

Abstract
Background
The Breast Health Initiative (BHI) was launched to demonstrate a scalable model to improve access to early diagnosis and treatment of breast cancer.
Methods
A package of evidence‐based interventions was codesigned and implemented with the stakeholders, as part of the national noncommunicable disease program, through the existing primary health care system. Data from the first 18 months of the BHI are presented.
Results
A total of 108,112 women received breast health education; 48% visited the health facilities for clinical breast examination (CBE), 3% had a positive CBE result, and 41% were referred to a diagnostic facility. The concordance of CBE findings between health care providers and adherence to follow‐up care improved considerably, with more women visiting the diagnostic facilities and completing diagnostic evaluation within 1 month from initial screening, and with only 9% lost to follow‐up. The authors observed a clinically meaningful decrease in time to complete diagnostic evaluation with biopsy, from 37 to 9 days.
Conclusions
The results demonstrate the feasibility and effectiveness of implementing a large‐scale, decentralized breast cancer early detection program delivered through the existing primary health care system in India.
Keywords: breast cancer, diagnosis, early detection, implementation, India
Short abstract
This article presents the key strategies, interventions, and results from the first 18 months of the large‐scale, decentralized breast cancer early detection program in a real‐world setting in India.
Introduction
Breast cancer is the most common cancer among women in India, 1 , 2 with an estimated 178,361 new cases and 90,408 deaths in 2020. 2 The 5‐year survival rate is less than 60% 3 and is likely due to a combination of factors: limited breast cancer awareness in the community and among health care providers, 4 suboptimal access to services for early detection of breast cancer resulting in late‐stage diagnosis, 5 and inequitable access to quality treatment. 6 Furthermore, the anticipated increase in breast cancer incidence is expected to challenge India's health care system with an increase of 52.3% by 2040. 1
To address the growing burden of noncommunicable diseases, the Ministry of Health and Family Welfare of the Government of India launched the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases, and Stroke (NPCDCS) in 2010. 7 The NPCDCS includes guidance for population‐based screening of all women aged 30 to 65 years for breast and cervical cancer. 7 However, operationalization and implementation of the program have been slow and inconsistent.
Since 2018, Jhpiego, an international nonprofit health organization affiliated with John's Hopkins University, has supported the Departments of Health in the states of Uttar Pradesh (UP) and Jharkhand in developing a resource‐appropriate, phased implementation strategy for decentralized breast cancer early detection and care, called the Breast Health Initiative (BHI). This strategy was codesigned with local experts and stakeholders within the context of the NPCDCS program and was based on guidelines developed by the Breast Health Global Initiative (BHGI). The BHGI is a resource‐stratified guideline for early detection, diagnosis, and treatment of breast cancer in low‐to‐middle‐income countries. 8 , 9
In this article, we present the key strategies, interventions, and results from the first 18 months of the BHI program. To our knowledge, this is one of the largest efforts to implement and evaluate a breast cancer early detection program in a public health setting in low‐to‐middle‐income countries.
Materials and Methods
We have conducted a situational assessment 5 of breast health services in both states using the BHGI “BCI2.5 toolkit.” 10 Based on the needs identified in the situational assessment 5 and relevant stakeholder inputs, combined with the guidance included in NPCDCS, 7 a context‐appropriate implementation plan for breast cancer care delivery was created.
The BHI implementation plan included training for and deployment of female community health workers (who are called accredited social health activists [ASHAs]) to conduct tailored breast cancer awareness programs aimed at women aged 30 to 65 years and quality clinical breast examination (CBE) training for auxiliary nurse midwives (ANMs), staff nurses, and medical officers at the primary care clinics.
According to the framework (Fig. 1), frontline health workers increase breast health awareness and encourage and facilitate women who have breast symptoms to present to the nearest primary‐level health facility for CBE by trained health care staff (auxiliary nurse midwives, facility‐based staff nurses, and/or physicians). Women with an abnormal CBE are referred to district hospitals for confirmatory CBE, imaging (breast ultrasound and/or mammography), fine‐needle aspiration biopsy (FNAB), and/or biopsy followed by pathologic confirmation. Women with a confirmed case of breast cancer are referred to the nearest medical college or tertiary care center for further evaluation and treatment.
