

Abstract
Aim
We evaluated gastrointestinal (GI) adverse events (AEs) with once‐weekly semaglutide 2.4 mg in adults with overweight or obesity and their contribution to weight loss (WL).
Materials and methods
AE analyses pooled data from the Semaglutide Treatment Effect in People With Obesity (STEP) 1‐3 trials for participants randomized to 68 weeks of semaglutide 2.4 mg (n = 2117) or placebo (n = 1262). WL was analysed by presence/absence of GI AEs. Mediation analysis estimated WL effects mediated by and unrelated to GI AEs. GI tolerability with semaglutide 2.4 mg maintenance and cessation after dose escalation was evaluated using STEP 4 data among 803 participants tolerating 20 weeks of semaglutide run‐in.
Results
GI AEs were more common with semaglutide 2.4 mg than placebo, with most frequently nausea (43.9% vs. 16.1% of participants), diarrhoea (29.7% vs. 15.9%), vomiting (24.5% vs. 6.3%) and constipation (24.2% vs. 11.1%). Most GI AEs with semaglutide were non‐serious (99.5% of AEs), mild‐to‐moderate (98.1%), transient and occurred most frequently during/shortly after dose escalation. Few semaglutide‐treated participants (4.3%) permanently discontinued treatment for GI AEs. In STEP 1‐3, mean WL with semaglutide 2.4 mg was similar in participants without (9.6%‐17.1%) versus with GI AEs (11.4%‐17.7%). Consistent with this observation, mediation analysis found that GI AEs contributed little to semaglutide‐induced WL: of the additional 7.6%‐14.4% WL with semaglutide versus placebo, <1 percentage point was mediated by GI AEs. In STEP 4, semaglutide 2.4 mg maintenance was well tolerated.
Conclusions
GI AEs were more common with semaglutide 2.4 mg than placebo, but typically mild‐to‐moderate and transient. Semaglutide‐induced WL was largely independent of GI AEs.
Keywords: antiobesity drug, GLP‐1 analogue, obesity therapy, phase III study, randomized trial, weight control
1. INTRODUCTION
Obesity is a chronic, relapsing disease, leading to substantial burden on individuals and health care systems worldwide. 1 , 2 Weight management guidelines recommend pharmacotherapy as an adjunct to lifestyle interventions in patients with a body mass index (BMI) ≥30 kg/m2, or ≥27 kg/m2 with weight‐related comorbidities. 3 , 4 , 5 , 6
Semaglutide is a glucagon‐like peptide‐1 receptor agonist (GLP‐1RA) indicated for type 2 diabetes (T2D) and now approved by the US Food and Drug Administration for weight management in people with overweight or obesity at a once‐weekly subcutaneous dose of 2.4 mg. 7 In the phase III Semaglutide Treatment Effect in People with obesity (STEP) 1‐4 studies, weekly semaglutide 2.4 mg demonstrated substantial, clinically meaningful weight losses and improvements in cardiometabolic parameters and patient‐reported outcomes. 8 , 9 , 10 , 11
Gastrointestinal (GI) adverse events (AEs), most commonly mild‐to‐moderate nausea, are a dose‐dependent class effect of GLP‐1RAs. 12 , 13 , 14 We conducted a pooled analysis of the STEP 1‐3 trials to evaluate the GI AE profile of semaglutide 2.4 mg. In addition, we explored whether GI AEs contributed to the weight‐loss effects of semaglutide in STEP 1‐3. Data from the STEP 4 withdrawal trial were analysed separately and used to evaluate the incidence of GI AEs after achievement of the target 2.4 mg maintenance dose. These analyses may inform understanding of both weight loss and GI tolerability with semaglutide 2.4 mg.
2. MATERIALS AND METHODS
2.1. Trial designs and populations
The STEP 1‐4 trial designs have been published. 8 , 9 , 10 , 11 , 15 In brief, STEP 1, 3 and 4 enrolled adults aged ≥18 years with a BMI ≥27 kg/m2 (with ≥1 weight‐related comorbidity) or ≥30 kg/m2, without diabetes. Participants in STEP 2 had a BMI of ≥27 kg/m2 plus T2D.
In STEP 1, semaglutide 2.4 mg was compared with placebo on a background of lifestyle intervention. In STEP 2, semaglutide 2.4 mg was compared with placebo or semaglutide 1.0 mg, plus lifestyle intervention (as semaglutide 1.0 mg was not developed for weight management, data for this dose are included in File S1). STEP 3 compared semaglutide 2.4 mg with placebo, as adjunct to intensive behavioural therapy. Study designs were similar, consisting of a 68‐week, randomized, placebo‐controlled treatment period (Figure S1), enabling pooling of data. The 68‐week STEP 4 trial used a withdrawal design: after a 20‐week run‐in period with open‐label semaglutide, participants were randomized to continued semaglutide 2.4 mg versus switch to placebo (both as adjunct to lifestyle intervention) (Figure S1). Only those who tolerated the 2.4 mg dose at week 20 were eligible for randomization. All trials were conducted according to the International Conference on Harmonisation Good Clinical Practice guidelines and the Declaration of Helsinki.
2.2. Study protocol and titration schedule
Each STEP trial included an initial dose escalation for semaglutide, with initiation at 0.25 mg once weekly for 4 weeks, increased at 4‐weekly intervals to 0.5 mg, 1.0 mg, 1.7 mg and finally 2.4 mg at week 16. 8 , 9 , 10 , 11 , 15 Participants unable to tolerate 2.4 mg (i.e. would otherwise discontinue treatment) were permitted to remain at lower maintenance doses, with at least one attempt to re‐escalate to 2.4 mg. Participants discontinuing treatment prematurely remained in each trial.
AE information, including onset and end date, was collected throughout each trial, using open‐ended, non‐leading verbal questions. Reported AEs were proactively followed up at each subsequent visit/contact. AEs were coded using the current version of the Medical Dictionary for Regulatory Activities (Version 22.1) and categorized based on severity and seriousness, using standard definitions (File S1). AE incidence was assessed as a supportive secondary safety endpoint in each trial.
2.3. Statistical considerations
On‐treatment GI AE incidence was evaluated in post‐hoc analyses performed using pooled STEP 1‐3 data for semaglutide 2.4 mg and placebo arms. STEP 4 was not included in the pooled analysis because of the differences in study design. For AE analyses, participants were considered to be on treatment if any dose of trial product was administered within the previous 49 days. The percentage of participants that experienced GI AEs and the event rate per 100 patient‐years of exposure were adjusted using Cochran‐Mantel‐Haenszel weights to account for differences between trials. 16 Median durations of GI AEs were estimated using the Kaplan‐Meier estimator.
The effect of GI AEs on weight loss was explored using two different post‐hoc analyses:
A descriptive analysis of percentage change in body weight from baseline to week 68 among participants who did or did not experience GI AEs during STEP 1‐3, using observed body weight data from participants who were on treatment and had a body weight assessment at week 68 (on treatment was defined as any dose of trial product within the previous 2 weeks). Analyses were performed separately among participants with/without (i) any GI AEs and (ii) a subset of common GI AEs that were probably considered to influence weight loss (nausea, diarrhoea and vomiting).
