segments in patients stratified based on presence and severity of FMR (data reported as mean ± standard deviation across all LV sub-papillary segments as illustrated in 1A). Note that for both ischemia and infarction, mean sub-papillary wall motion scores increased in proportion to FMR severity (both p<0.001 for trend), but that contractile dysfunction as discerned by wall motion score was greater for infarcted compared to ischemic segments within each FMR stratum (asterisk refers to p<0.001 for each comparison). All analyses performed in full study cohort (n=2647).