Figure 1.
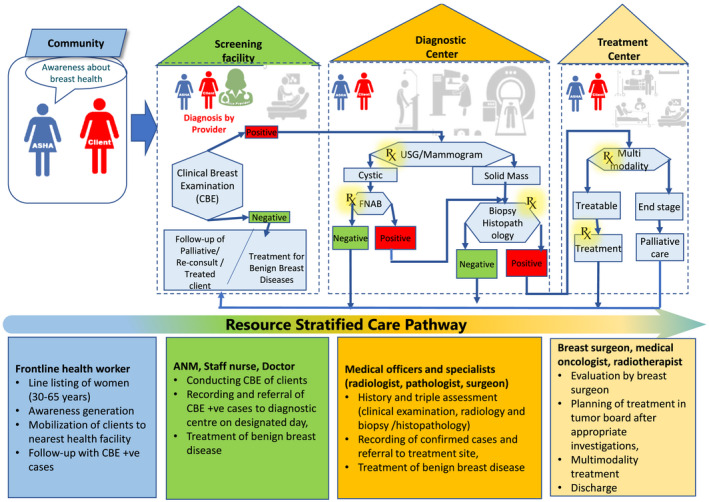
Operational framework and resource‐stratified care pathways for breast health services. ANM indicates auxiliary nurse midwife; ASHA, accredited social health activist; FNAB, fine‐needle aspiration biopsy; USG, ultrasonography.
We established a robust monitoring and evaluation system at the onset of the program, so that all key data needed for decision‐making could be captured in a timely and reliable manner. A centralized digital dashboard (Supporting Fig. 1) allowed for real‐time monitoring of key indicators.
In this article, we analyzed data collected from October 2018 to March 2020, including program outreach, quality of CBE defined as concordance of CBE findings between health care providers at the primary versus secondary levels of the health care system, adherence to follow‐up care for women with an abnormal CBE, time to complete diagnostic evaluation, and confirmed breast cancer diagnoses.
Program Sites
The BHI was implemented in UP and Jharkhand (Fig. 2). The program sites were purposefully selected to represent urban and rural settings, which can help future scale‐up efforts and sustainability in various settings. Both UP and Jharkhand are high‐focus states because of persistently low health outcomes. 11 , 12 The estimated age‐standardized incidence rate of breast cancer in UP and Jharkhand is 21.1 and 17.4 per 100,000 women, respectively. 13
Figure 2.

The intervention states.
Ethical Considerations
The data analysis was performed with the approval of the institutional review board of the Johns Hopkins School of Public Health in accordance with an assurance filed with and approved by the US Department of Health and Human Services.
Results
Table 1 summarizes the key implementation strategies and corresponding results of the BHI, and Table 2 depicts the timeline for key implementation activities
TABLE 1.
Breast Health Implementation Strategies and Key Interventions
| Breast Cancer Care Continuum (Health‐System Level) | Strategies |
Interventions |
|---|---|---|
|
Awareness/education (community level) |
|
|
|
Early detection/screening level (primary care) |
|
|
|
Diagnostic level (secondary or tertiary care) |
|
|
| Cross‐cutting |
|
|
Abbreviations: ANM, auxiliary nurse midwife; ASHA, accredited social health activist; CBE, clinical breast examination.
TABLE 2.
Timeline of Key Implementation Activities
| Activities | Year | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | ||||||||||||||||||||||
| April | May | June | July | August | September | October | November | December | January | February | March | April | May | June | July | August | September | October | November | December | January | February | March | |
| Situational assessment | ||||||||||||||||||||||||
| Breast Health Technical Advisory Committee | ||||||||||||||||||||||||
| Designing implementation strategy | ||||||||||||||||||||||||
| Facility assessment | ||||||||||||||||||||||||
| Training for health care providers | ||||||||||||||||||||||||
| Enumeration by ASHAs | ||||||||||||||||||||||||
| Supportive supervision | ||||||||||||||||||||||||
| Monthly feedback sharing with the facility | ||||||||||||||||||||||||
| Monthly progress reports | ||||||||||||||||||||||||
Abbreviations: ASHA, accredited social health activist.