Mediation analysis used a natural effects model with imputation‐based estimation, as described previously. 17 , 18 , 19 This analysis aimed to separate the overall effects on body weight into effects mediated by GI AEs (indirect effects) and those unrelated to GI AEs (direct effects), for the STEP 1‐3 trials. Changes in body weight were analysed addressing the effect of treatment (if taken as intended) using a mixed model for repeated measurements. 20
GI AE incidence in the STEP 4 trial was analysed with a methodology similar to that used for the STEP 1‐3 pooled analysis, with the exception that no adjustment of AE incidence or event rate was performed. Data from participants able to tolerate the semaglutide 2.4 mg dose during the 20‐week run‐in period who were subsequently randomized were used to evaluate the effect of continued semaglutide 2.4 mg or cessation of treatment (switch to placebo) on GI AE incidence.
3. RESULTS
3.1. Demographics and baseline characteristics (STEP 1‐4)
In total, 2117 participants were randomized to semaglutide 2.4 mg and 1262 to placebo within the STEP 1‐3 trials. In STEP 4, 902 participants entered the initial 20‐week semaglutide run‐in period; of these, 803 participants were subsequently randomized to continued semaglutide 2.4 mg (n = 535) or placebo (n = 268).
Baseline characteristics were similar in each trial, except that the STEP 2 population included fewer female participants, had lower BMI and higher age and glycated haemoglobin compared with STEP 1 and 3 (Table S1). In STEP 4, participant characteristics at randomization (week 20) were comparable between the continued semaglutide 2.4 mg and placebo arms (Table S1).
The majority of participants randomized to semaglutide 2.4 mg remained on treatment at week 68 in STEP 1‐3 (84.0%) and in STEP 4 (94.2%). Among these, most were receiving 2.4 mg once weekly (STEP 1‐3: 87.0%; STEP 4: 89.5%).
3.2. Incidence, timing and severity of any type of gastrointestinal adverse event (STEP 1‐3 pooled analysis)
A greater proportion of participants reported GI AEs in the semaglutide 2.4 mg arm compared with placebo: 72.9% and 47.1%, respectively (Table S2). Most GI AEs were non‐serious (99.5% of AEs) and mild or moderate in severity (98.1%) (Table S2). Severe GI AEs (namely nausea, abdominal pain, diarrhoea and vomiting) were reported by more participants in the semaglutide 2.4 mg arm (4.1% of participants) compared with the placebo arm (0.9%) (Table S2). GI AEs were reported more frequently within the dose‐escalation period, with the cumulative incidence of participants experiencing their first GI AE plateauing after week 20 (Figure 1A). Data for the 1.0 mg dose of semaglutide (STEP 2) are shown in Table S3 and Figure S2.
FIGURE 1.
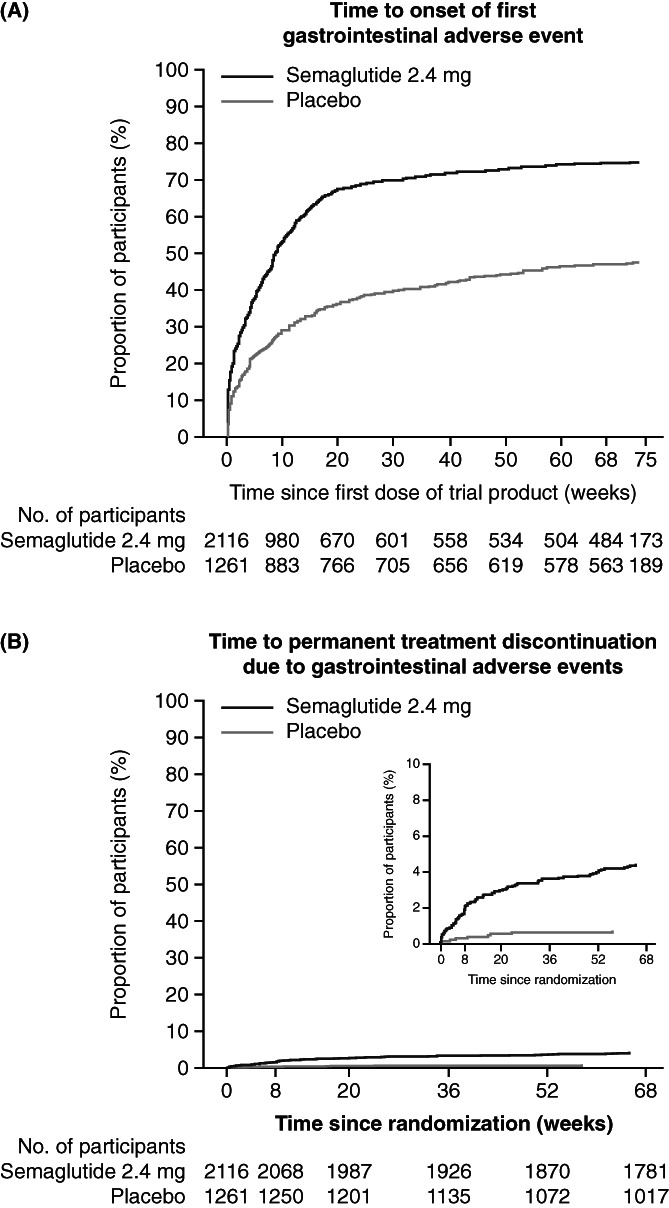
In the STEP 1‐3 trials: (A) Time to onset of first gastrointestinal adverse event; (B) Gastrointestinal adverse events leading to permanent treatment discontinuation. Data are on‐treatment adverse events (participants were considered to be on treatment if any dose of trial product was administered within the previous 49 days). Numbers below the plots represent the number of participants at risk. Equivalent data for the individual treatment arms (including semaglutide 1.0 mg) in the STEP 2 trial are shown in Figure S2
3.3. Incidence, timing and severity of most common gastrointestinal adverse events (STEP 1‐3 pooled analysis)
The most commonly reported GI AEs with semaglutide 2.4 mg were nausea, diarrhoea, vomiting and constipation (Table S2). Relative to the placebo arm, the prevalence of nausea, diarrhoea, vomiting and constipation in the semaglutide 2.4 mg arm were elevated throughout the 68‐week treatment period (Figure 2A‐D). The prevalence of nausea, diarrhoea and vomiting in the semaglutide 2.4 mg arm peaked at about week 20 and decreased thereafter, with the most prominent decline found for nausea (Figure 2A‐C). Individual nausea, diarrhoea and vomiting events were relatively short‐lived: in the semaglutide 2.4 mg arm, the median durations of nausea, diarrhoea and vomiting were 8, 3 and 2 days, respectively, and were similar to placebo (Figure 2A‐C). The median duration of constipation was longer: 47 days in the semaglutide arm and 35 days for placebo, with the prevalence plateauing at approximately week 10 (Figure 2D).
FIGURE 2.
