
Figure 3.
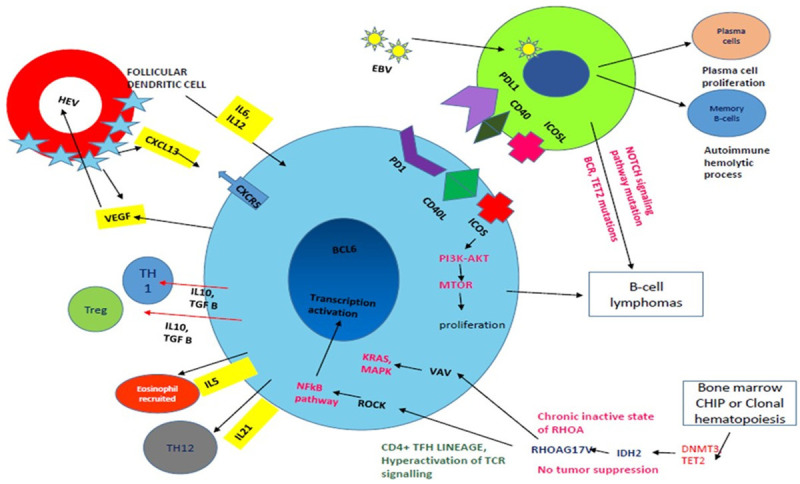
Pathogenesis of AITL: Art work shows TFH cells (Blue colour) interact with B-cells (Green colour) via PD1-PDL1, CD40L-CD40 and ICOSL-ICOS which leads to B-cell survival and proliferation. ICOS axis leads to TFH cell proliferation via p13AKT and mTOR pathway. Follicular dendritic cells secrete CXCL13, IL6, and IL2 creating conducive environment for proliferation of T-cells and in turn TFH cells produce VEGF which causes high endothelial venule proliferation (red colour circle). Eosinophils are recruited by IL5 secreted by TFH cells. EBV (small yellow circle with green spikes) infects the B-cells and further leads to T-cell proliferation and B-cell lymphomas rarely with gain of B-cell receptor, Tet2 mutations. Immunodeficiency is also caused by the virus. Increase in plasma cells and autoimmune haemolytic phenomenon can be associated with the B-cell proliferation associated. RHOA acts via the VAV-KRAS-MAPK and ROCK-NFkB pathway and affects the TFH cell differentiation and survival. Clonal haematopoiesis with various mutations can cause unregulated proliferation of the tumor cells.