Program Outreach
Overall, 108,112 women were contacted by ASHAs in the community for the breast health education, representing approximately 16% of target‐age women in program sites (Table 3). Forty‐eight percent (52,248 women) visited the health facilities for CBE, of which 1736 women (3%) had a positive CBE result, out of which 708 women (41%) visited a diagnostic facility. Of the latter, 423 women (60%) were confirmed to have a positive CBE result on repeat CBE by a medical officer or staff nurse, and 386 women (91%) underwent diagnostic evaluation. Twenty‐four women (8%) were ultimately confirmed to have breast cancer, and 19 women (79%) began treatment.
TABLE 3.
Summary of Results
| Women, No. | Women, % | Patients With a Suspicious Finding on CBE, % | |
|---|---|---|---|
| Contact in the community | 108,112 | 100 | Not applicable |
| Visited health facility for CBE | 52,248 | 48 | Not applicable |
| Suspicious finding on CBE referred to diagnostic facility | 1736 | 3.3 | 100 |
| Visited diagnostic facility | 708 | 41 | 40.8 |
| Suspicious finding on repeat CBE | 423 | 60 | 24.4 |
| Completed diagnostic evaluation | 386 | 91 | 22.2 |
| Confirmed diagnosis of cancer to date | 24 | 8 | 1.4 |
| Initiated treatment | 19 | 79 | 1.1 |
| Women with staging information available | 18 | 75 | 1.0 |
| Stage I and II | 13 | 72 | 0.7 |
| Stage III | 4 | 22 | 0.2 |
| Stage IV | 1 | 6 | 0.06 |
Abbreviations: CBE, clinical breast examination.
Training for Health Care Providers
Training effectiveness was assessed by pre‐ and post‐tests for knowledge of ASHAs, ANMs, staff nurses, and medical officers (multiple choice knowledge assessment tool) and the CBE skills of ANMs, staff nurses and medical officers (Objective Structured Clinical Examination [OSCE]). The mean knowledge scores improved from 69% to 93%, whereas mean CBE skills improved from 21% to 95%.
Quality of CBE
The concordance level of CBE findings between health care providers at the primary versus secondary levels of the health care system was high (94%) after initial training, and then it decreased in subsequent quarters to 45% to 50%. Based on facility‐level data for volume and quality of CBE performed, facilities were prioritized for supportive supervision visits to reinforce CBE skills in primary care. As such, the CBE concordance level increased to 78% in the final quarter of program implementation.
Adherence to Follow‐Up Care
Over the project implementation period from October 2018 to March 2020, a total of 708 women (41%) with a positive CBE result visited a diagnostic facility. During the first 3 months, adherence was only 14%; however, adherence quickly doubled (37%) and was maintained by the end of the reporting period (41%). Of the 423 women who visited a diagnostic facility and were confirmed to have a positive CBE result by the specialist, 386 (91%) completed diagnostic evaluation. Of those who completed diagnostic evaluation, 367 women underwent investigations without biopsy, whereas 19 women underwent a biopsy (Table 4). Of those who visited a diagnostic facility and were confirmed to have positive a CBE by the specialist, only 9% were not able to complete diagnostic evaluation.
TABLE 4.
Trend in Adherence of Patients with a CBE‐Positive Result to the Care Pathway
| Overall | Suspicious CBE Cases at Screening Facilities | Women With Suspicious CBE Result at a Screening Facility Who Visited a Diagnostic Facility, % (No.) | CBE Positive Cases at a Diagnostic Facility, No. | Women With a Confirmed CBE Positive Result at a Diagnostic Facility Who Completed a Diagnostic Evaluation, % (No.) | ||||
|---|---|---|---|---|---|---|---|---|
| Within 1 mo | >1 mo | Lost to Follow‐Up | Within 1 mo | >1 mo | Lost to Follow‐Up | |||
| Oct‐Dec 2018 | 201 | 14% (29) | 26% (53) | 59% (119) | 32 | 84% (27) | 6% (2) | 9% (3) |
| Jan‐Mar 2019 | 461 | 31% (142) | 10% (44) | 60% (275) | 122 | 66% (81) | 20% (25) | 13% (16) |
| Apr‐Jun 2019 | 488 | 37% (181) | 5% (25) | 58% (282) | 127 | 83% (106) | 10% (13) | 6% (8) |
| Jul‐Sep 2019 | 279 | 34% (96) | 6% (16) | 60% (167) | 62 | 82% (51) | 5% (3) | 13% (8) |
| Oct‐Dec 2019 | 178 | 35% (62) | 3% (5) | 62% (111) | 34 | 94% (32) | 3% (1) | 3% (1) |
| Jan‐Mar 2020 | 129 | 41% (53) | 2% (2) | 57% (74) | 46 | 91% (42) | 7% (3) | 2% (1) |
| Overall | 1736 | 32% (563) | 8% (145) | 59% (1028) | 423 | 80% (339) | 11% (47) | 9% (37) |
Abbreviations: CBE, clinical breast exam.