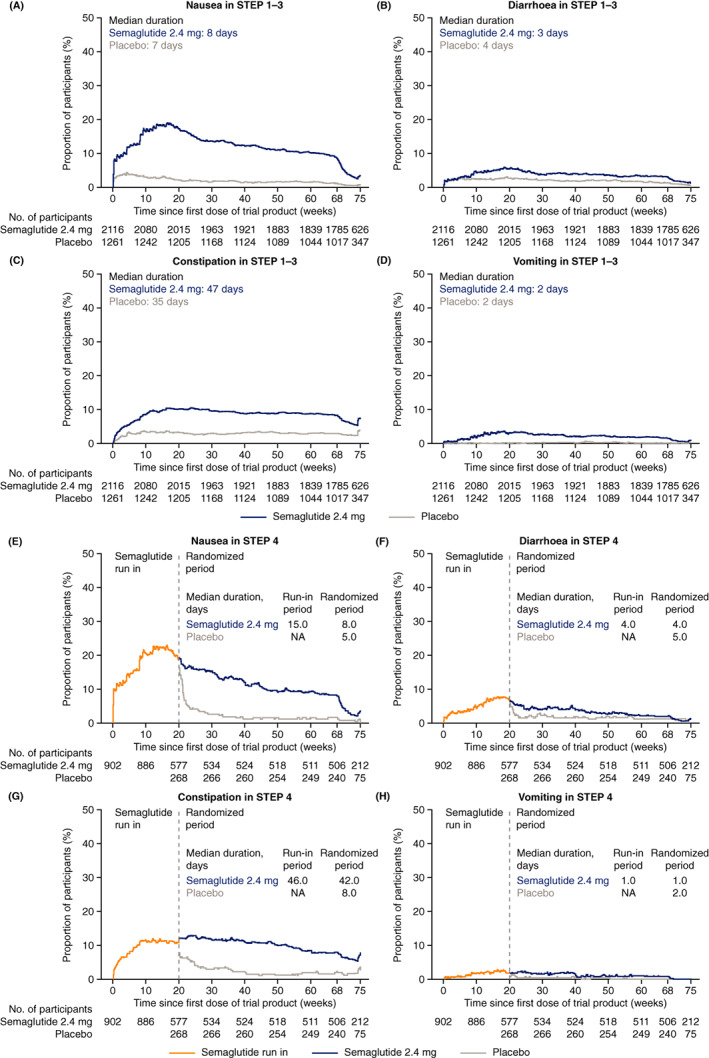
Prevalence of adverse events (nausea, diarrhoea, constipation and vomiting) over time in the (A‐D) STEP 1‐3 trials and (E‐H) STEP 4 trial. NA, not applicable. Data are on‐treatment adverse events (participants were considered to be on treatment if any dose of trial product was administered within the previous 49 days)
3.4. Impact of gastrointestinal adverse events on dose and treatment adherence (STEP 1‐3 pooled analysis)
GI AEs led to dose reduction or temporary treatment interruption in 12.5% of participants in the semaglutide 2.4 mg arm versus 1.7% of participants in the placebo arm. GI AEs led to permanent treatment discontinuation in more participants in the semaglutide 2.4 mg arm (4.3%) than in the placebo arm (0.7%), with most discontinuations occurring during the dose‐escalation period in both arms (Figure 1B).
Almost all participants who experienced GI AEs in the semaglutide 2.4 mg arm continued and completed the trial (95.5%), with a similar completion rate among those who did not experience GI AEs (93.0%). The proportion of participants in the semaglutide 2.4 mg arm who completed the trials on treatment was similar for participants who experienced GI AEs (83.1%) and for those who did not (86.7%); most of these participants (83.7% and 96.0%, respectively) were receiving the 2.4 mg dose at week 68 (Table 1). Among the participants in the semaglutide arm who experienced a dose reduction or temporary treatment interruption owing to GI AEs, 74.0% subsequently completed the study on treatment (at completion, 60.2% reported taking a dose of ≥1.7 mg and 36.7% the 2.4 mg dose) (Table 1).
TABLE 1.
Participant disposition in the STEP 1‐3 trials (pooled data) for: (i) the overall population; (ii) participants with or without GI AEs and (iii) participants with dose reductions or temporary treatment interruptions in response to a GI AE
| Semaglutide 2.4 mg once weekly | Placebo | |||||||
|---|---|---|---|---|---|---|---|---|
| n (%) | All participants (N = 2117) | Participants with GI AEs (N = 1562) | Participants without GI AEs (N = 555) | Participants who reduced dose or temporarily interrupted treatment in response to a GI AE (N = 265) | All participants (N = 1262) | Participants with GI AEs (N = 581) | Participants without GI AEs (N = 681) | Participants who reduced dose or temporarily interrupted treatment in response to a GI AE (N = 22) |
| In trial at week 68 | 2007 (94.8) | 1491 (95.5) | 516 (93.0) | 252 (95.1) | 1183 (93.7) | 546 (94.0) | 637 (93.5) | 21 (95.5) |
| On treatment at week 68 | 1779 (84.0) | 1298 (83.1) | 481 (86.7) | 196 (74.0) | 1021 (80.9) | 464 (79.9) | 557 (81.8) | 14 (63.6) |
| After ≥1 temporary interruption a | 199 (9.4) | 171 (10.9) | 28 (5.0) | 88 (33.2) | 109 (8.6) | 67 (11.5) | 42 (6.2) | 8 (36.4) |
| Permanent treatment discontinuation | 338 (16.0) | 264 (16.9) | 74 (13.3) | 69 (26.0) | 241 (19.1) | 117 (20.1) | 124 (18.2) | 8 (36.4) |
| Primary reason for permanent treatment discontinuation | ||||||||
| AE | 143 (6.8) | 133 (8.5) | 10 (1.8) | 38 (14.3) | 40 (3.2) | 27 (4.6) | 13 (1.9) | 3 (13.6) |
| Safety concern (investigator) | 17 (0.8) | 12 (0.8) | 5 (0.9) | 4 (1.5) | 2 (0.2) | 2 (0.3) | 0 | 2 (9.1) |
| Withdrawal of consent | 15 (0.7) | 8 (0.5) | 7 (1.3) | 2 (0.8) | 20 (1.6) | 9 (1.5) | 11 (1.6) | 0 |
| Lost to follow‐up | 49 (2.3) | 30 (1.9) | 19 (3.4) | 6 (2.3) | 35 (2.8) | 15 (2.6) | 20 (2.9) | 1 (4.5) |
| Other | 114 (5.4) | 81 (5.2) | 33 (5.9) | 19 (7.2) | 144 (11.4) | 64 (11.0) | 80 (11.7) | 2 (9.1) |
| Last dose for treatment completers, mg | ||||||||
| 2.4 | 1548/1779 (87.0) b | 1086/1298 (83.7) b | 462/481 (96.0) b | 72/196 (36.7) b | 994/1021 (97.4) b | 446/464 (96.1) b | 548/557 (98.4) b | 10/14 (71.4) b |
| 1.7 to <2.4 | 90/1779 (5.1) b | 84/1298 (6.5) b | 6/481 (1.2) b | 46/196 (23.5) b | 10/1021 (1.0) b | 9/464 (1.9) b | 1/557 (0.2) b | 3/14 (21.4) b |
| <1.7 | 129/1779 (7.3) b | 120/1298 (9.2) b | 9/481 (1.9) b | 77/196 (39.3) b | 11/1021 (1.1) b | 6/464 (1.3) b | 5/557(0.9) b | 1/14 (7.1) b |
| Other/not reported | 12/1779 (0.7) b | 8/1298 (0.6) b | 4/481 (0.8) b | 1/196 (0.5) b | 6/1021 (0.6) b | 3/464 (0.7) b | 3/557 (0.5) b | 0 |
Note: Proportion of participants (%) stated among the total number of participants in each group, unless indicated otherwise.