Average Time to Complete Diagnostic Evaluation
The average time to visit a diagnostic facility decreased from 12 to 5 days by the last quarter of the project. Of those women with a positive CBE result at a diagnostic facility, 80% completed a diagnostic evaluation within 1 month. The average time to complete a diagnostic evaluation without a biopsy remained unchanged, whereas the average time to a complete diagnostic evaluation with biopsy was reduced from 37 to 9 days.
Among women with a positive CBE result who underwent diagnostic evaluation, 91.2% underwent an ultrasound, 7.7% underwent an FNAB, and 1.1% underwent a mammogram. Among women who received an ultrasound, 68% underwent an ultrasound only, 20% underwent an ultrasound and an FNAB, 1.7% underwent an ultrasound, mammography, and an FNAB, and 1.3% underwent an ultrasound and mammography investigations. During the program implementation period, 75% of women with a positive CBE result underwent only 1 test, whereas 25% required more than 1 diagnostic test.
Breast Cancer Staging
We were able to collect staging details for 18 of the 24 women who were confirmed to have breast cancer. Of the 18 cases for which complete staging information was available, 13 (72%) were early stage (stage 1 and 2), 4 were locally advanced, and only 1 had metastatic disease (Table 3).
Discussion
During the first 18 months of implementation, we were able to reach 16% of the eligible population, 48% of which visited their nearby primary health care facility for CBE screening. We have observed that the quality of CBE and adherence to follow‐up care among women with abnormal CBE results improved considerably through the course of the program, with more women visiting the diagnostic facilities and completing diagnostic evaluation. We observed a significant decrease in the proportion of women lost to follow‐up; however, adherence remained low overall, with only 41% of women with a positive CBE result at primary care and reaching the next level of care for diagnostic evaluation. We also report a clinically meaningful decrease in time to complete diagnostic evaluation with biopsy from 37 to 9 days. Of the women in the program who were diagnosed with breast cancer, 72% had early‐stage disease, which compares favorably with the previously reported results. 5
Low screening uptake and adherence to the care pathway might have been affected by various factors including low awareness in the community regarding breast cancer screening, lack of trained providers, a fragmented health system, and poor coordination across levels of the health system. 14 , 15 , 16 The situational assessment 5 revealed low awareness about breast health among health care providers and women in the community, with more than 75% of patients with breast cancer reporting they had never undergone a CBE before their cancer diagnosis. 5 Furthermore, a pretest of knowledge and skills conducted before training initiation showed low knowledge (69%) and low CBE skills (21%) among health care providers. We attempted to address these issues with training for health care providers and implementing breast health awareness programming, including pragmatic information about breast screening in the BHI and for those with symptoms to seek timely diagnostics and treatment. Although we were not able to formally interview patients who did not receive diagnostic and tertiary care in our program, existing evidence suggests that adherence to care is influenced by geographic and health system barriers, cultural beliefs and misconceptions regarding breast cancer, competing priorities, and financial barriers. 5 , 17 , 18 Although it is beyond the scope of the current study, we estimated that approximately 40 patients with breast cancer could have been missed because of nonadherence to follow‐up care. It is also possible that some women sought follow‐up in the private sector for diagnostic evaluation and subsequent treatment. According to Rajpal and colleagues, 19 in 2014, 61% of patients with cancer in India used private facilities; this figure was higher for female patients. Moreover, visits to homeopathic practitioners and home remedies for treatment of a breast lump are common practice in both states. 5 Adherence to diagnostics did improve over the project implementation period, likely because of increased breast health awareness in the community and efforts to track patients in need of follow‐up. This implies the program was successful in ensuring timely completion of diagnosis.
Before the project implementation, more than 50% of patients delayed seeking care with a health care provider on average 4 to 5 months. 5 During the project implementation period, we observed a substantial decrease in the average time to visit a diagnostic facility and to complete diagnostic evaluation. This is an important metric because delays between the discovery of a clinically palpable breast finding and diagnosis of breast cancer are associated with significantly lower survival, 20 and the BHGI framework suggests a target of no more than 60 days from the detection of an abnormal breast finding. 21
Patient navigation has been shown to increase utilization and adherence to cancer screening services. 22 , 23 , 24 , 25 , 26 Although we attempted to implement frugal mechanisms for patient navigation that included reminder phone calls to patients in need of follow‐up, there is a need for further strengthening of these patient‐navigation systems.
Although the only modality currently recommended by the World Health Organization for population‐based breast cancer screening is mammography, 27 this comes with essential caveats, along with critical programmatic and technical requirements, all of which must be supported through sustainable financing. 27 , 28 As such, mammographic screening is recommended only in high‐resource settings with robust, well‐financed, and well‐coordinated health systems. 27 , 28 In lower‐resource settings, the WHO and the BHGI, 9 recently having joined forces in the Global Breast Cancer Initiative, 29 recommend that the first critical step in a phased approach to implementing breast health care is to ensure that all women with symptoms suggestive of breast cancer have equitable access to timely diagnosis and care, also called “early diagnosis.” Although early‐diagnosis strategies, including capacity building, are being implemented in India to ensure timely access to affordable diagnostic evaluation, the WHO advises consideration of using CBE as a screening modality for asymptomatic women at an appropriate target‐age range, in a more controlled setting, ideally with implementation research methods to evaluate processes and outcomes. 27
During the 18 months implementation process that we describe here, long‐term data were published from India by Mittra and colleagues 30 showed, for the first time in a high‐quality randomized control trial, a clinically meaningful (15%) reduction in breast cancer–specific mortality after screening by CBE. Although mortality was statistically significant only for women older than 50 years, there was a trend toward mortality reduction overall. According to the literature, 5 , 14 more than 50% of the patients presenting to a cancer specialist were in stages III and IV, whereas, after implementation of this breast cancer program, 72% of patients with breast cancer were diagnosed with early‐stage breast cancer. According to the Global Breast Cancer Initiative's recent estimates, countries with reduction in age‐standardized breast cancer mortality had at least 60% of patients with invasive breast cancer presenting as stage I or II disease at the population level. 31 Our program might be considered a related effort to demonstrate that a breast cancer screening program with CBE that incorporates community awareness and mobilization, primary care‐based screening, enhanced referral, and tracking processes in a resource‐constrained health system to facilitate timely diagnosis and treatment is feasible, and effective. The above findings seem to be consistent with experiences from several countries where the implementation of breast cancer awareness programming in conjunction with capacity building to increase equitable access to diagnosis and care, despite the absence of population‐based screening programs, has resulted in substantial decreases in average breast cancer stage at diagnosis, with steady declines in breast cancer mortality rates. 29 However, due to the relatively low age‐standardized incidence of breast cancer in rural India 2 and the early age at which screening for breast cancer is recommended in India's national strategy (ie, age 30 years in the NPCDCS), many more women would need to be screened and new cases detected in our program to demonstrate clinical downstaging.
We might also hypothesize that community‐based programming, education, and mobilization by ASHAs, along with quality CBE and patient navigation systems to ensure timely diagnosis and treatment, might have downstream impacts on future clinical downstaging for women who ultimately develop breast cancer, in India. This is supported by previous work by the BHGI 32 and a study conducted in Peru that reported women who underwent CBE were more likely to be diagnosed with an early stage of breast cancer. 33
Recommendations
To implement an evidence‐based, resource‐appropriate breast cancer program, we recommend the following:
Institutionalize creation of breast health awareness through the existing community‐based platforms.
Saturate the primary health care capacity to offer quality CBE and patient navigation services for breast cancer.