Abbreviations: AE, adverse event; GI, gastrointestinal.
Temporary treatment interruptions for any reason.
Proportion of participants (%) stated among those who were on treatment at week 68.
3.5. Impact of gastrointestinal adverse events on weight loss (STEP 1‐3)
Among participants on treatment at week 68 with a body weight assessment, the observed placebo‐corrected weight loss from baseline to week 68 for semaglutide 2.4 mg was 14.4 percentage points in the STEP 1 trial, 7.6 percentage points in the STEP 2 trial and 12.7 percentage points in the STEP 3 trial. Weight loss appeared nearly as great in those without versus with GI AEs (Figure 3). In the semaglutide 2.4 mg arms, the mean change observed from baseline to week 68 in body weight in those with versus without GI AEs was −17.3% versus −15.7% in STEP 1, −11.4% versus −9.6% in STEP 2 and −17.7% versus −17.1% in STEP 3. Results were similar when weight change was analysed in participants with or without any of the three common GI AEs that were considered to possibly influence weight loss (nausea, diarrhoea and/or vomiting) (Figure 3).
FIGURE 3.
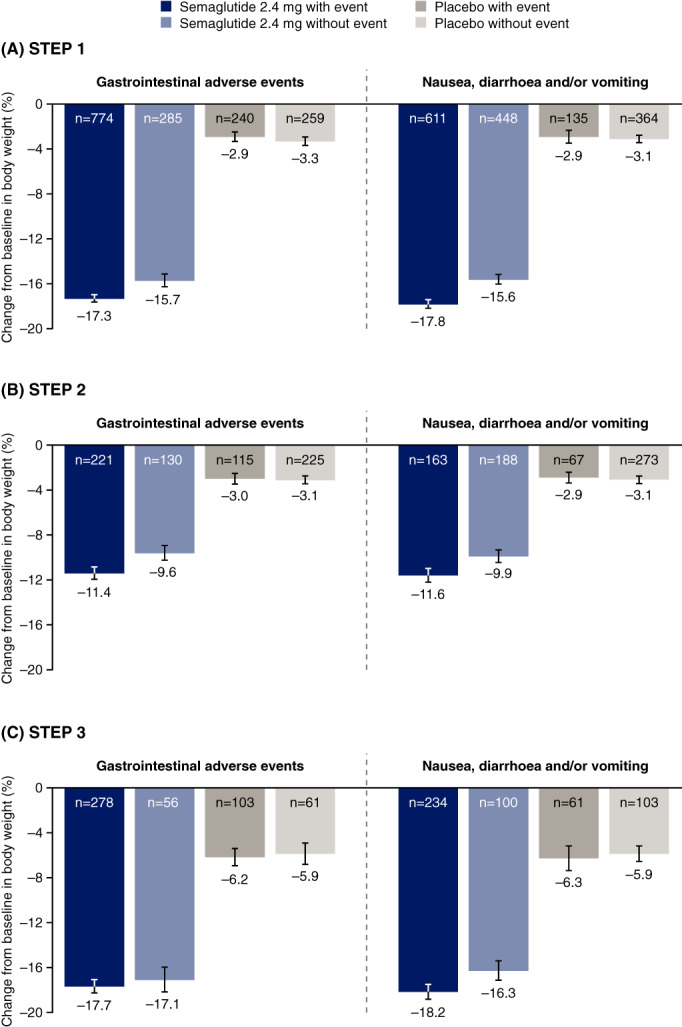
Change in body weight from baseline to week 68 among participants with and without gastrointestinal adverse events in: (A) STEP 1; (B) STEP 2; and (C) STEP 3. Bars present the mean percentage change from baseline in body weight ± standard error of the mean. Body weight data are observed on‐treatment data (any dose of trial product within previous 2 weeks) among participants who had a week 68 body weight assessment. Gastrointestinal adverse events comprise any type of gastrointestinal disorder, including on‐treatment adverse events (for assessment of adverse events, participants were considered to be on treatment if any dose of trial product was administered within the previous 49 days). Additional information on these analyses is included in Table S4
Mediation analysis found that the vast majority of the weight‐loss effects of semaglutide 2.4 mg were because of effects unrelated to GI AEs. Overall, <1 percentage point of semaglutide‐induced weight loss versus placebo was mediated by GI AEs, whether analysed based on the occurrence of any GI AE (Figure 4A) or the occurrence of nausea, diarrhoea and/or vomiting (Figure 4B). There was no notable difference in the magnitude of weight loss effect mediated by GI AEs between the STEP 1, 2 and 3 trials (Figure 4).
FIGURE 4.
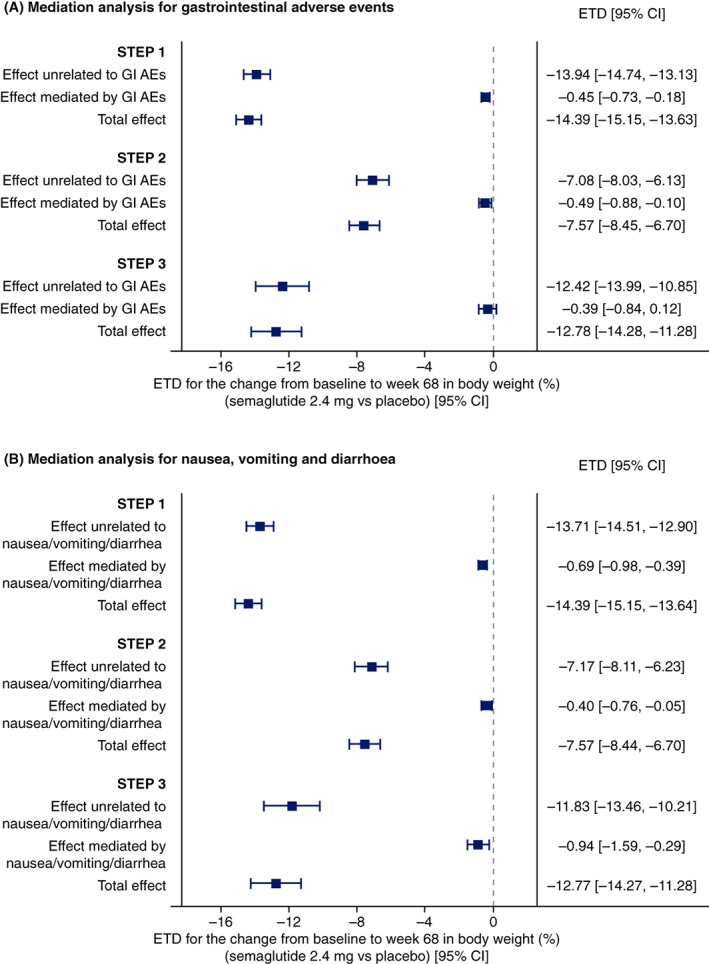
Mediation analysis of body weight changes mediated by or unrelated to GI AEs in the STEP 1‐3 trials. AE, adverse event; CI, confidence interval; ETD, estimated treatment difference; GI, gastrointestinal; HbA1c, glycated haemoglobin. Based on the on‐treatment data excluding measurements after initiation of antiobesity therapy (other obesity pharmacotherapy or bariatric surgery) from all randomized participants. Changes in body weight were analysed using a mixed model for repeated measurements, which included randomized treatment, stratification groups and their interaction (for STEP 2 only, including oral antihyperglycaemic drug treatment status and HbA1c category at screening) as factors, and baseline body weight as covariate, all nested within visit. Effects were estimated using a natural effects model (interaction between treatment and any GI AEs together with the baseline variables of body weight and stratification factors [STEP 2 only] as main effects, assuming no interaction between natural effects and baseline variables) with imputation‐based estimation. CIs are 95% Wald CIs. GI AEs comprise any type of GI disorder, including on‐treatment AEs (participants were considered to be on treatment if any dose of trial product was administered within the previous 49 days)
3.6. Effect of treatment maintenance on gastrointestinal adverse event incidence (STEP 4)
Of the 902 participants enrolled in the initial 20‐week run‐in period, 71.4% reported GI AEs, with type, severity and chronology similar to that reported in STEP 1‐3 (Table S2; Figure 2E‐H). In total, 99 participants (11.0%) enrolled in the run‐in did not attain the target dosage required to participate in the randomized period at week 20, with AEs cited as the most common reason (48 of 99 participants [48.4%]) .
Among the 803 participants randomized at week 20, GI AEs with onset during the randomized period were reported in 41.9% of participants receiving continued semaglutide 2.4 mg treatment, compared with 26.1% of participants that switched to placebo (Table S2). In participants receiving continued semaglutide 2.4 mg treatment, the prevalence of nausea, diarrhoea and constipation decreased over time, and the prevalence of vomiting remained low (Figure 2E‐H).
Almost all cases of permanent treatment discontinuation because of GI AEs occurred during the run‐in period (in 44 enrolled participants [4.9%]). After randomization, few participants in either arm experienced dose adjustments or temporary or permanent discontinuations of treatment because of GI AEs (Table S2).
4. DISCUSSION
These analyses provide a robust assessment of the GI tolerability of semaglutide 2.4 mg in ~2650 adults over 68 weeks and show that weight loss with semaglutide 2.4 mg was mostly attributable to effects unrelated to GI AEs.
Pooled data from the STEP 1‐3 trials demonstrate frequent reports of GI AEs in both semaglutide 2.4 mg and placebo arms, with nausea, diarrhoea, vomiting and constipation the most common side effects with semaglutide. The relatively high incidence of GI AEs in the placebo arms was not unexpected and may in part reflect the known underlying increased risk of GI disorders associated with obesity. 21 While not assessed directly in our study, crude comparison of the incidences of GI AEs reported in the individual STEP 1, 2 and 3 trials 8 , 9 , 10 indicates between‐trial variation in incidences for both semaglutide 2.4 mg and placebo arms, which may reflect trial‐specific differences in design and patient populations.
Although GI AEs occurred more frequently with semaglutide 2.4 mg than with placebo across STEP 1‐4, the vast majority of GI AEs reported were non‐serious and mild‐to‐moderate in severity, and did not necessitate dose reduction or discontinuation. GI AEs were most prevalent during or shortly after dose escalation, declining in prevalence thereafter. While rates of nausea, diarrhoea and vomiting with semaglutide remained elevated compared with placebo throughout treatment, participants typically recovered from each event within a few days. Constipation tended to last longer, and may be because of the effects of GLP‐1RAs on GI motility. 22 Among the participants who reported any GI AEs, the vast majority experienced their first event during the dose‐escalation period, suggesting that the elevated prevalence of GI AEs with semaglutide versus placebo after dose escalation is primarily because of additional events being reported by participants who have previously experienced a GI AE. Collectively, these results should reassure patients and physicians alike that GI AEs associated with semaglutide 2.4 mg are unlikely to be serious and will typically be transient, although a small proportion of patients may continue to experience GI AEs throughout treatment. Importantly, in STEP 1‐3, only 4.3% of participants in the semaglutide arm discontinued treatment prematurely because of GI AEs, with very few discontinuations occurring after dose escalation.
STEP 4 provides additional insight and reassurance on the GI tolerability profile of semaglutide 2.4 mg. Participants able to tolerate semaglutide 2.4 mg utilizing the standard escalation regimen during the 20‐week run‐in were typically able to tolerate continued treatment for the remainder of the trial, with only two discontinuations because of GI AEs after week 20. Furthermore, for those who had ongoing GI side effects, the prevalence of nausea, diarrhoea and constipation decreased gradually over time.