Implement incentives for frontline health workers to strengthen community mobilization and follow‐up of women with a positive CBE result.
Integrate breast cancer screening with existing primary health care system and national programs and schemes for better coordination and outreach.
Integrate technology solutions for decentralizing triaging and diagnostics (eg, portable ultrasound machine, telepathology) services to district‐level facilities.
Develop patient navigation strategies at all levels: community, screening, diagnostics, and treatment.
Implement robust data collection and management systems for enabling evidence‐based decision‐making at all levels.
Improve resource allocation for breast cancer care services.
In conclusion, results from the first 18 months of the BHI demonstrate the feasibility and effectiveness of implementing a large‐scale, decentralized, and context‐appropriate breast cancer early detection program in India. Breast health education, delivered through frontline health workers as a part of the routine home and community visits, can be an effective means for mobilizing women to the primary health care facilities for CBE. Our results demonstrate that it is feasible to build the capacity of primary‐level health care providers for conducting high‐quality CBEs. The increase in adherence over time, for women with an abnormal CBE visiting the diagnostic center, coupled with reductions in the time to final diagnosis and downstaging are suggestive of the effectiveness of the patient‐tracking and referral system. This is a very encouraging result, as early detection and diagnosis directly influence survival, provided that appropriate care is available and affordable. The strategic plan was codesigned with the respective state governments and the government of India, and conscious efforts were made to avoid the creation of a parallel, nonreplicable system.
Especially noteworthy is the finding that, during the rollout of this plan, existing resources and platforms were used to integrate the care pathway within the ongoing primary health care system, which will facilitate both its scalability and its sustainability.
Funding Support
This project was funded by Johns Hopkins University.
Conflict of Interest Disclosures
The authors made no disclosures.
Author Contributions
Somesh Kumar: Conceptualization, methodology, project administration, supervision, writing–original draft, and review and editing. Gulnoza Usmanova: Conceptualization, analysis, methodology, writing–original draft, and review and editing. Tapas Sadasivan Nair: Analysis, writing–original draft, review, and literature search. Vineet Kumar Srivastava: Conceptualization, project administration, supervision, writing–original draft, and literature search. Rakesh Singh: Analysis, data management, and literature search. Nochiketa Mohanty: Conceptualization, analysis, methodology, literature search, and writing–review and editing. Nadeem Akhtar: Project administration, writing–original draft, and literature search. Meshach Sunny Kujur: Project administration, writing–original draft, and literature search Ashish Kumar Srivastava: Project administration, supervision, writing–original draft, and literature search. Suranjeen Prasad Pallipamula: Conceptualization, writing–original draft, and literature search. Gaurav Agarwal: Conceptualization and review and editing. Amresh Bahadur Singh: Conceptualization and review and editing. Vivek Kashyap: Review and editing. Maura McCarthy: Literature review and writing–review and editing. Erica J. Liebermann: Conceptualization, writing–original draft, and review and editing. Ophira Ginsburg: Conceptualization and writing–review and editing.
Supporting information
Fig S1
Kumar S, Usmanova G, Nair TS, Srivastava VK, Singh R, Mohanty N, Akhtar N, Kujur MS, Srivastava AK, Pallipamula SP, Agarwal G, Singh AB, Kashyap V, McCarthy M, Liebermann EJ, Ginsburg O. Implementation of a large‐scale breast cancer early detection program in a resource‐constrained setting: real‐world experiences from 2 large states in India. Cancer. 2022. 10.1002/cncr.34114
The first two authors contributed equally to this article.
The last two authors contributed equally to this article.
We thank the governments of Uttar Pradesh and Jharkhand for their leadership and overwhelming support in performing this program. We also thank Johns Hopkins University for its generous funding.
Tapas Sadasivan Nair's current address: World Health Organization, Geneva, Switzerland.
Ashish Kumar Srivastava's current address: Norway India Partnership Initiative, New Delhi, India.
Erica J. Lieberman's current address: University of Rhode Island, College of Nursing, Providence, Rhode Island.
Ophira Ginsburg's current address: International Agency for Research on Cancer, Lyon France.
References
- 1. Mathur P, Sathishkumar K, Chaturvedi M, et al. Cancer Statistics, 2020: report from National Cancer Registry Programme, India. JCO Glob Oncol. 2020;6:1063‐1075. doi: 10.1200/GO.20.00122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. International Agency for Research on Cancer. Published 2020. Accessed June 1, 2021. https://gco.iarc.fr/today [Google Scholar]
- 3. Sathwara J, Bobdey S, Ganesh B. Breast cancer survival studies in India: a review. Int J Res Med Sci. 2017;4:7. doi: 10.18203/2320-6012.ijrms20162266 [DOI] [Google Scholar]
- 4. Somanna SN, Nandagudi Srinivasa M, Chaluvarayaswamy R, Malila N. Time interval between self‐detection of symptoms to treatment of breast cancer. APJCP. 2020;21:169‐174. doi: 10.31557/APJCP.2020.21.1.169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kumar S, Srivastava A, Srivastava AK, et al. Designing a resource‐stratified, phased implementation strategy for breast health care services in India. Cancer. 2020;126:2458‐2468. [DOI] [PubMed] [Google Scholar]
- 6. Malvia S, Bagadi SA, Dubey US, Saxena S. Epidemiology of breast cancer in Indian women. Asia Pac J Clin Oncol. 2017;13:289‐295. [DOI] [PubMed] [Google Scholar]
- 7. National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases & Stroke: Operational Guidelines. Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India. Accessed June 1, 2021. https://main.mohfw.gov.in/sites/default/files/Operational%20Guidelines%20of%20NPCDCS%20%28Revised%20‐%202013‐17%29_1.pdf
- 8. Anderson BO, Carlson RW. Guidelines for improving breast health care in limited resource countries: the Breast Health Global Initiative. JNCCN. 2007;5:349‐356. doi: 10.6004/jnccn.2007.0031 [DOI] [PubMed] [Google Scholar]
- 9. Anderson BO, Yip CH, Smith RA, et al. Guideline implementation for breast healthcare in low‐income and middle‐income countries: overview of the Breast Health Global Initiative Global Summit 2007. Cancer. 2008;113(8 suppl):2221‐2243. [DOI] [PubMed] [Google Scholar]
- 10. Breast Health Global Initiative . BCI2.5 toolkits for breast health assessment. Fred Hutchinson Cancer Research Center. Accessed June 5, 2021. https://www.fredhutch.org/en/research/divisions/public‐health‐sciences‐division/research/epidemiology/breast‐cancer‐initiative‐2‐5.html [Google Scholar]
- 11. Office of the Registrar General & Census Commissioner India . Census of India. Accessed June 10, 2021. https://www.censusindia.gov.in/2011‐prov‐results/prov_results_paper1_india.html
- 12. Awasthi A, Pandey CM, Chauhan RK, Singh U. Disparity in maternal, newborn and child health services in high focus states in India: a district‐level cross‐sectional analysis. BMJ Open. 2016;6:e009885. doi: 10.1136/bmjopen-2015-009885 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Indian Council of Medical Research, Public Health Foundation of India, and Institute for Health Metrics and Evaluation . GBD India Compare. Accessed June 11, 2021. https://vizhub.healthdata.org/gbd‐compare/india
- 14. Ainapure K, Sumit K, Pattanshetty S. A study on implementation of national programme for prevention and control of cancer, diabetes, cardiovascular diseases and stroke in Udupi district, Karnataka. IJCMPH. 2018;5:2384‐2387. [Google Scholar]
- 15. Kashyap V, Shivaswamy M. Assessment of implementation of the national programme for the prevention and control of cancer, diabetes, cardiovascular diseases, and stroke at subcenters of Belagavi taluka: a cross‐sectional study. Ind J Health Sci Biomed Res. 2019;12:21‐27. doi: 10.4103/kleuhsj.kleuhsj_232_18 [DOI] [Google Scholar]
- 16. Modi B, Pranay J, Vasoya N. Evaluation of National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular disease and Stroke (NPCDCS) in Gandhinagar district, Gujarat. Healthline J. 2019;10:33‐38. [Google Scholar]