GI disorders are well‐known side effects of GLP‐1RAs, leading clinicians to query whether weight losses are a result of these side effects. Across STEP 1‐3, we observed that reductions in body weight from baseline to week 68 with semaglutide 2.4 mg were nearly as great in participants without versus with GI AEs: in the descriptive analysis, weight loss with semaglutide 2.4 mg ranged from 9.6% to 17.1% in participants without GI AEs and from 11.4% to 17.7% in those with GI AEs. Consistent with these observations, the mediation analysis (which formally estimates the contribution of GI AEs to weight loss) found that GI AEs appeared to contribute little to the weight‐loss benefit of semaglutide: of the additional 7.6%‐14.4% weight loss provided by semaglutide 2.4 mg over placebo in STEP 1‐3, <1 percentage point was estimated to be mediated by GI AEs (for GI disorders overall and specifically for the occurrence of nausea, diarrhoea and/or vomiting). Thus, the mediation analysis found that weight loss with semaglutide 2.4 mg was mostly attributable to treatment effects unrelated to GI AEs. These results are consistent with previous analyses of the weight‐loss effects of GLP‐1RAs in people with obesity and/or T2D, which typically showed a small contribution of GI AEs to GLP‐1RA‐induced weight loss. 13 , 17 , 18 , 23 , 24 The ability of semaglutide to lower body weight appears to relate to increased satiety, appetite regulation, improved hedonic and homeostatic control of eating and reduced energy intake, mediated by direct and indirect central nervous system effects, particularly on the hypothalamus and hindbrain. 25 , 26 , 27
The GI AE profile of semaglutide 2.4 mg in the STEP trials is consistent with previous observations with lower semaglutide doses and the established AE profile of GLP‐1RAs. 14 , 28 , 29 Direct comparison of GI AE incidence with semaglutide 1.0 and 2.4 mg in adults with T2D and overweight or obesity in STEP 2 found only a slightly higher incidence of GI AEs with semaglutide 2.4 mg (63.5% of participants) versus 1.0 mg (57.5%), despite the more than doubling of dose, and few patients discontinued treatment because of GI AEs in either group (4.2% of participants vs. 3.5%, respectively). 9 These findings are consistent with the established dose dependence of GI AEs with the GLP‐1RA class and semaglutide specifically. 12 , 14 , 30 , 31 , 32 As higher incidences of GI AEs tend to be experienced with higher doses of GLP‐1RAs, gradual dose escalation and dose adjustment may help mitigate the impact of GI AEs in clinical practice. 29 , 30
Almost all approved obesity pharmacotherapies are commonly associated with GI AEs, including orlistat (e.g. faecal urgency), phentermine‐topiramate (e.g. constipation) and naltrexone‐bupropion (e.g. nausea and constipation). 1 , 3 Use of liraglutide 3.0 mg, another GLP‐1RA, approved for treatment of overweight or obesity, can also result in mild‐or‐moderate GI AEs of a nature similar to those reported in the STEP trials, primarily during initial dose escalation. 33 , 34 , 35 , 36 , 37
The mechanism of action through which GI AEs arise with GLP‐1RAs remains uncertain. Delayed gastric emptying may be a potential contributor, particularly with short‐acting GLP‐1RAs; longer‐acting agents do not appear to be associated with notable delays in gastric emptying. 14 , 26 , 30 A 12‐week study of semaglutide 1.0 mg in adults with obesity using the paracetamol absorption test identified a delay in first‐hour gastric emptying after a meal versus placebo; however, a 20‐week study of semaglutide 2.4 mg did not identify such a delay in paracetamol‐assessed gastric emptying. 26 , 38 Changes in the rate of lower GI transit may be responsible for constipation and/or diarrhoea, although evidence is lacking. The mechanism for GLP‐1RA‐induced nausea may primarily relate to central effects; studies in animal models suggest that nausea responses associated with peripheral GLP‐1RA administration involve activation of GLP‐1 receptors in the central nervous system. 39 , 40
In clinical practice, GI AEs (most commonly nausea) are known to be a common reason for discontinuation of GLP‐1RA treatment. 41 People with overweight or obesity must balance the typically short‐term impact of potential GI AEs against the significant health benefits offered by long‐term GLP‐1RA treatment. While physicians must establish a differential diagnosis to exclude other potential causes of GI symptoms (particularly if symptoms are prolonged/severe), adopting strategies to mitigate the impact of GI AEs and aid resolution is important to optimize persistence with GLP‐1RA treatment. A range of complementary approaches has been proposed, including: patient education and counselling on topics such as meal size and stopping eating when feeling full 29 , 42 ; gradual dose escalation 7 , 43 , 44 , 45 , 46 ; and dose adjustment with re‐escalation upon AE resolution. 15
This study has some limitations. First, the pooled analysis and mediation analyses were post hoc and should, therefore, be considered as exploratory analyses. Second, the time course of GI AEs was not fully accounted for in the analyses of contribution to weight loss. In addition, the descriptive analyses of the impact of GI AEs on body weight changes were only conducted in those who remained on treatment at week 68, and thus those who discontinued treatment before this time were excluded. Furthermore, the mediation analysis should be interpreted with caution, as it assumes no confounding factors beyond those included in the model (baseline body weight and stratification factors), which may not be the case, given that post‐randomization events (GI AEs) are used in the analysis. For the STEP 4 analyses, while the randomization to continued semaglutide or placebo was double‐blinded, participants were aware of this randomized withdrawal trial design, which could influence AE reporting. Finally, it should be noted that the STEP trials represent a controlled clinical trial environment with regular follow‐up, which may differ from routine clinical practice.
In conclusion, while GI AEs were common with semaglutide 2.4 mg across the STEP 1‐4 trials, effects were typically mild‐to‐moderate, non‐serious and transient, with few events leading to treatment discontinuation. The substantial weight‐lowering effects of semaglutide 2.4 mg appeared to be largely independent of GI AEs, both for any type of GI AE and for nausea, diarrhoea and/or vomiting specifically.
CONFLICT OF INTEREST
SW reports research funding, advisory/consulting fees and/or other support from AstraZeneca, Bausch Health Inc., Boehringer Ingelheim, CIHR, Janssen, Lilly and Novo Nordisk. SC is an employee of and shareholder at Novo Nordisk A/S. MD is a consultant, advisory board member and speaker for AstraZeneca, Boehringer Ingelheim, Janssen, Lilly, Merck Sharp & Dohme, Novo Nordisk and Sanofi‐Aventis; advisory board member for Gilead Sciences Ltd. and Servier; speaker for Mitsubishi Tanabe Pharma Corporation, NAPP and Takeda Pharmaceuticals International Inc.; received research funding from AstraZeneca, Boehringer Ingelheim, Janssen, Lilly, Novo Nordisk and Sanofi‐Aventis. MD is also co‐funded by the NIHR Leicester Biomedical Research Centre. DD is a consultant, advisory board member and speaker for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk and Sanofi‐Aventis; received research funding from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk and Sanofi‐Aventis. BG is an employee of and shareholder at Novo Nordisk A/S. IL reports research funding, advisory/consulting fees and/or other support from AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, GI Dynamics, Intarcia, Intercept, Janssen, Mannkind, Merck, Mylan, Novartis, Novo Nordisk, Pfizer, Sanofi, TARGETPharma, Valeritas and Zealand Pharma. OM is an advisory board member for AstraZeneca, Boehringer Ingelheim, BOL Pharma, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk and Sanofi; received research grant support through Hadassah Hebrew University Hospital from AstraZeneca and Novo Nordisk; speaker's bureau for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck Sharp & Dohme, Novo Nordisk and Sanofi. DMR is a consultant, advisory board member, speaker and clinical investigator for Novo Nordisk; clinical investigator for AstraZeneca and Boehringer Ingelheim; received honoraria from Medscape; received research funding from Obesinov and SARL; holds stock/shares in Novo Nordisk. MT is an employee of and shareholder at Novo Nordisk A/S. TAW serves on advisory boards for Novo Nordisk and WW (formerly Weight Watchers) and has received grant support, on behalf of the University of Pennsylvania, from Novo Nordisk. SDP has received consulting fees and/or speaking honoraria from Abbott, AstraZeneca, Bausch, Bayer, Boehringer Ingelheim, Dexcom, Eli Lilly, HLS, Janssen, Merck, Novo Nordisk and Sanofi; was involved in research studies for Abbott, AstraZeneca, Bausch, Boehringer Ingelheim, Eli Lilly, Janssen, Merck, Novo Nordisk and Sanofi.
AUTHOR CONTRIBUTIONS
All authors were responsible for the acquisition, analysis or interpretation of data and critical revision of the manuscript for important intellectual content. SW, DD and SDP drafted the manuscript. SW, SC, BG, IL, MT and SDP supervised the study. SC, DD, BG, IL and MT were involved in the concept and design. BG and MT performed the statistical analysis. SC, BG and MT were responsible for administrative, technical or material support.
PEER REVIEW
The peer review history for this article is available at https://publons.com/publon/10.1111/dom.14551.
Supporting information
File S1. Supporting Information.
ACKNOWLEDGMENTS
The authors thank the participants, investigators and site staff involved in the STEP 1‐4 trials. In addition, the authors thank Meir Schechter, MD, PhD (Diabetes Unit, Department of Endocrinology and Metabolism, Hadassah Medical Center; Faculty of Medicine, Hebrew University of Jerusalem, Israel), Maria Oxenbøll, MSc (an employee of Novo Nordisk A/S) and Hanna Kristina Hedman, PhD (previously an employee of Novo Nordisk A/S) for review of and input to the manuscript, and Nicola Beadle of Axis, a division of Spirit Medical Communications Group Ltd., and Melanie Jones, a contract writer working on behalf of Axis, for medical writing and editorial assistance (funded by Novo Nordisk A/S, Denmark). The STEP 1‐4 trials were funded by Novo Nordisk A/S.
Wharton S, Calanna S, Davies M, et al. Gastrointestinal tolerability of once‐weekly semaglutide 2.4 mg in adults with overweight or obesity, and the relationship between gastrointestinal adverse events and weight loss. Diabetes Obes Metab. 2022;24(1):94-105. doi:10.1111/dom.14551
All trials were registered with ClinicalTrials.gov (NCT03548935, NCT03552757, NCT03611582 and NCT03548987).
DATA AVAILABILITY STATEMENT
Data will be shared with bona fide researchers submitting a research proposal approved by the independent review board. Access request proposals can be found at novonordisk‐trials.com. Data will be made available after research completion, and approval of the product and product use in the European Union and the USA. Individual participant data will be shared in data sets in a de‐identified/anonymized format.
REFERENCES
- 1. Bessesen DH, Van Gaal LF. Progress and challenges in anti‐obesity pharmacotherapy. Lancet Diabetes Endocrinol. 2018;6(3):237‐248. 10.1016/S2213-8587(17)30236-X [DOI] [PubMed] [Google Scholar]
- 2. Frühbeck G, Busetto L, Dicker D, et al. The ABCD of obesity: an EASO position statement on a diagnostic term with clinical and scientific implications. Obes Facts. 2019;12(2):131‐136. 10.1159/000497124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. American Diabetes Association. 8 . Obesity management for the treatment of type 2 diabetes: Standards of Medical Care in Diabetes‐2020. Diabetes Care. 2020;43(suppl 1):S89‐S97 [Addendum in: Diabetes Care. 2020;43(8):1980]. 10.2337/dc20-S008 [DOI] [PubMed] [Google Scholar]
- 4. Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22(suppl 3):1‐203. 10.4158/EP161365.GL [DOI] [PubMed] [Google Scholar]
- 5. Wharton S, Lau DCW, Vallis M, et al. Obesity in adults: a clinical practice guideline. CMAJ. 2020;192(31):E875‐E891. 10.1503/cmaj.191707 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Yumuk V, Tsigos C, Fried M, et al. European guidelines for obesity management in adults. Obes Facts. 2015;8(6):402‐424 [Erratum in: Obes Facts. 2016;9(1):64]. 10.1159/000442721 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. U.S. Food & Drug Administration WEGOVY® (semaglutide) prescribing information. June 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/215256s000lbl.pdf. Accessed June 10, 2021.
- 8. Wilding JPH, Batterham RL, Calanna S, et al. Once‐weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384:989‐1002. 10.1056/NEJMoa2032183 [DOI] [PubMed] [Google Scholar]
- 9. Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double‐blind, double‐dummy, placebo‐controlled, phase 3 trial. Lancet. 2021;397(10278):971‐984. 10.1016/S0140-6736(21)00213-0 [DOI] [PubMed] [Google Scholar]
- 10. Wadden TA, Bailey TS, Billings LK, et al. Effect of subcutaneous semaglutide vs placebo as an adjunct to intensive behavioral therapy on body weight in adults with overweight or obesity: the STEP 3 randomized clinical trial. JAMA. 2021;325(14):1403‐1413. 10.1001/jama.2021.1831 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Rubino D, Abrahamsson N, Davies M, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325(14):1414‐1425. 10.1001/jama.2021.3224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Bettge K, Kahle M, Abd El Aziz MS, Meier JJ, Nauck MA. Occurrence of nausea, vomiting and diarrhoea reported as adverse events in clinical trials studying glucagon‐like peptide‐1 receptor agonists: a systematic analysis of published clinical trials. Diabetes Obes Metab. 2017;19(3):336‐347. 10.1111/dom.12824 [DOI] [PubMed] [Google Scholar]
- 13. Horowitz M, Aroda VR, Han J, Hardy E, Rayner CK. Upper and/or lower gastrointestinal adverse events with glucagon‐like peptide‐1 receptor agonists: incidence and consequences. Diabetes Obes Metab. 2017;19(5):672‐681. 10.1111/dom.12872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Nauck MA, Meier JJ. Management of endocrine disease: are all GLP‐1 agonists equal in the treatment of type 2 diabetes? Eur J Endocrinol. 2019;181(6):R211‐R234. 10.1530/EJE-19-0566 [DOI] [PubMed] [Google Scholar]
- 15. Kushner RF, Calanna S, Davies M, et al. Semaglutide 2.4 mg for the treatment of obesity: key elements of the STEP trials 1 to 5. Obesity (Silver Spring). 2020;28(6):1050‐1061. 10.1002/oby.22794 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Chuang‐Stein C, Beltangady M. Reporting cumulative proportion of subjects with an adverse event based on data from multiple studies. Pharm Stat. 2011;10(1):3‐7. 10.1002/pst.397 [DOI] [PubMed] [Google Scholar]
- 17. Ahrén B, Atkin SL, Charpentier G, et al. Semaglutide induces weight loss in subjects with type 2 diabetes regardless of baseline BMI or gastrointestinal adverse events in the SUSTAIN 1 to 5 trials. Diabetes Obes Metab. 2018;20(9):2210‐2219. 10.1111/dom.13353 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Lingvay I, Hansen T, Macura S, et al. Superior weight loss with once‐weekly semaglutide versus other glucagon‐like peptide‐1 receptor agonists is independent of gastrointestinal adverse events. BMJ Open Diabetes Res Care. 2020;8(2):e001706. 10.1136/bmjdrc-2020-001706 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Vansteelandt S, Bekaert M, Lange T. Imputation strategies for the estimation of natural direct and indirect effects. Epidemiol Methods. 2012;1(1):131‐158. 10.1515/2161-962X.1014 [DOI] [PubMed] [Google Scholar]
- 20. Wharton S, Astrup A, Endahl L, et al. Estimating and reporting treatment effects in clinical trials for weight management: using estimands to interpret effects of intercurrent events and missing data. Int J Obes (Lond). 2021;45(5):923‐933. 10.1038/s41366-020-00733-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Camilleri M, Malhi H, Acosta A. Gastrointestinal complications of obesity. Gastroenterology. 2017;152(7):1656‐1670. 10.1053/j.gastro.2016.12.052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Marathe CS, Rayner CK, Jones KL, Horowitz M. Effects of GLP‐1 and incretin‐based therapies on gastrointestinal motor function. Exp Diabetes Res. 2011;2011:279530. 10.1155/2011/279530 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Lean ME, Carraro R, Finer N, et al. Tolerability of nausea and vomiting and associations with weight loss in a randomized trial of liraglutide in obese, non‐diabetic adults. Int J Obes (Lond). 2014;38(5):689‐697. 10.1038/ijo.2013.149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Trautmann ME, Han J, Ruggles J. Early pharmacodynamic effects of exenatide once weekly in type 2 diabetes are independent of weight loss: a pooled analysis of patient‐level data. Clin Ther. 2016;38(6):1464‐1473. 10.1016/j.clinthera.2016.03.039 [DOI] [PubMed] [Google Scholar]