- 17. Breast Cancer Initiative 2.5 . Improving access to breast cancer care. Fred Hutchinson Research Cancer Center. Accessed July 20, 2021. https://www.fredhutch.org/content/dam/www/research/divisions/public‐health‐sciences/epidemiology/bci‐25/KSPDF/KS%20Planning%20Access%20030617.pdf [Google Scholar]
- 18. Sharma K, Costas A, Shulman LN, Meara JG. A systematic review of barriers to breast cancer care in developing countries resulting in delayed patient presentation. J Oncol. 2012;2012:121873. doi: 10.1155/2012/121873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Rajpal S, Kumar A, Joe W. Economic burden of cancer in India: evidence from cross‐sectional nationally representative household survey, 2014. PLoS One. 2018;13:1‐17. doi: 10.1371/journal.pone.0193320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Richards MA, Westcombe AM, Love SB, Littlejohns P, Ramirez AJ. Influence of delay on survival in patients with breast cancer: a systematic review. Lancet. 1999;353:1119‐1126. doi: 10.1016/S0140-6736(99)02143-1 [DOI] [PubMed] [Google Scholar]
- 21. Duggan C, Dvaladze A, Rositch AF, et al. The Breast Health Global Initiative 2018 Global Summit on Improving Breast Healthcare Through Resource‐Stratified Phased Implementation: methods and overview. Cancer. 2020;126:2339‐2352. doi: 10.1002/cncr.32891 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Dalton M, Holzman E, Erwin E, et al. Patient navigation services for cancer care in low‐and middle‐income countries: a scoping review. PLoS One. 2019;14:e0223537. doi: 10.1371/journal.pone.0223537 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Freeman HP. The origin, evolution, and principles of patient navigation cancer epidemiology biomarkers and prevention. Cancer Epidemiol Biomarkers Prev. 2012;21:1614‐1617. doi: 10.1158/1055-9965.Epi-12-0982 [DOI] [PubMed] [Google Scholar]
- 24. Freund KM, Battaglia TA, Calhoun E, et al. Impact of patient navigation on timely cancer care: the patient navigation research program. J Natl Cancer Inst. 2014;106:dju115. doi: 10.1093/jnci/dju115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Young AM, Charalambous A, Owen RI, et al. Essential oncology nursing care along the cancer continuum. Lancet Oncol. 2020;21:e555‐e563. doi: 10.1016/S1470-2045(20)30612-4 [DOI] [PubMed] [Google Scholar]
- 26. Wild C, Weiderpass E, Stewart BW. World Cancer Report: Cancer Research for Cancer Prevention. IARC Press; 2020. [Google Scholar]
- 27. WHO Position Paper on Mammography Screening. World Health Organization; 2014. [PubMed] [Google Scholar]
- 28. International Agency for Research on Cancer . IARC Handbooks of Cancer Prevention. Oxford University Press; 1997. [Google Scholar]
- 29. Anderson BO, Ilbawi AM, Fidarova E, et al. The Global Breast Cancer Initiative: a strategic collaboration to strengthen health care for noncommunicable diseases. Lancet Oncol. 2021;22:578‐581. doi: 10.1016/S1470-2045(21)00071-1 [DOI] [PubMed] [Google Scholar]
- 30. Mittra I, Mishra GA, Dikshit RP, et al. Effect of screening by clinical breast examination on breast cancer incidence and mortality after 20 years: prospective, cluster randomised controlled trial in Mumbai. BMJ. 2021;372:n256. doi: 10.1136/bmj.n256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Duggan C, Trapani D, Ilbawi AM, et al. National health system characteristics, breast cancer stage at diagnosis, and breast cancer mortality: a population‐based analysis. Lancet Oncol. 2021;22:P1632‐P1642. doi: 10.1016/S1470-2045(21)00462-9 [DOI] [PubMed] [Google Scholar]
- 32. Ginsburg O, Yip C‐H, Brooks A, et al. Breast cancer early detection: a phased approach to implementation. Cancer. 2020;126(suppl 10):2379‐2393. doi: 10.1002/cncr.32887 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Romanoff A, Constant TH, Johnson KM, et al. Association of previous clinical breast examination with reduced delays and earlier‐stage breast cancer diagnosis among women in Peru. JAMA Oncol. 2017;3:1563‐1567. doi: 10.1001/jamaoncol.2017.1023 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig S1