- 25. Blundell J, Finlayson G, Axelsen M, et al. Effects of once‐weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity. Diabetes Obes Metab. 2017;19(9):1242‐1251. 10.1111/dom.12932 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Friedrichsen M, Breitschaft A, Tadayon S, Wizert A, Skovgaard D. The effect of semaglutide 2.4 mg once weekly on energy intake, appetite and gastric emptying in subjects with obesity. Diabetes Obes Metab. 2021;23(3):754‐762. 10.1111/dom.14280 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Gabery S, Salinas CG, Paulsen SJ, et al. Semaglutide lowers body weight in rodents via distributed neural pathways. JCI Insight. 2020;5(6):e133429. 10.1172/jci.insight.133429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Aroda VR, Ahmann A, Cariou B, et al. Comparative efficacy, safety, and cardiovascular outcomes with once‐weekly subcutaneous semaglutide in the treatment of type 2 diabetes: insights from the SUSTAIN 1‐7 trials. Diabetes Metab. 2019;45(5):409‐418. 10.1016/j.diabet.2018.12.001 [DOI] [PubMed] [Google Scholar]
- 29. Hinnen D. Glucagon‐like peptide 1 receptor agonists for type 2 diabetes. Diabetes Spectr. 2017;30(3):202‐210. 10.2337/ds16-0026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Knudsen LB, Lau J. The discovery and development of liraglutide and semaglutide. Front Endocrinol (Lausanne). 2019;10:155. 10.3389/fendo.2019.00155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. O'Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double‐blind, placebo and active controlled, dose‐ranging, phase 2 trial. Lancet. 2018;392(10148):637‐649. 10.1016/S0140-6736(18)31773-2 [DOI] [PubMed] [Google Scholar]
- 32. Wilding JP, Overgaard RV, Jacobsen LV, Jensen CB, le Roux CW. Exposure‐response analyses of liraglutide 3.0 mg for weight management. Diabetes Obes Metab. 2016;18(5):491‐499. 10.1111/dom.12639 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Davies MJ, Bergenstal R, Bode B, et al. Efficacy of liraglutide for weight loss among patients with type 2 diabetes: the SCALE diabetes randomized clinical trial. JAMA. 2015;314(7):687‐699. 10.1001/jama.2015.9676 [DOI] [PubMed] [Google Scholar]
- 34. Garvey WT, Birkenfeld AL, Dicker D, et al. Efficacy and safety of liraglutide 3.0 mg in individuals with overweight or obesity and type 2 diabetes treated with basal insulin: the SCALE insulin randomized controlled trial. Diabetes Care. 2020;43(5):1085‐1093. 10.2337/dc19-1745 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Mehta A, Marso SP, Neeland IJ. Liraglutide for weight management: a critical review of the evidence. Obes Sci Pract. 2017;3(1):3‐14. 10.1002/osp4.84 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Pi‐Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11‐22. 10.1056/NEJMoa1411892 [DOI] [PubMed] [Google Scholar]
- 37. Wadden TA, Tronieri JS, Sugimoto D, et al. Liraglutide 3.0 mg and intensive behavioral therapy (IBT) for obesity in primary care: the SCALE IBT randomized controlled trial. Obesity (Silver Spring). 2020;28(3):529‐536. 10.1002/oby.22726 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Hjerpsted JB, Flint A, Brooks A, Axelsen MB, Kvist T, Blundell J. Semaglutide improves postprandial glucose and lipid metabolism, and delays first‐hour gastric emptying in subjects with obesity. Diabetes Obes Metab. 2018;20(3):610‐619. 10.1111/dom.13120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Kanoski SE, Rupprecht LE, Fortin SM, De Jonghe BC, Hayes MR. The role of nausea in food intake and body weight suppression by peripheral GLP‐1 receptor agonists, exendin‐4 and liraglutide. Neuropharmacology. 2012;62(5–6):1916‐1927. 10.1016/j.neuropharm.2011.12.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Kanoski SE, Hayes MR, Skibicka KP. GLP‐1 and weight loss: unraveling the diverse neural circuitry. Am J Physiol Regul Integr Comp Physiol. 2016;310(10):R885‐R895. 10.1152/ajpregu.00520.2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Sikirica MV, Martin AA, Wood R, Leith A, Piercy J, Higgins V. Reasons for discontinuation of GLP1 receptor agonists: data from a real‐world cross‐sectional survey of physicians and their patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2017;10:403‐412. 10.2147/DMSO.S141235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Fitch A, Ingersoll AB. Patient initiation and maintenance of GLP‐1 RAs for treatment of obesity: narrative review and practical considerations for primary care providers. Postgrad Med. 2021;133(3):310‐319. 10.1080/00325481.2020.1845534 [DOI] [PubMed] [Google Scholar]
- 43. Fineman MS, Shen LZ, Taylor K, Kim DD, Baron AD. Effectiveness of progressive dose‐escalation of exenatide (exendin‐4) in reducing dose‐limiting side effects in subjects with type 2 diabetes. Diabetes Metab Res Rev. 2004;20(5):411‐417. 10.1002/dmrr.499 [DOI] [PubMed] [Google Scholar]
- 44. Frias JP, Nauck MA, Van J, et al. Efficacy and tolerability of tirzepatide, a dual glucose‐dependent insulinotropic peptide and glucagon‐like peptide‐1 receptor agonist in patients with type 2 diabetes: a 12‐week, randomized, double‐blind, placebo‐controlled study to evaluate different dose‐escalation regimens. Diabetes Obes Metab. 2020;22(6):938‐946. 10.1111/dom.13979 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Papathanasiou T, Strathe A, Agersø H, Lund TM, Overgaard RV. Impact of dose‐escalation schemes and drug discontinuation on weight loss outcomes with liraglutide 3.0 mg: a model‐based approach. Diabetes Obes Metab. 2020;22(6):969‐977. 10.1111/dom.13985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. U.S. Food & Drug Administration SAXENDA® (liraglutide) prescribing information. March 2020. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/206321s011lbl.pdf. Accessed June 10, 2021
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
File S1. Supporting Information.
Data Availability Statement
Data will be shared with bona fide researchers submitting a research proposal approved by the independent review board. Access request proposals can be found at novonordisk‐trials.com. Data will be made available after research completion, and approval of the product and product use in the European Union and the USA. Individual participant data will be shared in data sets in a de‐identified/anonymized format.